Tired of always speculating about MR spectroscopy?
If you've ever looked at an MR spectroscopy & thought: "I have no idea what I’m looking at!"--then this cheat sheet is for you!
Here are the 4 basic rules you need so you can understand the spectrum of basic spectroscopy!
First you need to know the peaks.
3 main peaks: Choline, Creatine, NAA
Remember the order bc a spectrum looks like mountain peaks & it is cold in the mountains. And CHOld CREATures NAp or hibernate in the mountains
Choline
Marker of membrane turnover
Remember: membranes coat or “CHOat” the cell
Choline = ChoLEAN, choline LEANS into the creatine peak, it’s right next to it
Creatine
Marker of energy, basically an internal control
Remember, everyone takes Creatine powder for energy!
Creatine is at ~3—creatine almost rhymes with 3
NAA Marker of neuronal health
N = Neuron
NAA has double As so it is at ~2!
Four rules:
1. Hunter’s angle:
—Most people know that the peaks of the spectrum should go up at you move lateral, called Hunter’s angle
—Most bad things reverse Hunter’s angle
—Ask yourself: Is my arrow pointed up to shoot into the air at the enemy (good) or is point to the ground where it will hit the dirt (bad)
2. TE & spectrum length are inversely related
—Spectroscopy follows the rule: speak softly & carry a big stick.
—Short TE = long spectrum, lots of extra peaks for glutamate/glycine, myoinsitol
—Long TE = short spectrum, mainly the basic 3 peaks
3. Each region has its own unique signature
—Each brain region has its own unique composition of compounds that might alter Hunter’s angle a bit, but not reverse it
—Need a control in contralateral normal brain so compare apples to apples
4. Lactate peak goes like a sine wave
—Lactate peak represents anerobic metabolism—sign of cells in trouble
It’s at 1.3ppm. Remember this bc 13 is an unlucky number & lactate is an unlucky sign!
—It’s like a sine wave: up at short TE (35), down at intermediate TE (144), and up again at long TE (244)
—You can use this flipping to better visualize the lactate peak
—You can remember it’s down in the middle TE bc when you’re caught in the middle, you’re down & out
Just remember these tricks & you will be spectacular at basic spectroscopy!
Sink or swim!
Brain is swimming in CSF!
CSF is key for protection, buoyancy, & hormone/waste transport
Most know basic ventricular anatomy well, but not subarachnoid anatomy.
How many cisterns do YOU know?
Here’s a quick guide to the key midline cisterns & what to know for each
—Cisterna Magna:
Largest of the cisterns
Contains CN 9-11 & vertebral arteries
Remember this bc the LARGEST cistern contains the LARGEST cranial nerve (vagus) and the two cranial nerves around it
—Prepontine cistern:
Contains CN 6 & basilar artery
Remember this bc the shape of the number 6 mirrors the curvature of the anterior pons, where this cistern lies
—Chiasmatic cistern
Contains CN 2 & pituitary stalk
Easy to remember bc the CHIASM is CN 2
—Interpeduncular cistern:
Contains CN 3 & mammillary bodies
Remember this bc if you lay the number 3 on its side it looks both like the two cerebral peduncles (where this cistern lies) & well, two mamillary bodies
—Quadrigeminal cistern
Contains CN4 & pineal gland
East to remember bc QUAD is the prefix for FOUR
—Lamina terminalis:
Contains the ACOMM
Remember this bc the shape of subarachnoid hemorrhage after ACOMM rupture follows this cistern anteriorly
Now when you look at cisternal anatomy, you will definitely be able to go with the flow!
1/Time to go with the flow!
Hoping no one notices you don’t know the anatomy of internal carotid (ICA)?
Do you say “carotid siphon” & hope no one asks for more detail?
Here’s a thread to help you siphon off some information about ICA anatomy!
Listen up!
Trying to get into a rhythm on how to approach pulsatile tinnitus?
Does pulsatile tinnitus get your heart racing?
This week’s @theAJNR SCANtastic has all you need to know!
https://t.co/BTI94N5Wsk
Pulsatile tinnitus is caused by turbulent blood around the petrous bone!
It’s like traffic: if you alter the flow of traffic, you will start to hear some noise & horns!
So what causes turbulent traffic?
1. Complex traffic patterns
If the roads are crazy, people get confused and drive crazy. Same w/flow from:
--AVMs
--dAVFs
--Tumors
--Diverticula
2. Diverted traffic
Nothing causes more chaos than making people go a different way than normal. Variant flow anatomy can cause pulsatile tinnitus:
--Large mastoid emissary veins
--Large occipital sinus.
3. Blockage of traffic!
If there is an accident, there is turbulence as people try to get around. For flow, blockages are stenoses:
--Carotid stenosis
--Transverse/sigmoid sinus stenosis
--Jugular stenosis
In this month’s @theAJNR, Zhang et al. found jugular stenoses were equally prevalent in both controls & pts w/pulsatile tinnitus
It raises the question if should we treat jugular stenosis!
Now hopefully your heart won’t skip a beat when you see a case of pulsatile tinnitus!
Follow @theAJNR and check it out for yourself:
https://t.co/BTI94N5Wsk
1/Does your ability to remember temporal lobe anatomy seem, well, temporary?
Or are you feeling temporally challenged when it comes to this complex region?
Here’s a thread to help you remember the structures of the temporal lobe!
My attending once said, “If you don’t want to miss something, you have to know where look for it!”
Intracranial aneurysms may occur at many locations, but overwhelming at the ACOM & PCOMM. Look hard at these regions!
Remember, you miss 100% of aneurysms you don't look for!
Remember these two regions by always saying to yourself before you sign off any angiogram report:
"Always Please Communicate Aneurysms!"
Always = Anterior
Please = Posterior
Communicate = Communicating
Hopefully this will rupture any misconceptions about where to look for aneurysms!
Can you get the diagnosis when it comes to carotid stenosis?
Having some confusion about the strokes you see w/ICA occlusion?
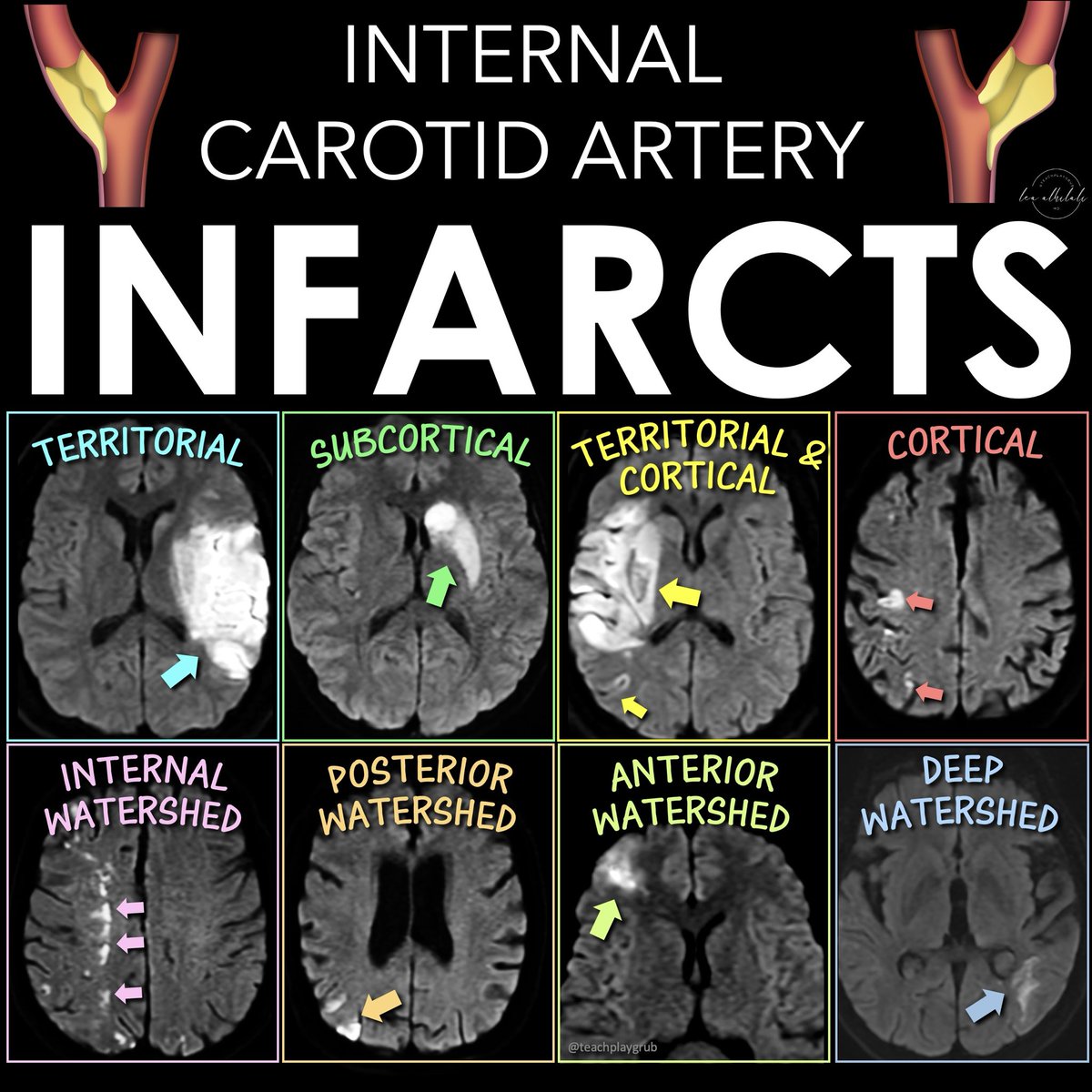
Why are there so many different patterns of infarcts w/ICA occlusion/stenosis?
There are 5 main infarct patterns—and they reflect the different types of disruption to flow you get w/carotid disease: artery to artery emboli, embolic shower, & hypoperfusion
Here’s what you see:
1. Territorial infarction w/cortical or subcortical involvement
--From artery-to-artery or distal embolism.
--More than one occlusion indicates more proximal arterial dz
2. Subcortical infarction
--When ICA, MCA, & ACA perforating deep arteries are occluded
--Can be from MCA occlusion w/good collaterals or emboli directly to deep perforating arteries
3. Combined territorial & smaller cortical and/or subcortical infarcts
--From partial embolism fragmentation or emboli shower of various sizes
4. Multiple small infarcts in the distal territories of the MCA & ACA
--If in more than one arterial territory, it’s suggestive of cardio-embolism
--If single arterial territory, it’s from a parent artery steno-occlusive lesion
5. Watershed infarctions.
Two types:
--External border-zone (located between the cortical territories of ACA, MCA, & PCA)
--Internal borderzone (between the deep & superficial networks of MCA & ACA)
--Traditionally thought from low-flow, but emboli are often a cause
--Hemodynamic mechanism may be more important in internal borderzone infarcts & embolism in external borderzone infarcts
Now you can draw the right conclusions with ICA occlusions!
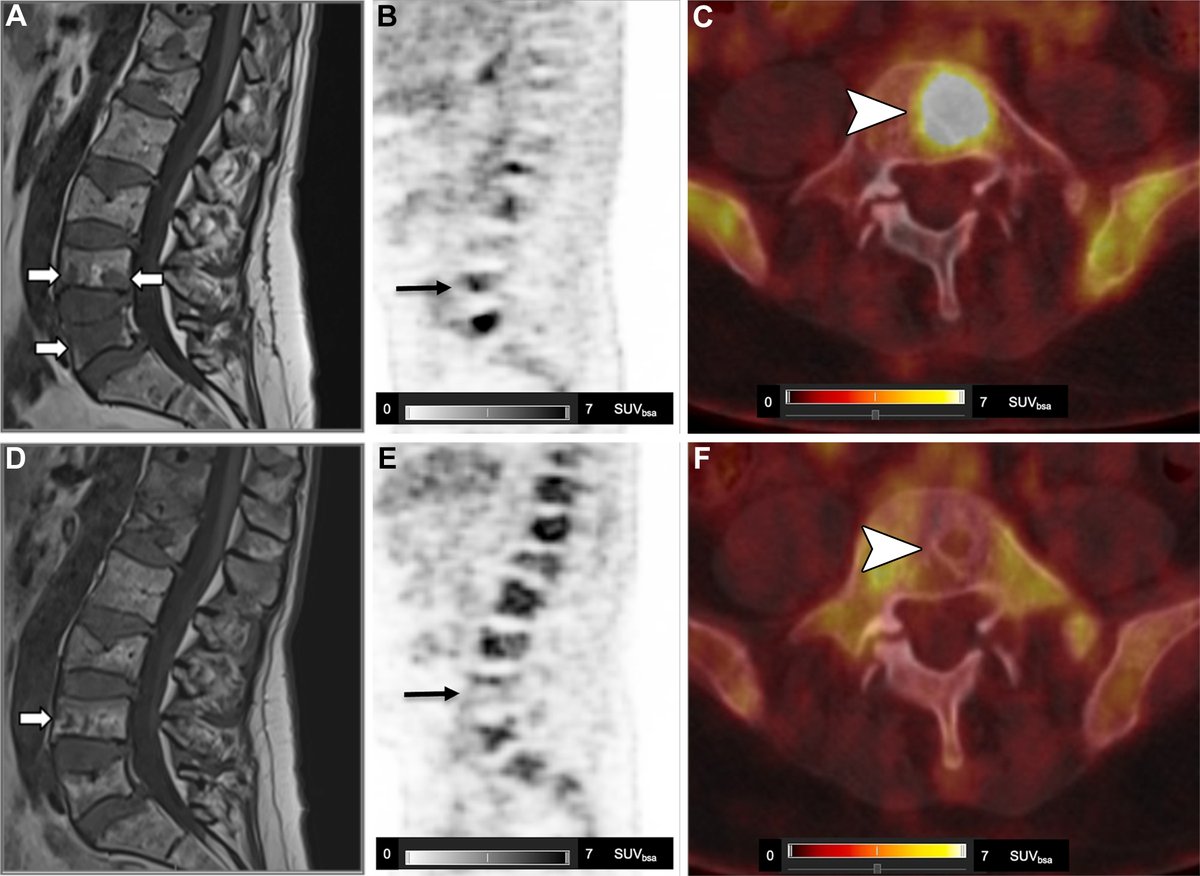
WB-DW MRI or FDG PET/CT for myeloma response? This review breaks down strengths, pitfalls, and standardized criteria (MY-RADS & Deauville). Learn how to integrate both for accurate posttreatment assessment and improved confidence. https://t.co/PweymUwoFZ
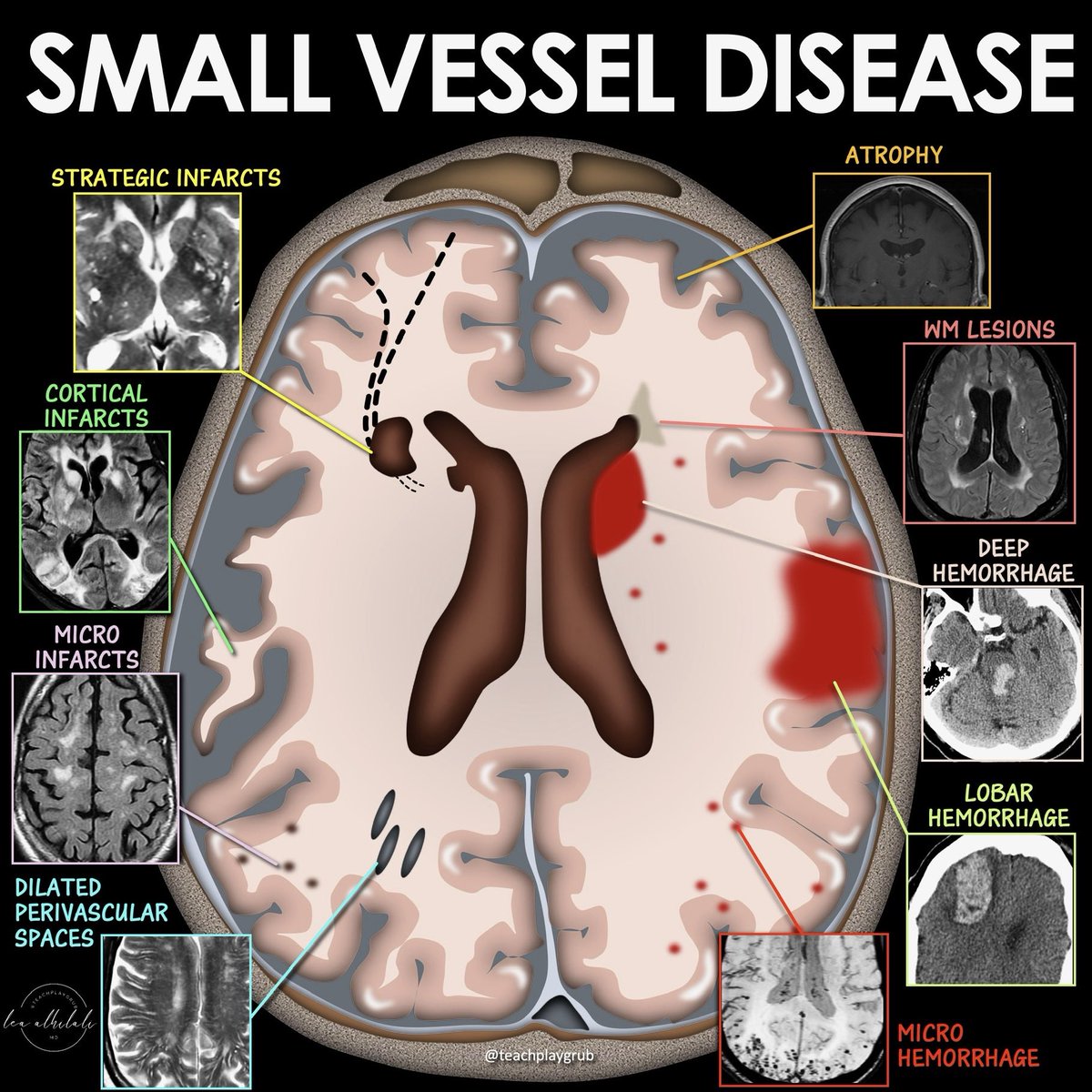
Just because it’s called SMALL vessel disease doesn’t mean it doesn’t have a BIG impact!
Small vessel disease (SVD) is a BIG contributor to vascular dementia, along w/large vessel cortical infarcts
Do YOU know all the faces of small vessel disease?
Common imaging markers of SVD include:
--White matter hyperintensities (WMHs)
--Lacunes
--Enlarged perivascular spaces
--Microbleeds
--Small subcortical infarcts
--Brain atrophy
But what you see isn’t always what you get!
Even in patients w/similar degrees of SVD, clinical symptoms can be very variable.
Variability exists because of:
--Perilesional penumbra
--Remote effects from disruption of brain connectivity
--Differing brain reserve & compensatory mechanisms
So remember, imaging findings of SMALL vessel disease are just the tip of a very BIG iceberg
From the October-December 2025 Issue of #Neurographics: Pictorial Review of Cerebral Venous Thrombosis with Emphasis on Diagnostic Clues and Radiological Patterns
https://t.co/bBlfFfCopl
Most patients with CSF pressure disorders don’t read the textbook.
This review is about what to do when the imaging, symptoms, and physiology don’t line up, and why “high” vs “low” pressure is often the wrong framework.
🔓Open access:
https://t.co/YnLJG2asav
Emerging MRI biomarkers such as the central vein sign and paramagnetic rim lesions show promise for differentiating multiple sclerosis from mimics and reducing misdiagnosis. @radiologyto https://t.co/AZHvMrrQSX
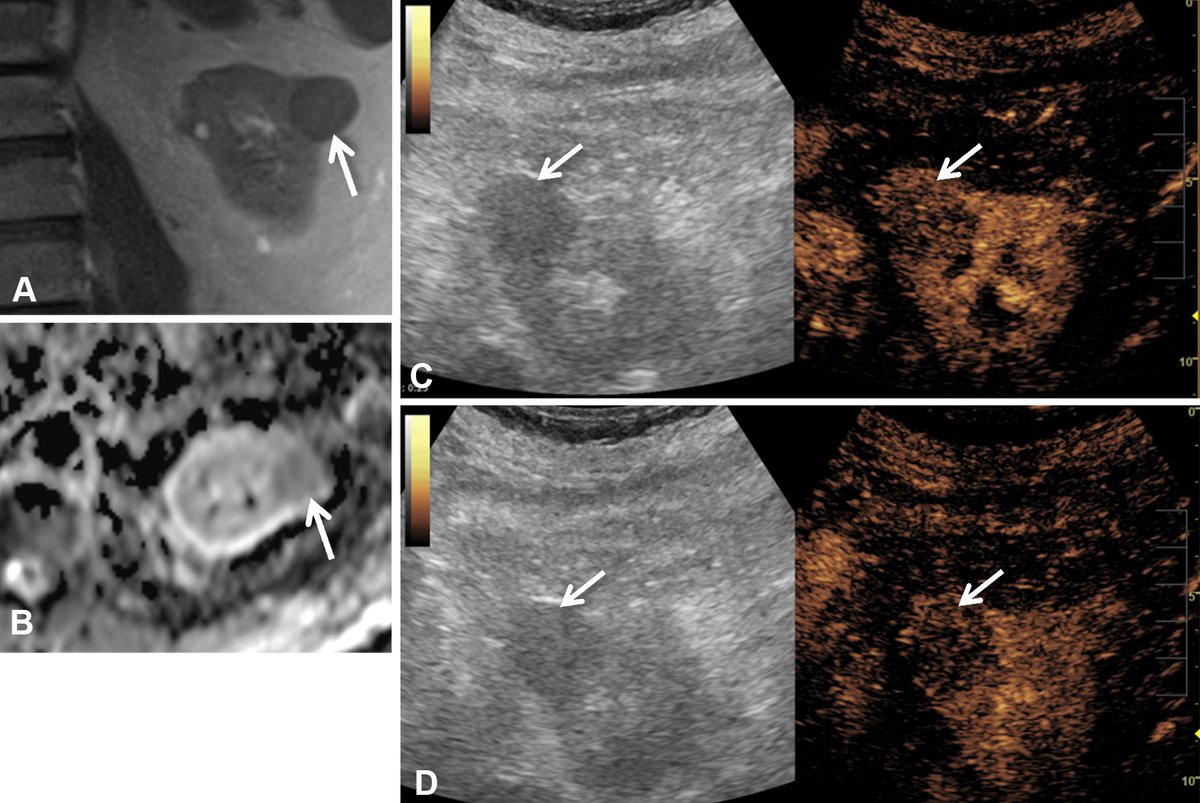
Renal lesions can be hard to characterize, especially in the absence of potentially nephro-toxic agents. Read how CEUS can characterize lesions as well as CT or MRI and gives better determination of avascular lesions from cysts. @MayoRadiology https://t.co/xA6fYmR5FT
11/Hopefully now you know that good things can often come in small field strengths!!
But this only scratches the surface!
Follow @theAJNR & check out the article for yourself:
https://t.co/tB14xq5I07
In medicine, anatomy is power!
It helps diagnose & treat disease--but you must know it first!
Posterior fossa perforator branches are key in stroke. How many do YOU know?
Here's a color-coded map of the perforators for each, an easy reference guide to help you branch out!
Key points:
Here are the 3 main syndromes associated with occlusion of these perforators & some quick tips to remember classic signs:
—Low (proximal) occlusion:
Contralateral hemiparesis—I remember this because the low basilar is right by the vertebral arteries. So I remember cutting off ONE of the legs
CN 6 deficit: Here is where the vertebral arteries are moving towards the basilar at midline—so a deficit here will cause your eye to move towards midline with a CN6 deficit
—Mid occlusion:
Quadraparesis—I remember this bc cutting the basilar at the mid portion looks like cutting someone in half at the trunk. Neither leg will move after that!
Corticobulbar signs—Basilar is long like an esophagus. Cutting esophagus in half = can’t swallow = bulbar symptoms
—High occlusion
Contralateral hemiparesis—I remember this bc the top of the basilar is near the PCAs, which look like arms. So I remember cutting off ONE of the arms
PCA symptoms—bc it’s right by the PCAs!
Parinaud’s (upward gaze palsy)—PCAs are heading UP from the basilar towards the VISUAL cortex. So if you occlude them, you can’t go UP with your EYES!
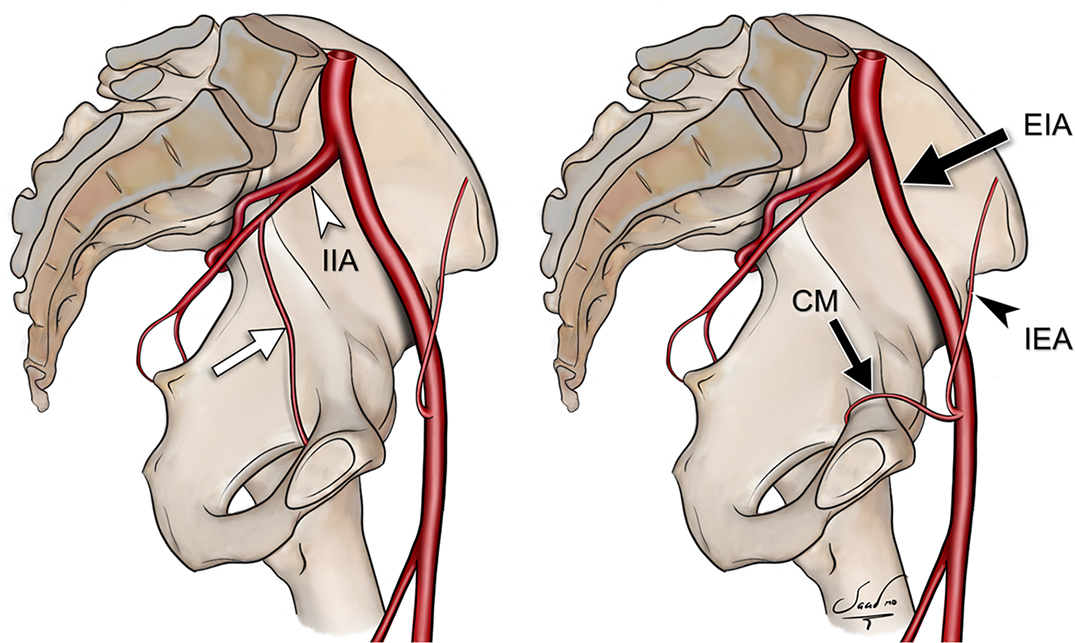
It is essential to understand variant vascular anatomy in MSK imaging to evaluate for potential clinical implications and risk of intraoperative injury. https://t.co/mdGwwPaAYB