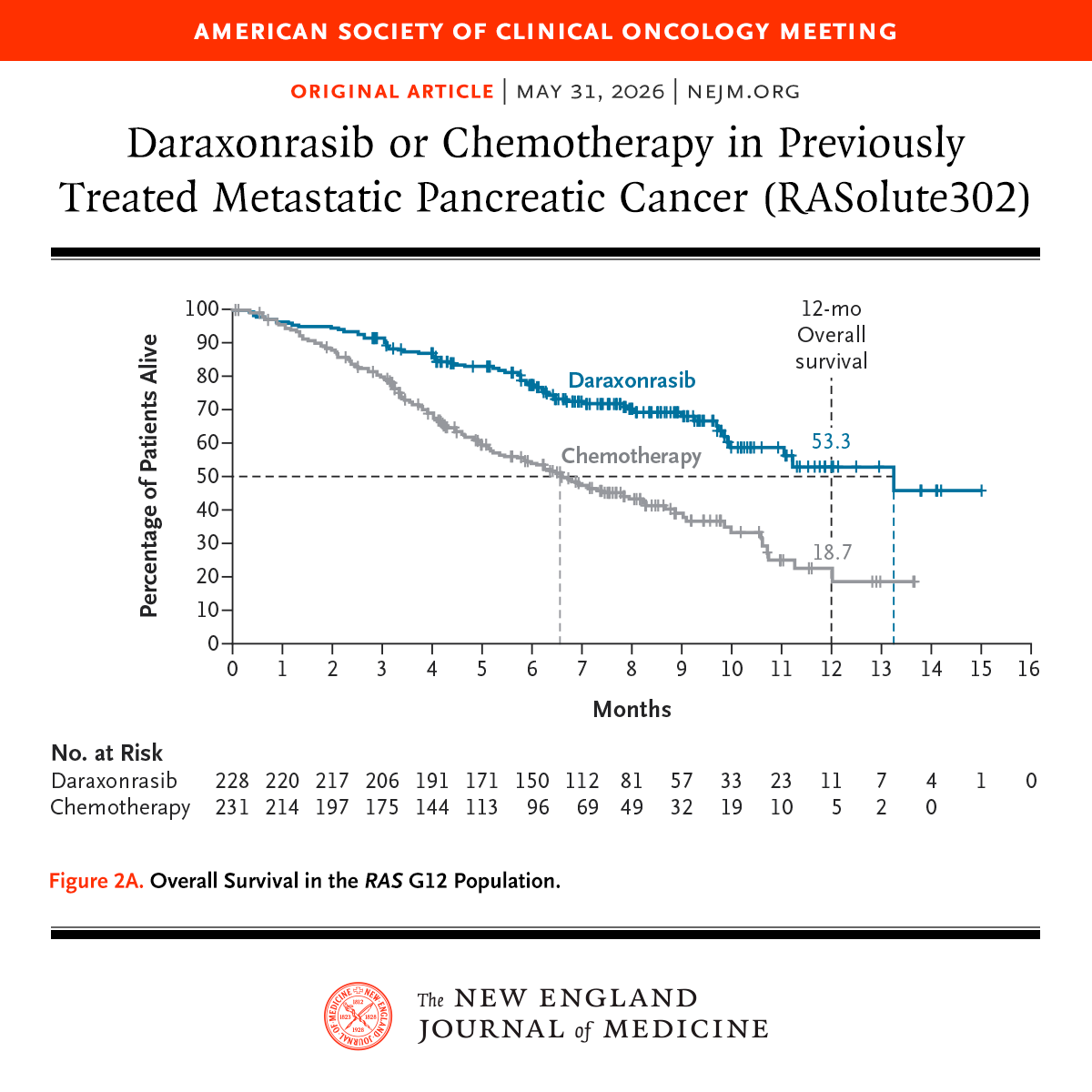
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
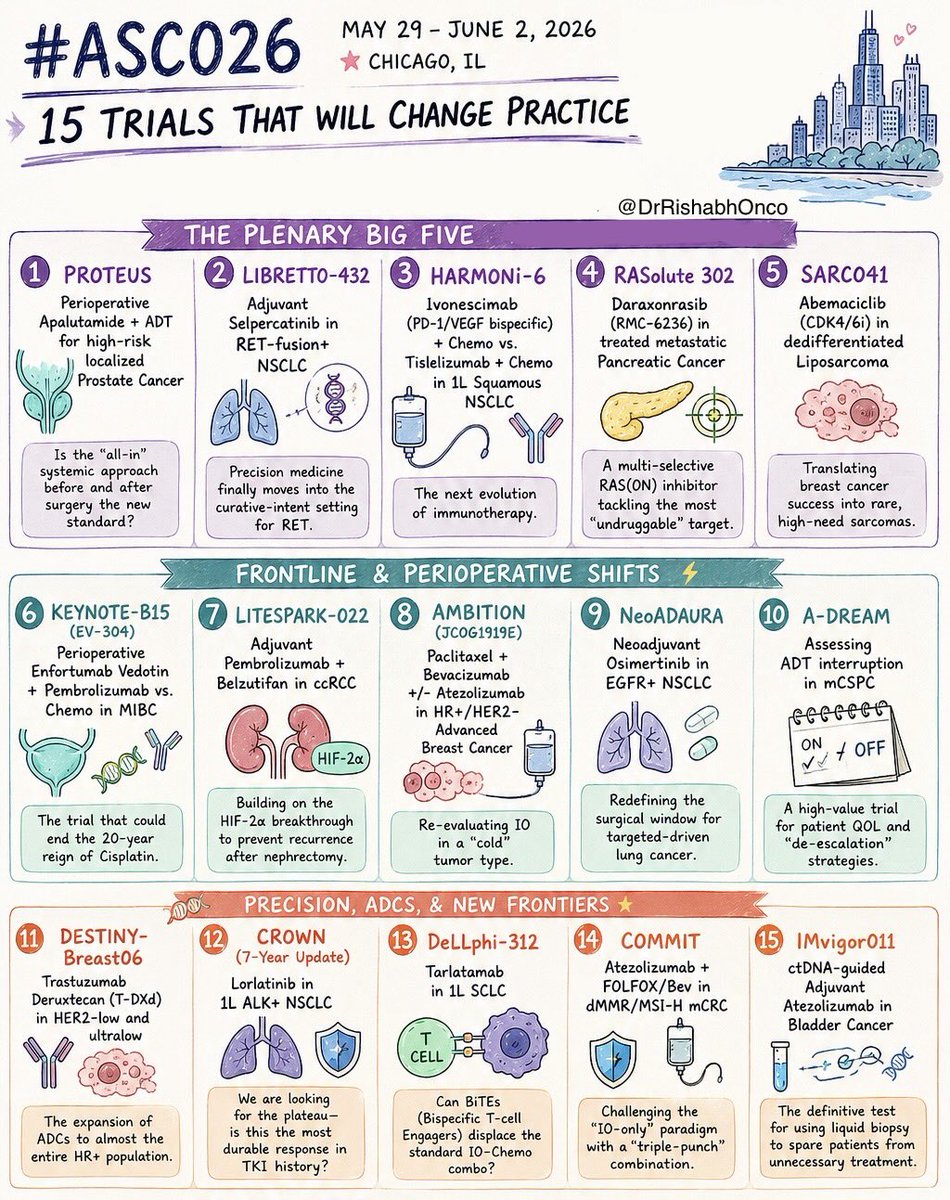
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26
May 29 - June 2 | Chicago
Which trial are you watching most closely?
🌟 PLENARY GAME-CHANGERS
1️⃣ PROTEUS
Perioperative apalutamide + ADT in high-risk localized prostate cancer
2️⃣ LIBRETTO-432
Adjuvant selpercatinib in RET+ NSCLC
3️⃣ HARMONi-6
Ivonescimab + chemo vs tislelizumab + chemo in squamous NSCLC
4️⃣ RASolute 302
Daraxonrasib (RMC-6236) in metastatic pancreatic cancer
5️⃣ SARC041
Abemaciclib in dedifferentiated liposarcoma
⚡ FRONTLINE & PERIOPERATIVE SHIFTS
6️⃣ KEYNOTE-B15 / EV-304
EV + pembrolizumab vs chemo in MIBC
7️⃣ LITESPARK-022
Pembrolizumab + belzutifan in adjuvant ccRCC
8️⃣ AMBITION
Paclitaxel/bevacizumab ± atezolizumab in HR+ breast cancer
9️⃣ NeoADAURA
Neoadjuvant osimertinib in EGFR+ NSCLC
🔟 A-DREAM
ADT interruption strategies in mCSPC
🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY
1️⃣1️⃣ DESTINY-Breast06
T-DXd expands into HER2-ultralow disease
1️⃣2️⃣ CROWN (7-year update)
Lorlatinib durability in ALK+ NSCLC
1️⃣3️⃣ DeLLphi-312
Tarlatamab in frontline SCLC
1️⃣4️⃣ COMMIT
Atezolizumab + FOLFOX/Bev in MSI-H mCRC
1️⃣5️⃣ IMvigor011
ctDNA-guided adjuvant atezolizumab in bladder cancer
#OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert@ASCO@JCOPO_ASCO@OncBrothers
🫀 Why do some patients crash on trastuzumab… and others don’t?
👉 Not just anthracyclines 💉
👉 Not just age 🎂
👉 Host genomics? 🧬
New JAMA Oncology data highlight CHIP as a key risk factor
Study snapshot 🧪
15,729 patients (UK Biobank) 🇬🇧
454 trastuzumab cohort 🏥
•mouse model 🐭
Key signal 📊
📈 2-year cardiotoxicity (CHIP vs no CHIP):
ESC: 15.7% vs 5.0%
Canadian: 19.9% vs 10.8%
CREC: 20.9% vs 11.3%
👉 Adjusted risk: sHR 1.91 📌
👉 CHIP + trastuzumab → ~4.5× HF risk ⚠️
Biology fits 🔬
Tet2-deficient mice 🐭 → ↓LVEF with trastuzumab 📉
Takeaway 🎯
🧬 CHIP may help identify high-risk patients
⚠️ Not practice-changing yet
💡 Toxicity = drug 💊 × host biology 🧬
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #BreastCancer #CardioOncology
@OncoAlert@myesmo@esmo_open@asco@JAMAOnc
#ESMORareCancers26: Preliminary data with the DR5 agonist, ozekibart, added to chemotherapy indicate robust activity and a manageable safety profile in relapsed/refractory #EwingSarcoma.
Learn more➡️ https://t.co/0Rqz7e2Cz4
#ESMODailyReporter
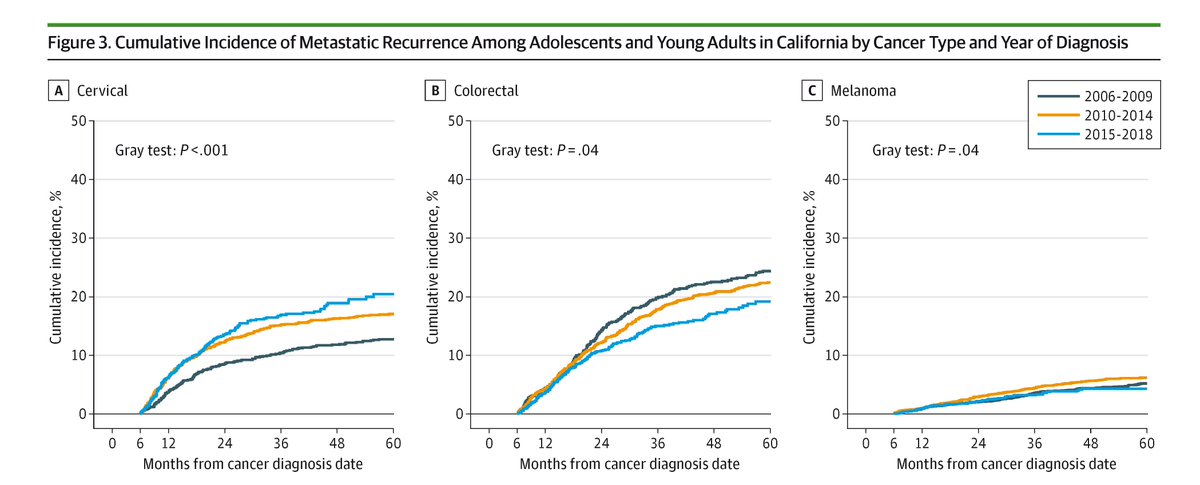
Among adolescents and young adults with #cancer, 9.5% of patients with earlier-stage cancer experienced metastatic recurrence within five years, with the highest rates in sarcoma (24.5%) and colorectal cancer (21.8%).
https://t.co/RS85GuKpr6
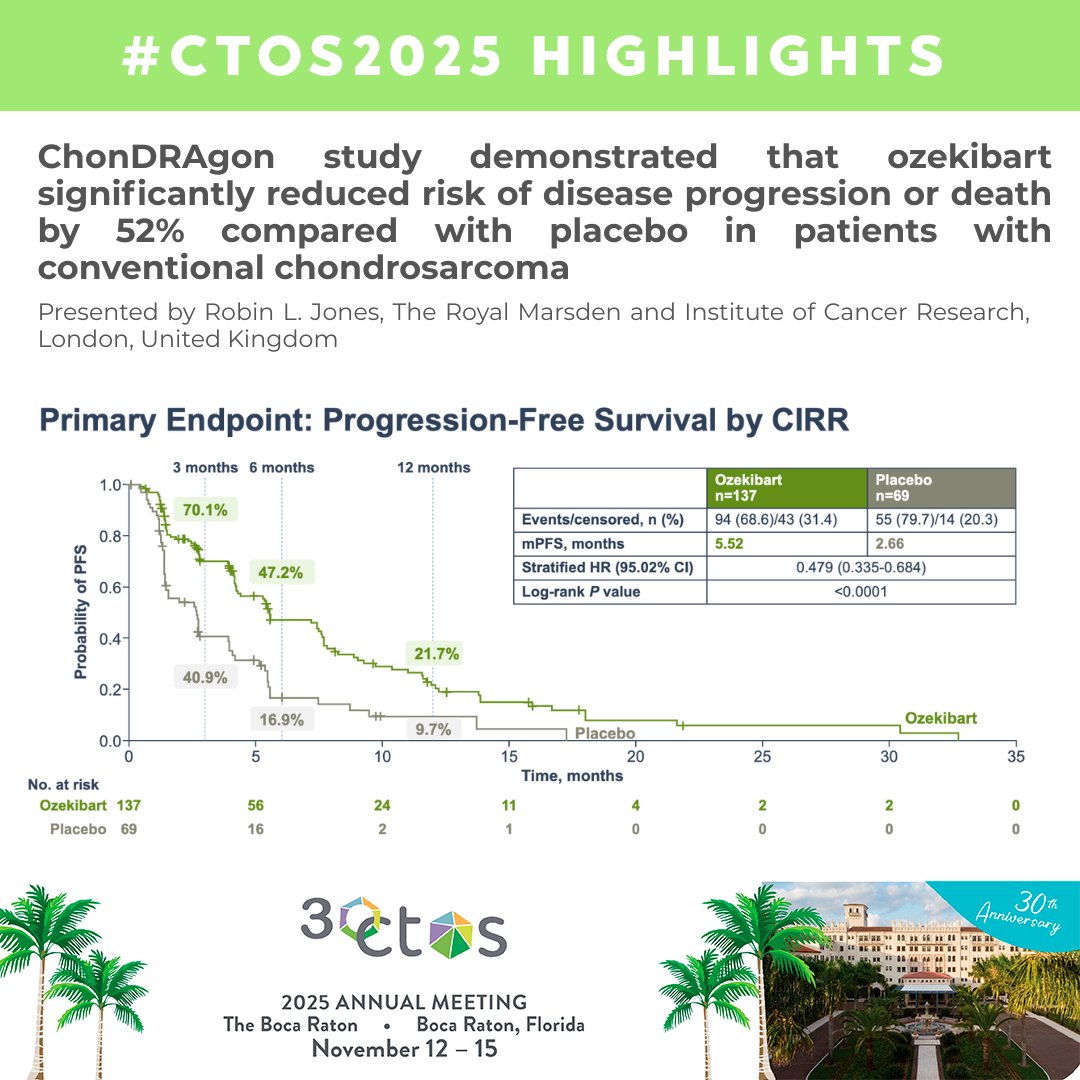
🚨Historical presentation at #CTOS2025
ChonDRAgon - first positive randomised trial in chondrosarcoma
🔹Ozekibart vs placebo
🔹 mPFS 5.52 vs 2.66 months
🔹 HR 0.479; p<0.0001
🔹 a manageable safety profile - most common TRAE: fatigue, diarrhea, and nausea
Men with PSA <1–2 ng/ml at 60 are very unlikely to die from prostate cancer. Screening them again may just cause harm, not help.
#ProstateCancer@JNCI_Now@APCCC_Lugano@PCFnews
https://t.co/ky2BoM6HJz
Why 30%↓ vs 20%↑ in RECIST?
🔹 WHO (1981) set them differently:
• Shrinkage (PR = 50% area ↓ → ~30% 1D) → high bar to avoid false positives (be sure a drug really shrinks tumors).
• Growth (PD = 25% area ↑ → ~12% 1D) → lower bar to catch progression early.
🔹 RECIST
👉 The 30% shrinkage comes straight from math:
WHO (1981) used 50% ↓ in tumor area → when converted to 1D, that’s ~30% ↓ in diameter.
👉 The 20% growth wasn’t pure math.
WHO’s 25% ↑ in area = ~12% ↑ in 1D… but that risked calling progression too early (measurement error).
So the RECIST task force chose 20% ↑ as a safer, reproducible cutoff.
💡 In short: 30% = math, 20% = pragmatism ✅
#OncoTwitter #MedTwitter #ColorectalCancer #Immunotherapy
@OncoAlert@myesmo@asco
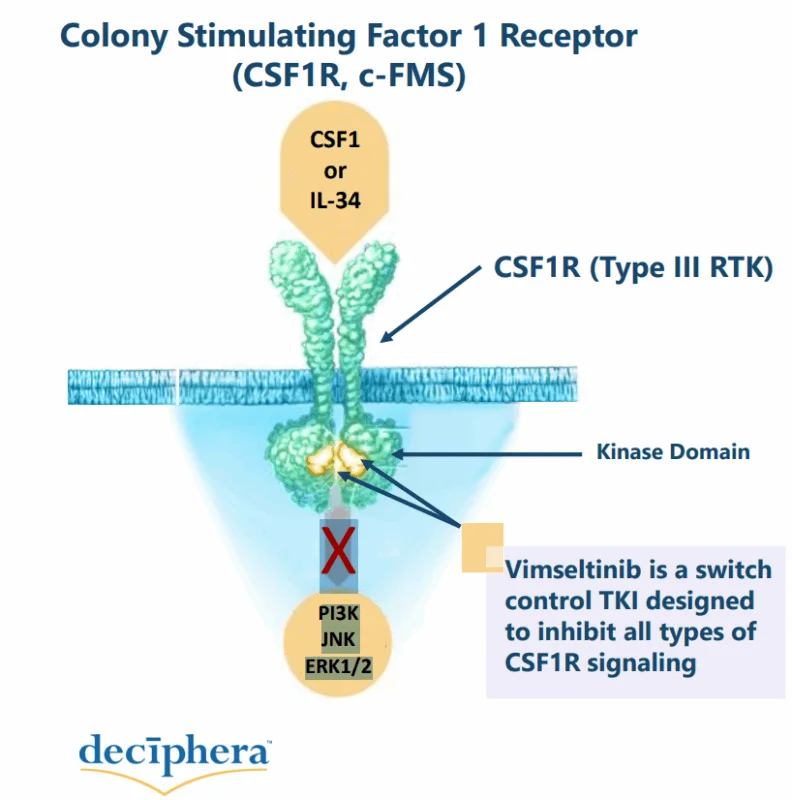
✍️Phase 3 MOTION trial in #TGCT: Vimseltinib vs placebo
-RECIST 40% ORR
-Tumor Volume Score 67% ORR
-Clinically meaningful Improvement
-Well tolerated and manageable adverse events
➡️ Vimseltinib is a well-deserved standard of care
#ESMO24#ESMOAmbassadors
🚨 New therapy approved in #sarcoma!
@EMA_News has granted the use of 🎯CSFR1 #vimseltinib in patients with #TGCT with funtion deterioration and in whom surgical options have been exhausted or would induce unacceptable morbidity or disability
▶️https://t.co/t4ASfzJDJo
🔥🚨@OncoAlert Hot off the press.
Just published @NEJM#OverallSurvival Results of:
⭐️#MARIPOSA Study of:
#Amivantamab plus #Lazertinib vs #Osimertinib in 1st line #Treatment of #EGFR+ Advanced Non-Small Cell #LungCancer.
Reminder that we have now two excellent (but different) combination regimens:
✅ #Amivantamab + #Lazertinib (#MARIPOSA)
✅ #Osimertinib + #Chemotherapy
(#FLAURA2) with #OS data just presented @IASLC #WCLC25
👇🏻
https://t.co/bcWXooSYix
Long-awaited OS results from #FLAURA2 (1L chemo + osimertinib vs osi):
-mOS: 47.5 vs 37.6 mo (HR 0.77)
-Benefit consistent across subgroups
-Longer osimertinib exposure with combo
Strong evidence supporting osi+chemo for newly diagnosed EGFR+ NSCLC.
#WCLC2025
De-escalated adjuvant radiotherapy versus standard adjuvant treatment for human papillomavirus-associated oropharyngeal squamous cell carcinoma (MC1675): a phase 3, open-label, randomised controlled trial - The Lancet Oncology https://t.co/RBAraRkmW4