Youtube Link : https://t.co/O0Pepy9OvU
“I am still alive, but the film ‘Satluj’ shows me as dead.”
After 31 years, a key eyewitness in the Jaswant Singh Khalra case has broken his silence. Kikkar Singh, who says he personally fed Khalra while he was in police custody and later became a CBI witness, speaks out for the first time.
Christopher Nolan managed to create the most anxiety-inducing war movie opening in history using little to no dialogue and the literal ticking of his grandfather’s pocket watch.
@DhruvMundhraYT Dr. Shamsheer Vayalil is the richest doctor in India, with an estimated net worth of approximately $3.7 billion (around Rs. 30,770 crore). He is a radiologist.
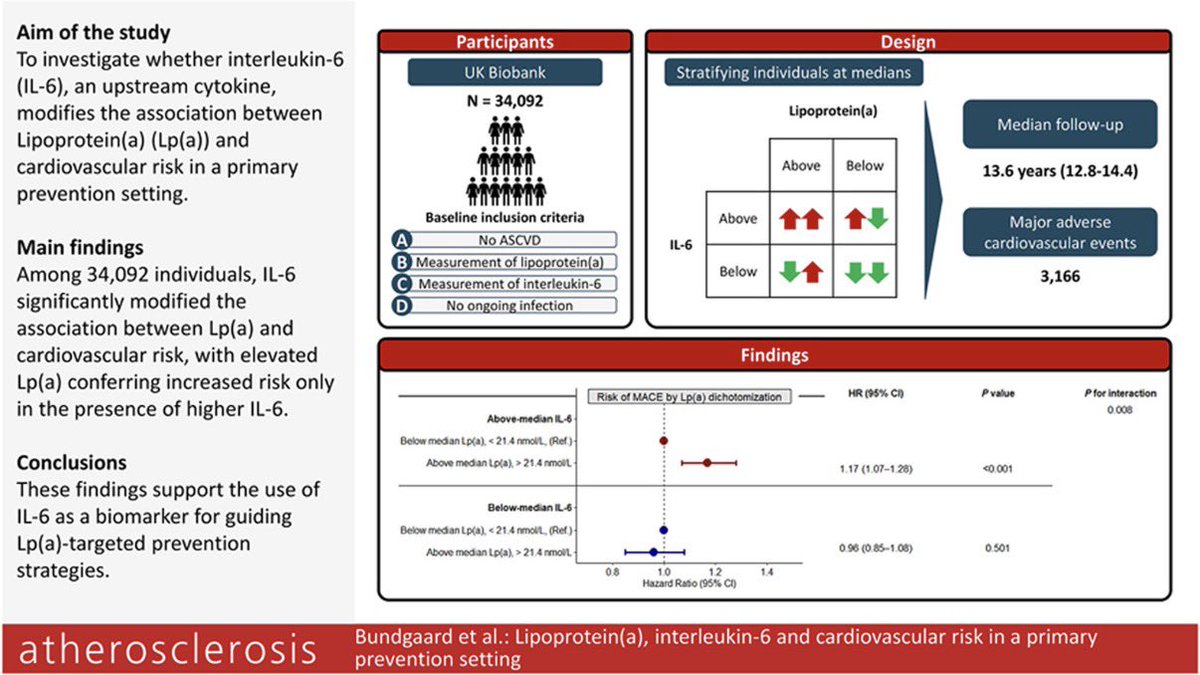
Lipoprotein(a), interleukin-6 and cardiovascular risk in a primary prevention setting
☝️New data from UK Biobank (n=34,092): In primary prevention, the cardiovascular risk associated with elevated Lp(a) was significantly influenced by IL-6, a key upstream inflammatory cytokine.
1️⃣ Higher Lp(a) increased MACE risk only when IL-6 was elevated (HR 1.17; 95% CI 1.07–1.28), while no significant association was seen when IL-6 was below median levels.
2️⃣ Inflammation appears to amplify Lp(a) pathogenicity, supporting the concept that not all elevated Lp(a) carries the same biological risk burden.
3️⃣ hs-CRP did not show the same modifying effect, suggesting IL-6 may be a more informative biomarker than conventional inflammatory markers for Lp(a)-related risk stratification.
4️⃣ Clinical implication: Future Lp(a)-lowering therapies may yield greatest benefit in individuals with concomitant elevated IL-6, enabling more precise preventive targeting.
👉 Elevated Lp(a) appears to confer its greatest cardiovascular hazard in the presence of heightened IL-6–mediated inflammation, supporting a biologically integrated model in which inherited atherothrombotic burden and residual inflammatory risk act synergistically
@ATHjournal@society_eas
🔗 https://t.co/dEWhC0JpAm
👉 Update on familial hypercholesterolemia: An expert clinical consensus from the National Lipid Association
👆 FH is common (≈1:311) and systematically underdiagnosed → the real problem is not rarity, it’s detection
👆 Driven by lifelong LDL-C exposure, not a single value → risk = LDL-C × time
👆 Genetics help, but phenotype rules → treat based on LDL-C burden, not just mutations
📍 Diagnosis
LDL-C ≥190 mg/dL (adults) → think FH, but confirm clinically
Genetic testing = useful for cascade screening, not mandatory
Always exclude secondary causes before labeling
📍 Screening
Universal pediatric screening (9–11 yrs) is not optional—it’s delayed prevention
Cascade screening = highest yield strategy (and still underused)
📍 Risk
Standard risk calculators? Useless in FH → they underestimate risk
Risk depends on:
Lifetime LDL exposure
Lp(a)
Family history
Timing of treatment
📍 Treatment (no shortcuts)
Lifelong, early, aggressive
Targets:
<55 mg/dL (secondary prevention)
<70 mg/dL (primary prevention)
Start with:
High-intensity statin, ezetimibe, PCSK9i / others as needed
≥50% LDL reduction is the floor, not the goal
📍 Take-home
FH is not a lipid disorder.
It’s a time-dependent vascular disease.
Diagnose early, treat hard, treat forever.
🔗 🔓 Open Access https://t.co/mt2c3QNp9y
@nationallipid@LipidJournal@society_eas
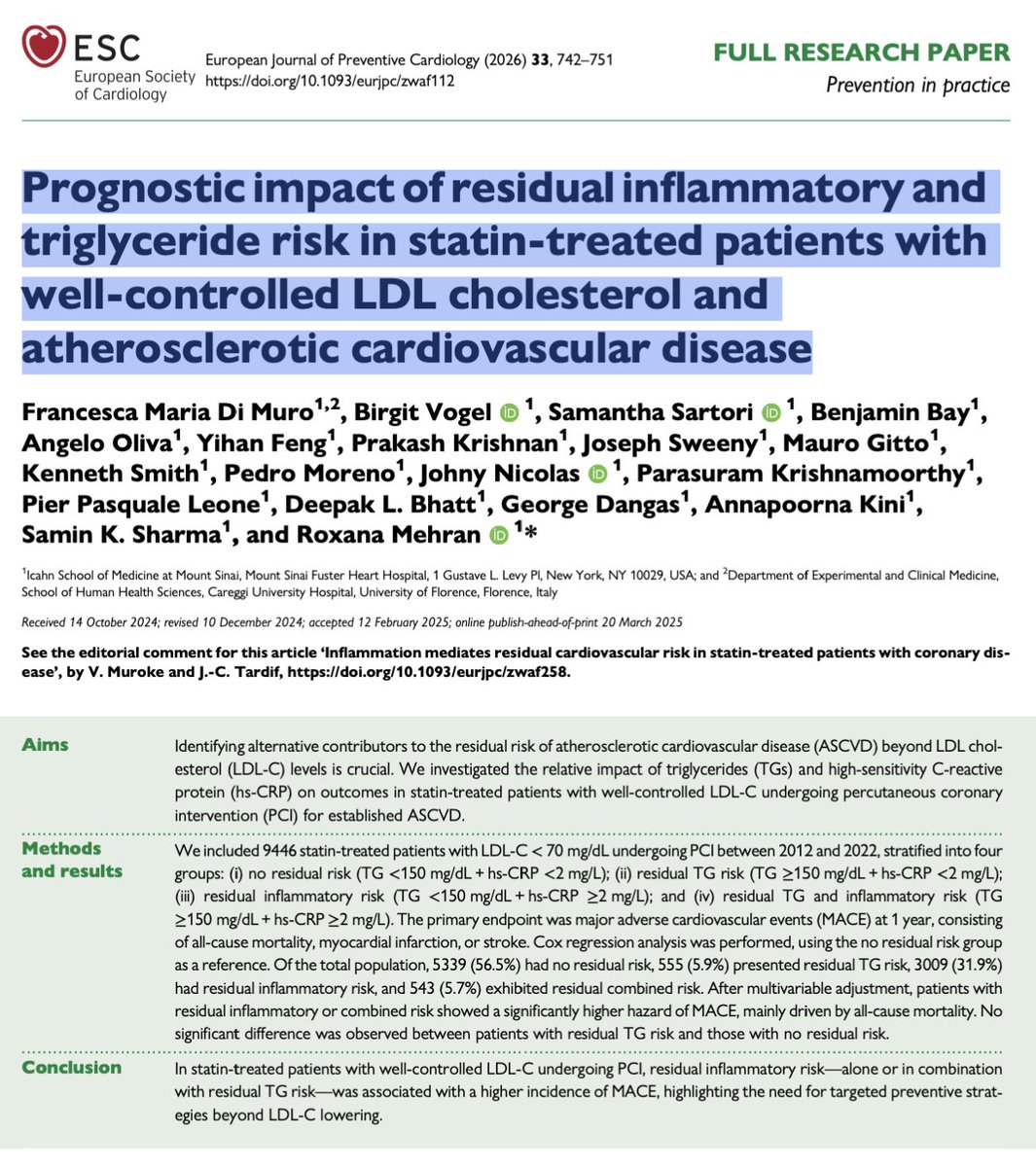
🫀🔥 LDL is controlled. Statins are optimized. And yet… patients still have events.
This study addresses one of the most important unanswered questions in cardiology:
👉 What really drives residual cardiovascular risk?
📊 In >9,400 statin-treated patients with LDL <70 mg/dL undergoing PCI:
Patients were stratified by:
Triglycerides (TG ≥150 mg/dL)
Inflammation (hs-CRP ≥2 mg/L)
💡 The result is striking:
👉 Inflammation—not triglycerides—drives risk
Residual inflammatory risk → ~1.8x higher MACE
Combined TG + inflammation → ~1.9x higher MACE
Residual TG risk alone → NO significant increase
⚠️ And what’s driving this?
👉 Mostly all-cause mortality
Not subtle. Not marginal.
👉 Clinically meaningful.
🧠 Let’s be clear:
We’ve spent decades optimizing:
✔ LDL
✔ Lipid profiles
✔ Cholesterol targets
But this study shows:
👉 You can win the lipid battle… and still lose the war
🔥 Because atherosclerosis is not just lipid-driven.
👉 It’s an inflammatory disease
🎯 Clinical implication
Risk stratification cannot stop at LDL.
We need to integrate:
hs-CRP
Inflammatory burden
Systemic biology
🚀 Paradigm shift
From:
❌ “How low is LDL?”
➡️ to
✅ “How active is the disease?”
🧠 Bottom line
Lowering LDL is necessary.
👉 But it is NOT sufficient.
If inflammation persists:
👉 Risk persists.
⚡ The future of prevention?
Not just lipid control.
👉 Inflammation-guided precision cardiology.