Interesting case
Defer ad-hoc PCI as the patient is stable and STE resolved
Admit to CCU for anti thrombotic and anti platelets DAPT
reschedule him for IVUS during same admission to evaluate thrombotic resolution
Or optimize medical therapy
If the aneurysm >20 mm or > 3 of the reference vessel or unsuitable for covered stent call the CS for surgical ligation
🚨 CADENCE Trial — #ACC26
We have encouraging results from one of the most anticipated clinical trials at #ACC26
Sotatercept in patients with HFpEF and combined post- and precapillary pulmonary hypertension
🔑 Key findings:
• Significant reduction in pulmonary vascular resistance
• Improvements in mPAP and PAWP
• Better functional capacity (6MWD)
• Signals toward reduced clinical worsening
🧠 A promising new pathway targeting pulmonary vascular and cardiac remodeling
👀 Could this open a new era in HFpEF management?
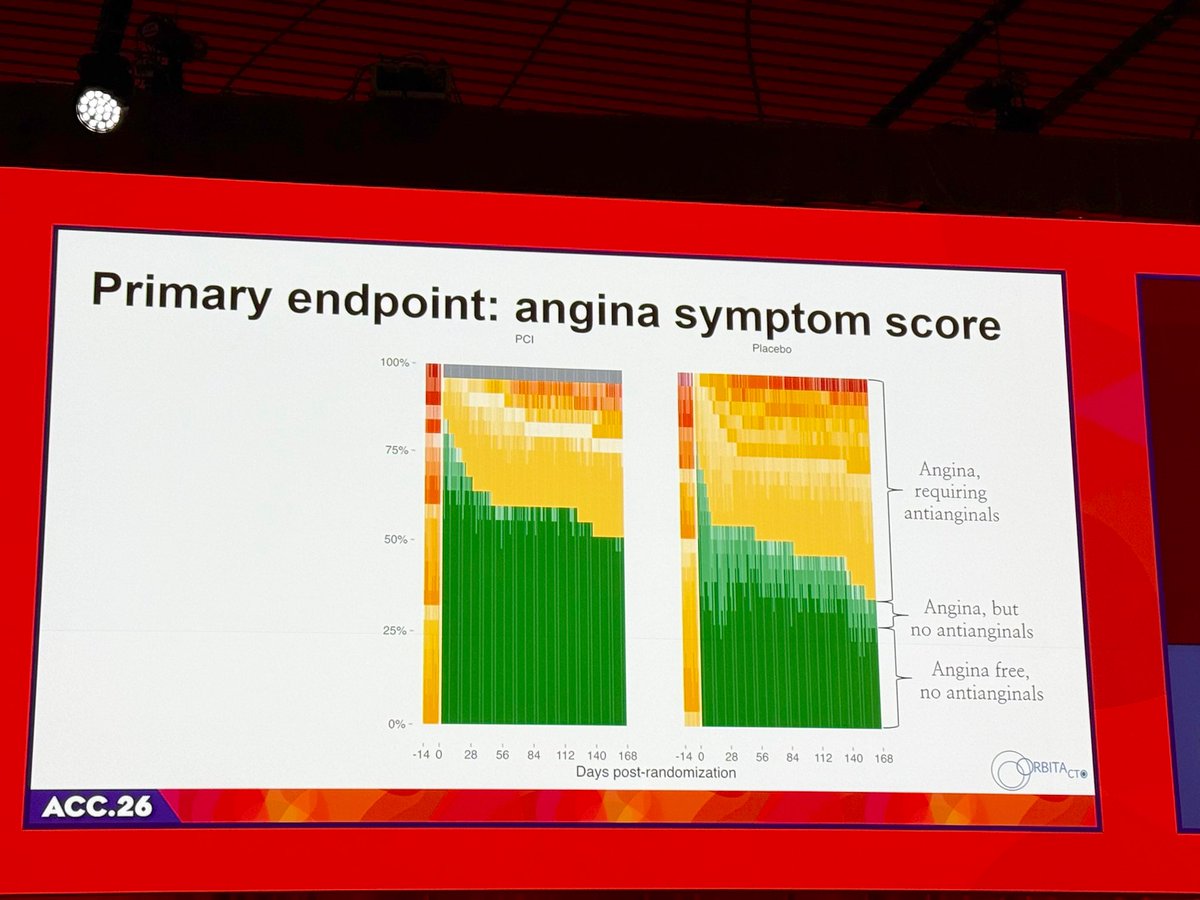
ORBITA-CTO #ACC26
СТО PCI reduced angina frequency (immediate consistent & sustained)
Excellent experienced operators, 25% pts had JC score 3 (difficult) CTO ,similar antianginal use in both groups( post pci angina, micro vascular dz, non cad pain?)
#ACC26 Much awaited Door to Unload trial for Anterior MI failed to show the benefit for Impella. Unload before Revasc for Ant MI. Surprisingly mean BP ~140 despite LVEDP in high 20s!
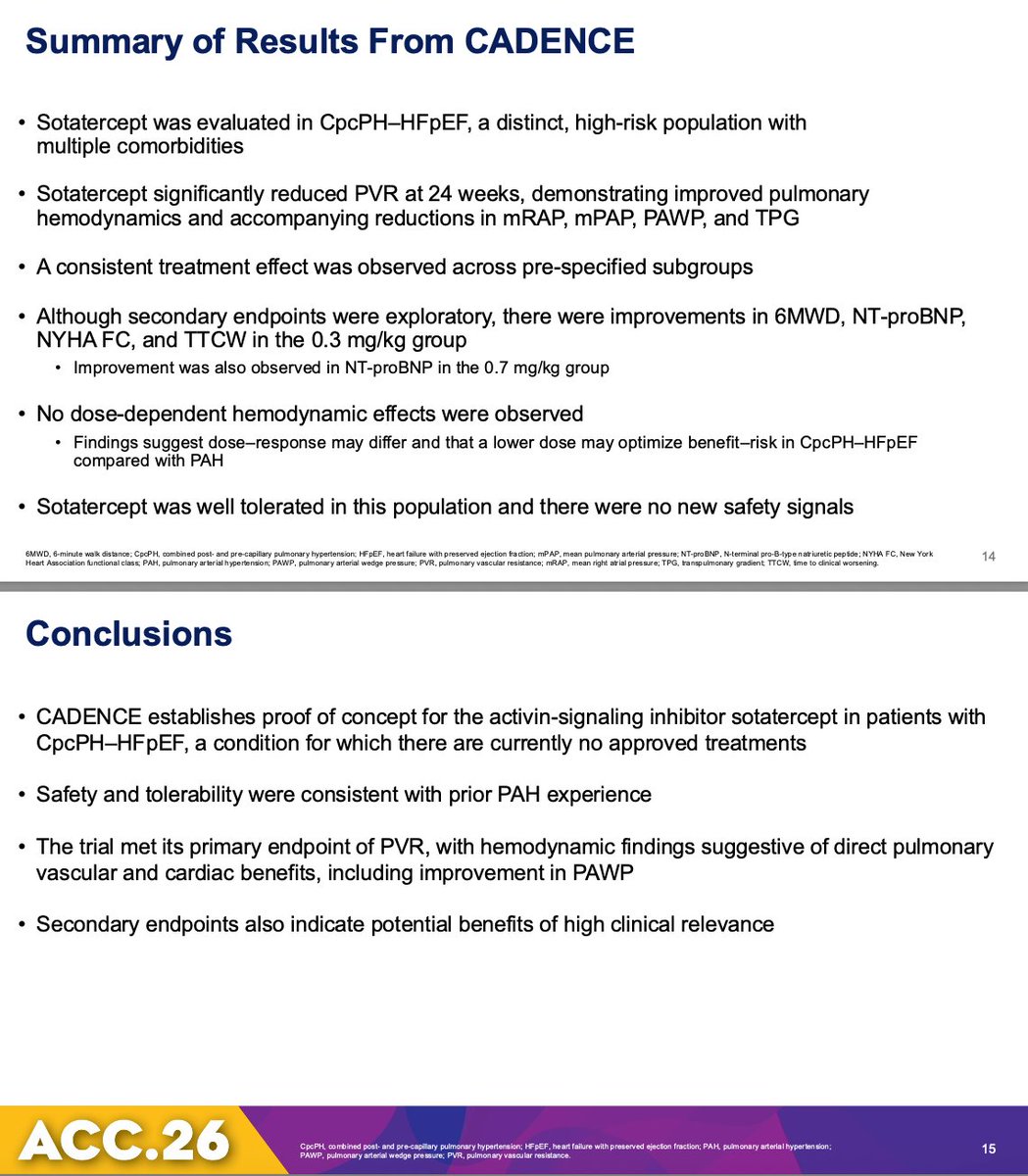
CADENCE #ACC26
🧑⚕️ HFpEF patients with combined post- and pre-capillary pulmonary hypertension —a high-risk group with no approved therapies
🧠Targeting activin signaling with sotatercept would improve pulmonary vascular disease and hemodynamics
📊 Primary result: Met primary endpoint → significant reduction in pulmonary vascular resistance (PVR)
📉Improvements in PAWP, exercise capacity, and other hemodynamics, suggesting both pulmonary + cardiac benefit
💡 First real signal that we can treat pulmonary vascular disease in HFpEF—not just manage symptoms
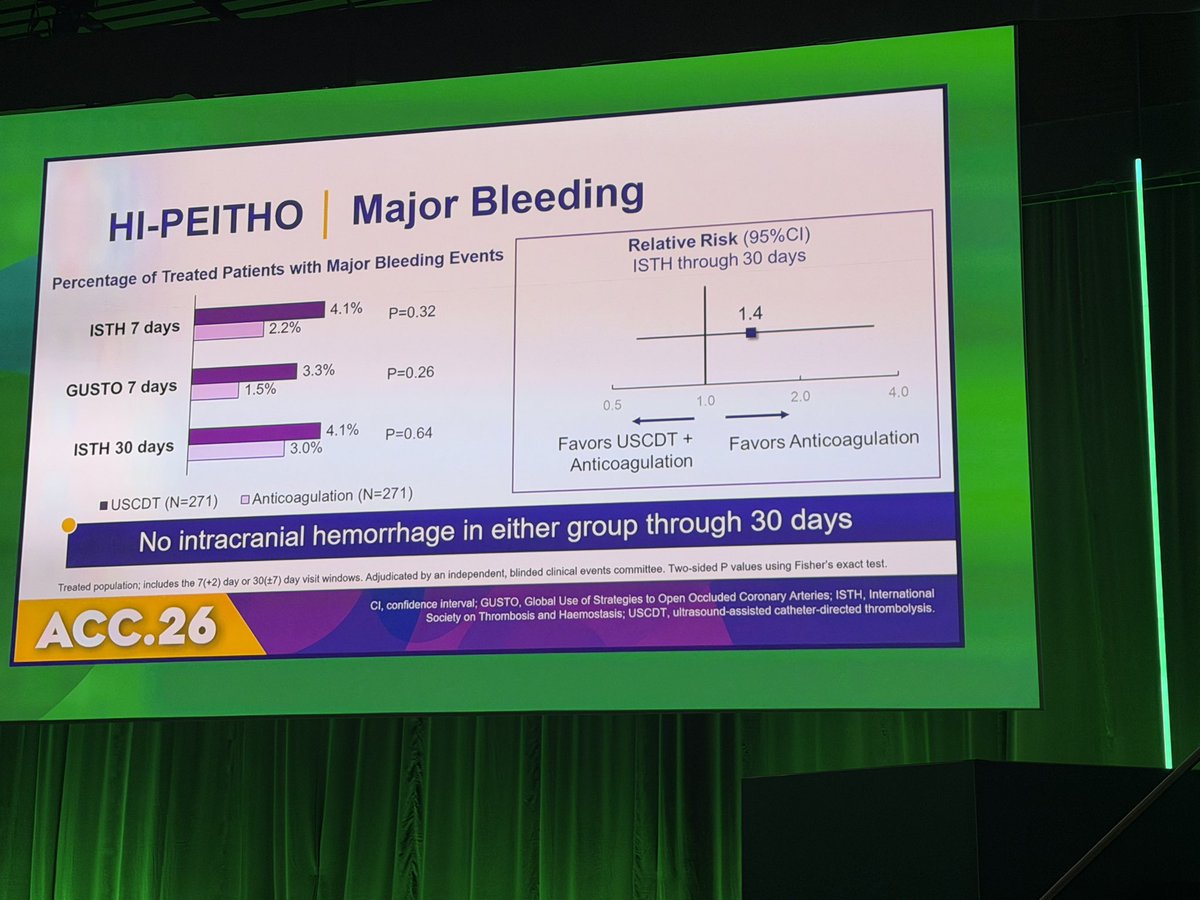
Management of intermediate–high-risk PE remains a major clinical challenge.
🎷HI-PEITHO tests catheter-directed thrombolysis vs anticoagulation alone.
Will this change how we escalate therapy in PE?
➡️ Key results:
🎷544 patients randomized w/ intermediate Risk PE- 43% female, mean age 58
🎷Anti CoAg 🆚 thrombolysis
🎷outcome: PE mortality/PE recurrence
💥Favored Catheter directed thrombolysis for PE: Relative Risk 0.39
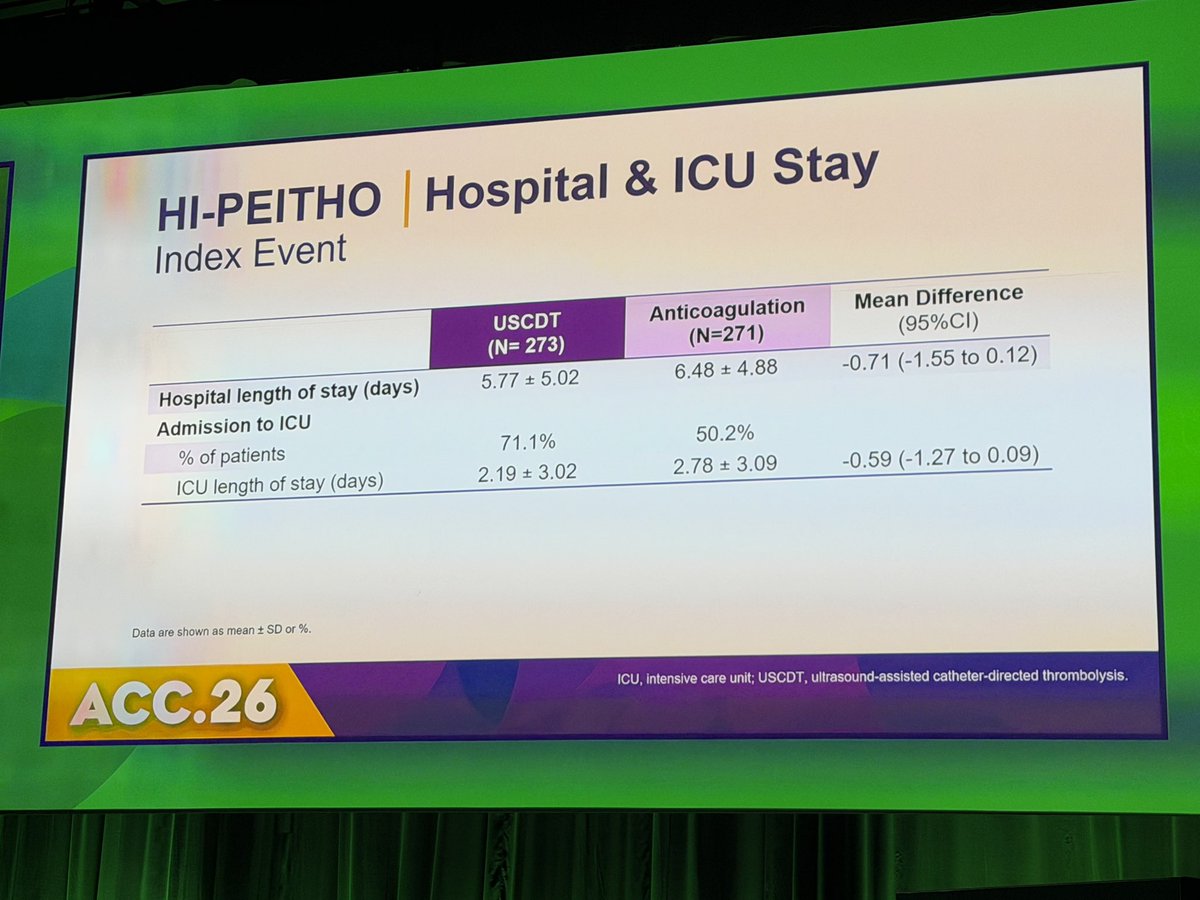
⤵️ Hospital stay
⤴️ Bleeding but no diff in major bleeding
#ACC26 #PulmonaryEmbolism #Cardiology
@NEJM
📎 https://t.co/wbrSDsVsXj
CHIP-BCIS3 evaluates LV unloading strategies in complex PCI
Can mechanical support improve outcomes in stable elective pci?
➡️ Key results:
Use of unloading with microaxial flow pump did not improve outcomes and was associated with ⤴️ CV deaths I. Patients with severe LV dysfunction undergoing complex PCI
83% Male
#ACC26 #PCI #CardioTwitter #LBCT @NEJM@mmamas1973
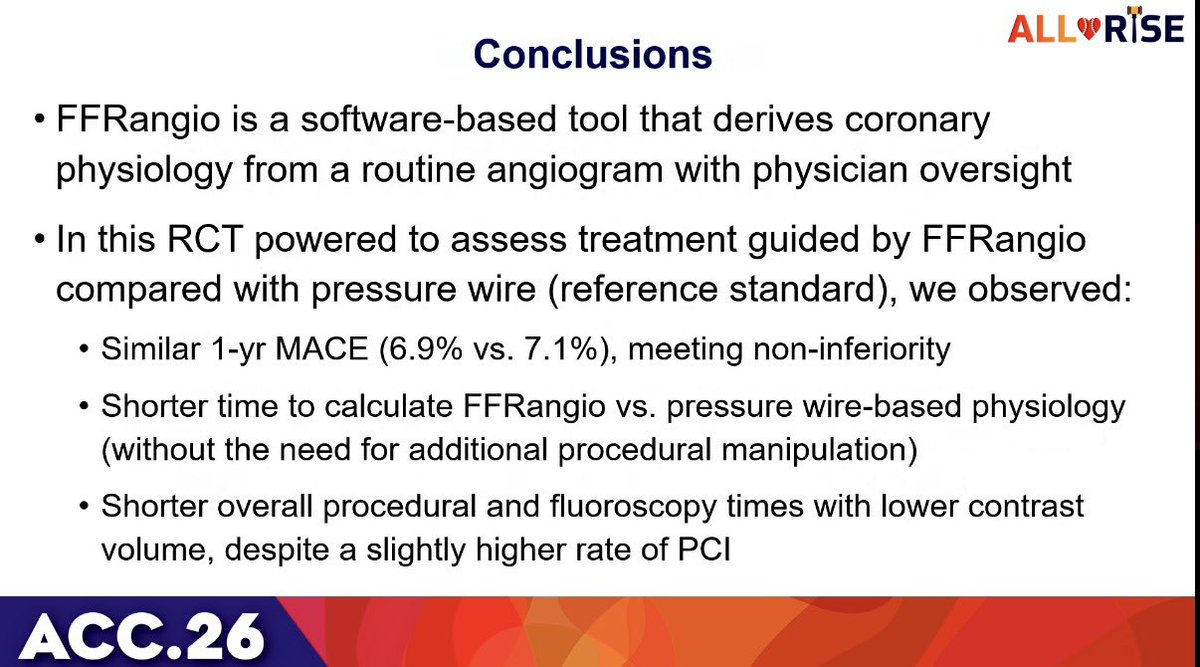
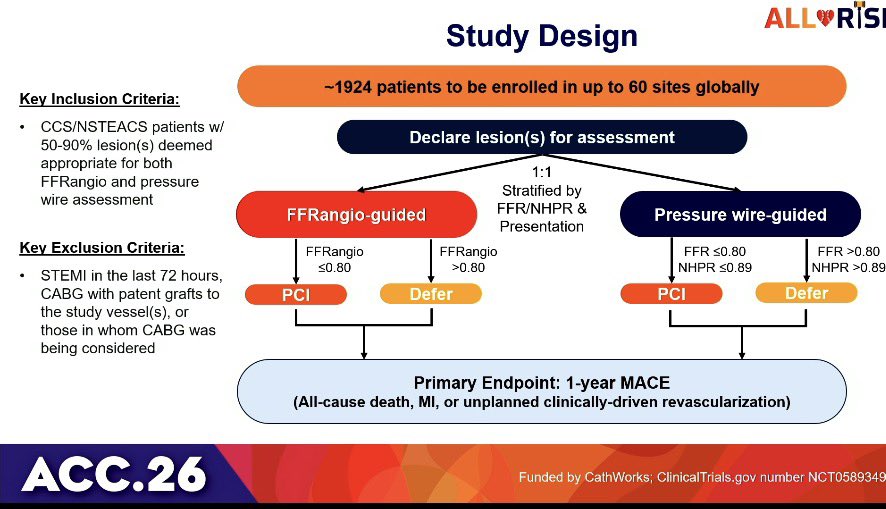
Do we still need pressure wires to guide PCI?
#ALLRISE trial compares angiography-derived physiology vs wire-based assessment.
Is FFRangio better than a pressure wire approach? Is it ready for prime time?
➡️ Key results:
🎷FFRangio 🆚 pressure wire: shorter time of procedure and same MACE outcomes at 1 year
🎷 Shorter time, ⤵️ fluoro ⤵️ contrast use
25% 💃🏻
#ACC26 #PCI #LBCT #CardioTwitter @NEJM
📎 https://t.co/ikH9K5gFUI
بين يومٍ أنت حاضر فيه… ويومٍ تغيب فيه، يظهر صدق النيّة كما هو، بلا زينةٍ ولا ادّعاء
فكم من اسمٍ علا حين خدم، ثم خبا حين استأثر،
وكم من أثرٍ صامتٍ بقي، لأن صاحبه مرّ خفيفًا… وأثقل الميزان.
ليست الحكاية في الوصول، بل في ما تتركه خلفك؛
فالطريق ينسى العابرين، ولا ينسى من مهّدوه