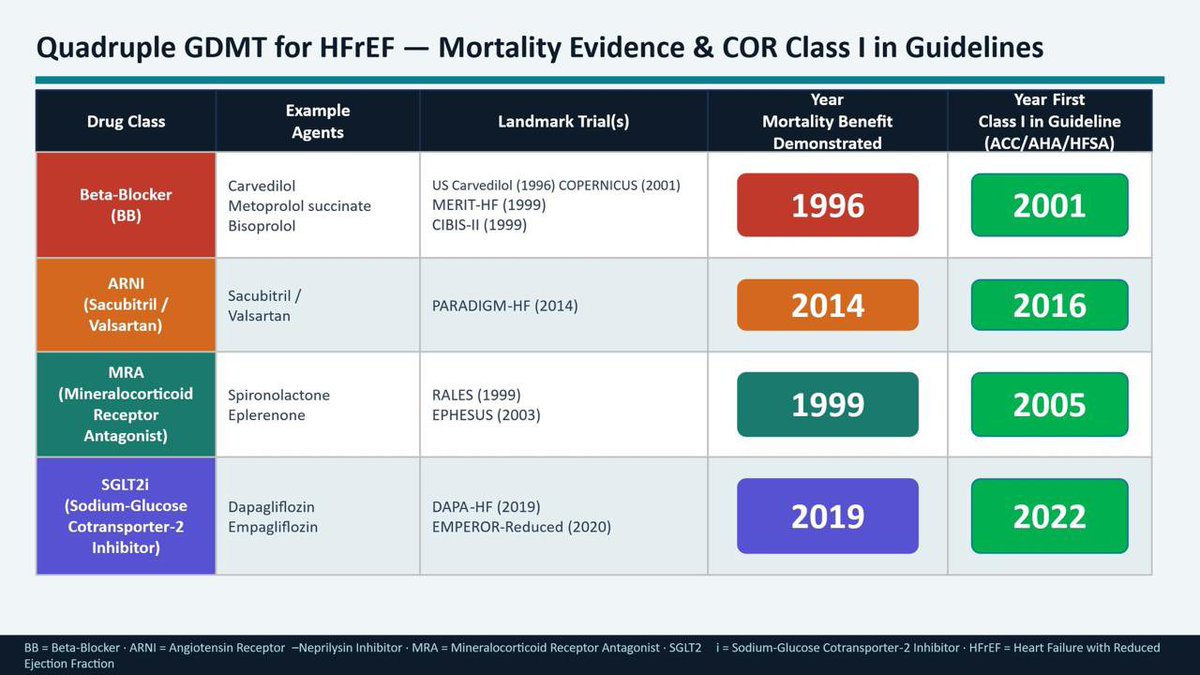
Every pillar of HFrEF quadruple therapy has Class I guideline evidence. Here’s how the science unfolded:
🔴 Beta-Blocker → mortality benefit 1996 → Class I in 2001
🟠 ARNI (Sacubitril/Valsartan) → PARADIGM-HF 2014 → Class I in 2016
🟢 MRA (Spironolactone/Eplerenone) → RALES 1999 → Class I in 2005
🟣 SGLT2i (Dapa/Empa) → DAPA-HF 2019 → Class I in 2022
Decades of landmark trials. Thousands of patients. One clear conclusion:
All four drugs. Every eligible patient.
The evidence is unambiguous. The guidelines are unambiguous.
Now we just have to act on them.
#HFrEF #GDMT #HeartFailure #Cardiology #CardioTwitter #MedTwitter
With deep sorrow, I received the news of Dr. Eugene Braunwald’s passing, one of the greatest figures in world cardiology.
His scientific legacy, clinical vision, and immeasurable contribution to generations of cardiologists will continue to live on in our daily practice and in the history of medicine.
My heartfelt condolences to his family, friends, students, and to the entire cardiology community. May he rest in peace.
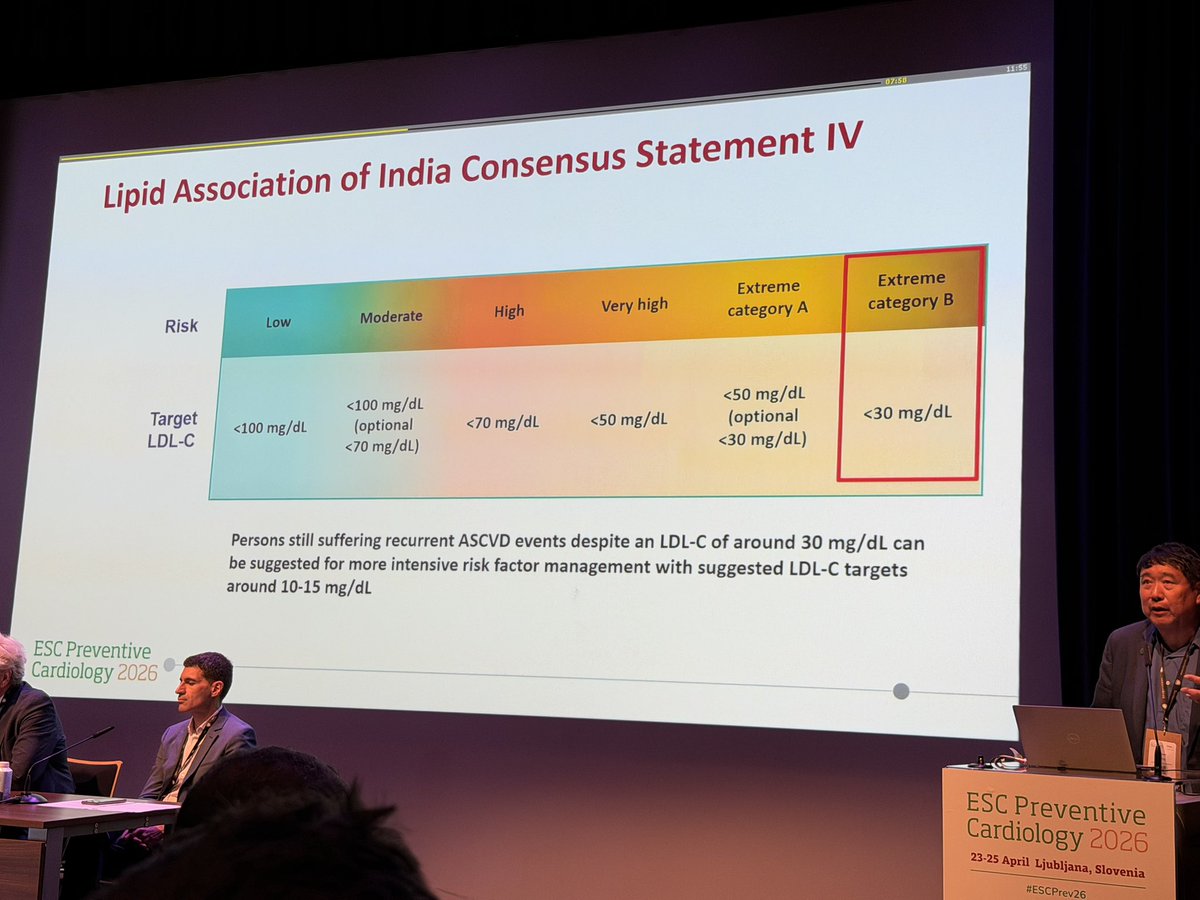
My Indian Friends, this is Nathan Wong MD and the statement of The Lipid Association Of India… your thoughts?
Please circulate if you approve!
#ESCPrev2026
The Hook
Cardiology trials keep telling you "20% risk reduction."
But what if that same trial meant:
→ 1 in 50 patients helped (NNT 50)
→ 49 of 50 got zero benefit
Welcome to the greatest trick in clinical trials: Relative Risk vs. Absolute Risk. A thread 🧵👇
Most common med student presentation mistake I see:
The opening sentence when presenting a patient should give the patient’s age, gender and why they are being seen but NOTHING more. Leave the other stuff out until after you orient the listener to why the patient is there.
Good: “53yom here with chest pain” “82yof day 3 post op”
After this you can fill in details and the listener is oriented as you speak.
Bad: “60yom with h/o HTN, diabetes, prior hip fracture, BPH, ED, anxiety, family history of colon CA who now comes in because of chest pain.”
The listener has no idea which parts of that PMH matter most until you say why the patient is being seen.
Ok, what do you think is this patient’s coronary calcium score, if I told you this is a 66 y old male with LDL 80 on no statins, would you prescribe LLT, what would be your target?
Heavy angiographic calcification of the proximal LAD, no real lesions, we know little!
The natural history of patients with medically managed CCS is not as benign as we think. Our analysis of reconstructed individual patient's data from 29 trials and 53,000 pts shows AMI rates of 12.5% at 5 years and 8.6% mortality rate.
Outcomes will be much worse in non RCT real-world populations where risk factor control less optimal and multimorbidity more prevalent.
work led by @Nicholaswschew and team
➡️ https://t.co/m30sllCBz5
⚠️ We’ve been explaining calcium in hyperkalemia WRONG for decades.
“Membrane stabilization”?
➡️ Probably not 🤔
🧠 What we were taught:
👉 Calcium restores resting membrane potential (RMP)
👉 That’s why it “stabilizes” the myocardium
Sounds clean.
But… it may be wrong physiology.
🔬 What this study shows:
▪️ Hyperkalemia →
→ ↑ RMP
→ ↓ sodium channel availability
→ severe conduction slowing → QRS widening → sine wave ECG
✔️ Calcium DOES improve ECG
✔️ Calcium DOES restore conduction
❌ But it does NOT restore RMP
⚡ So what is calcium really doing?
👉 It restores conduction velocity, not membrane potential
Mechanism:
▪️ ↑ L-type Ca²⁺ current
▪️ Enables Ca²⁺-dependent propagation
▪️ Bypasses impaired sodium channel conduction
➡️ The heart switches from Na⁺-dependent conduction → Ca²⁺-supported conduction
📉 Key physiological shift
Hyperkalemia:
▪️ Sodium channels ↓
▪️ Conduction fails
Calcium:
▪️ Doesn’t fix the membrane
▪️ Keeps the signal moving anyway
💡 Clinical implication:
👉 Calcium is NOT a “cosmetic ECG fix”
👉 It is a conduction rescue therapy
🎯 Use it when: ▪️ QRS widening
▪️ Conduction delay
▪️ Pre-arrest patterns
⚠️ NOT just for: ▪️ Isolated peaked T waves
🔥 Take-home
We should stop saying:
❌ “Calcium stabilizes the membrane”
And start saying:
✔️ “Calcium restores cardiac conduction during hyperkalemia”
📚 Piktel JS et al. (2024)
Critical Care Medicine
DOI: 10.1097/CCM.0000000000006376
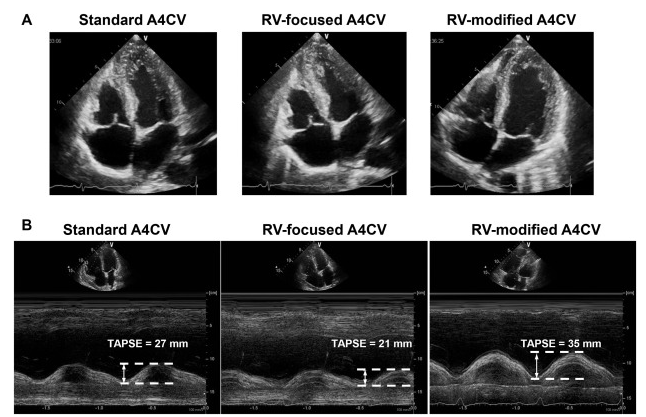
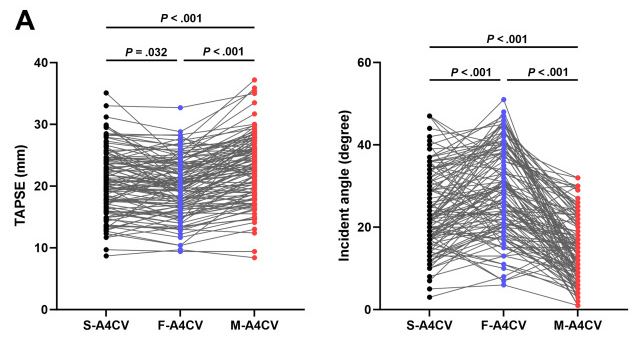
🧪 ¿Cómo se debe medir el #TAPSE en Ecocardiografía?
Un estudio reciente comparó 3 métodos distintos y hay un claro ganador:
⭐ El plano apical 4 cámaras modificado (A4C modificado):
👉🏼Se alinea mejor con el strain del ventrículo derecho
👉🏼Reduce los errores por el ángulo del haz de ultrasonido
🔗DOI: 10.1016/j.echo.2024.12.013
Heart failure is a clinical diagnosis based on symptoms and exam findings. You can’t make the diagnosis by echocardiogram. Patients with low LVEF can be euvolemic. And those with normal LVEF can be in significant heart failure (diastolic). We get an echo in new HF to guide management, but it does not make the diagnosis.
Missed STEMIs (NSTEMI-OMIs) have ~7.8% in-hospital mortality.
That’s higher than than the 1-year mortality after STEMI managed in time.
Time is muscle, regardless of ECG criteria. We now have tools to detect a significant proportion of these earlier at acceptable PPV!
If you keep your eyes open in medicine, you’ll notice lots of patients with symptoms we can’t explain through western medicine. Their tests are normal but they still have headaches, palpitations, chest pain, dizziness etc.
It’s important not to dismiss these patients. Their symptoms are real, and blowing them off drives people away from medical care.
It’s also important to remain humble. There is so much we don’t understand about the human body. I tell patients this and do not object if they want to explore options outside of western medicine. I’ve seen people improve with acupuncture, cupping, meditation, physical therapy, and even chiropractors in one case of chronic chest pain.
I don’t recommend these as first line treatments, and they should be used cautiously because they can lack rigorous evidence. But when patients are suffering and I can’t help them, I support anything that improves their quality of life.
🫀💊 The aspirin conundrum—solved (partly) by genetics
This 2025 American Journal of Preventive Cardiology State-of-the-Art Review tackles one of the longest-running dilemmas in prevention: why does low-dose aspirin help some people—but harm others? The answer may lie in Lp(a) genetics .
⚖️ The classic problem
In primary prevention, aspirin reduces myocardial infarction—but increases major bleeding to a similar extent. At the population level, benefits and harms cancel out, leading guidelines to largely step back from routine aspirin use.
🧬 Enter Lp(a) and the LPA genotype
The review focuses on a specific LPA polymorphism (rs3798220), present in ~3–4% of individuals, strongly associated with:
markedly elevated Lp(a) levels
increased atherothrombotic risk
Crucially, three large studies (Women’s Health Study, ARIC, ASPREE) show a consistent pattern:
In LPA-negative individuals → aspirin provides minimal benefit (very high NNT: 250–800)
In LPA-positive individuals → aspirin dramatically reduces cardiovascular events, bringing their risk down to the level of non-carriers
📊 The numbers matter
In LPA carriers:
Relative risk reduction: ~55–80%
Absolute risk reduction: ~2.7–3%
Number needed to treat (NNT): ~34–38👉 Comparable to, or better than, many statin trials.
🧠 Why this makes sense biologically
Lp(a) promotes thrombosis via its plasminogen-like structure. Aspirin doesn’t lower Lp(a) levels—but may neutralize its pro-thrombotic effect.
⚠️ Important caveats
Evidence is based on post-hoc genetic analyses
Most data come from European ancestry
Bleeding risk still exists and must be individualized
🔮 Bottom line
This paper reframes aspirin not as a blunt population tool—but as a precision therapy.
👉 For most people, aspirin isn’t worth it.
For a genetically defined few, it may be exactly right.
🧭 Sometimes, the problem isn’t the drug—it’s who we give it to.