Video surveillance captured an episode of syncope from ventricular arrhythmia in a 47-year-old man with heart failure with a reduced ejection fraction and an implantable cardioverter–defibrillator for the primary prevention of sudden cardiac death. Full case details: https://t.co/SXodrEVrqv
Building on the First Definition of Heart Failure, the Second Definition refines HF staging with sharper stage criteria, emphasizing early detection and individualized risk reduction and introduces the universal classification of HF causes, with explicit acknowledgment of geographic variation in HF risk and outcomes. https://t.co/YDuE4stb5s
This updated document provides a unified, internationally harmonized framework intended to standardize terminology. It addresses changes in disease manifestations, diagnostic strategies, and understanding of pathophysiology.
✍🏼 @MinnowWalsh@KarenSliwa@amibanerjee1@BiykemB@akshaydesaimd@DukeHFDoc@MKIttlesonMD@lamcardio@WilfriedMullens@NutritionHF
PHYSICAL EXAMINATION:
- Thin papery skin
- Easy spontaneous bruising
- Buffalo hump
- Severe dehydration
- Drowsiness/confusion
- Features of shock
LAB FINDINGS:
🧪 Sodium: 120.4
🧪 Potassium: 6.78
The patient developed hypotensive shock not responding adequately to IV fluids.
We are currently managing this case as Addisonian Crisis.
KEY POINTS FOR CLINICAL PRACTICE:
⚠️ Long-term steroid use can suppress adrenal axis
⚠️ Stress/infection can precipitate acute adrenal failure
⚠️ Shock + hyponatremia + hyperkalemia is a critical diagnostic triad
⚠️ Treatment should NOT be delayed for cortisol confirmation
ONGOING MANAGEMENT:
💉 IV Hydrocortisone 100 mg stat
💧 Aggressive IV normal saline resuscitation
🍬 Dextrose if hypoglycemia present
🦠 Management of underlying trigger
One diagnosis where early recognition can literally save a patient’s life.
Inhaled corticosteroids are the foundation of asthma therapy and play a crucial role in reducing the risk of asthma attacks.
In @LancetRespirMed, a Personal View discusses how inhaled corticosteroids have changed asthma treatment over the last 50 years: https://t.co/wPKdt6Byw1
Inflammatory myopathies are typically associated with a myositis-specific autoantibody that determines the diagnosis and prognosis. Myositis subgroups have distinct pathomechanisms that now allow for targeted therapies.
Learn more in the Review Article “Inflammatory Myopathies” by Yves Allenbach, MD, PhD, and Olivier Benveniste, MD, PhD: https://t.co/ZeCKdNe87v
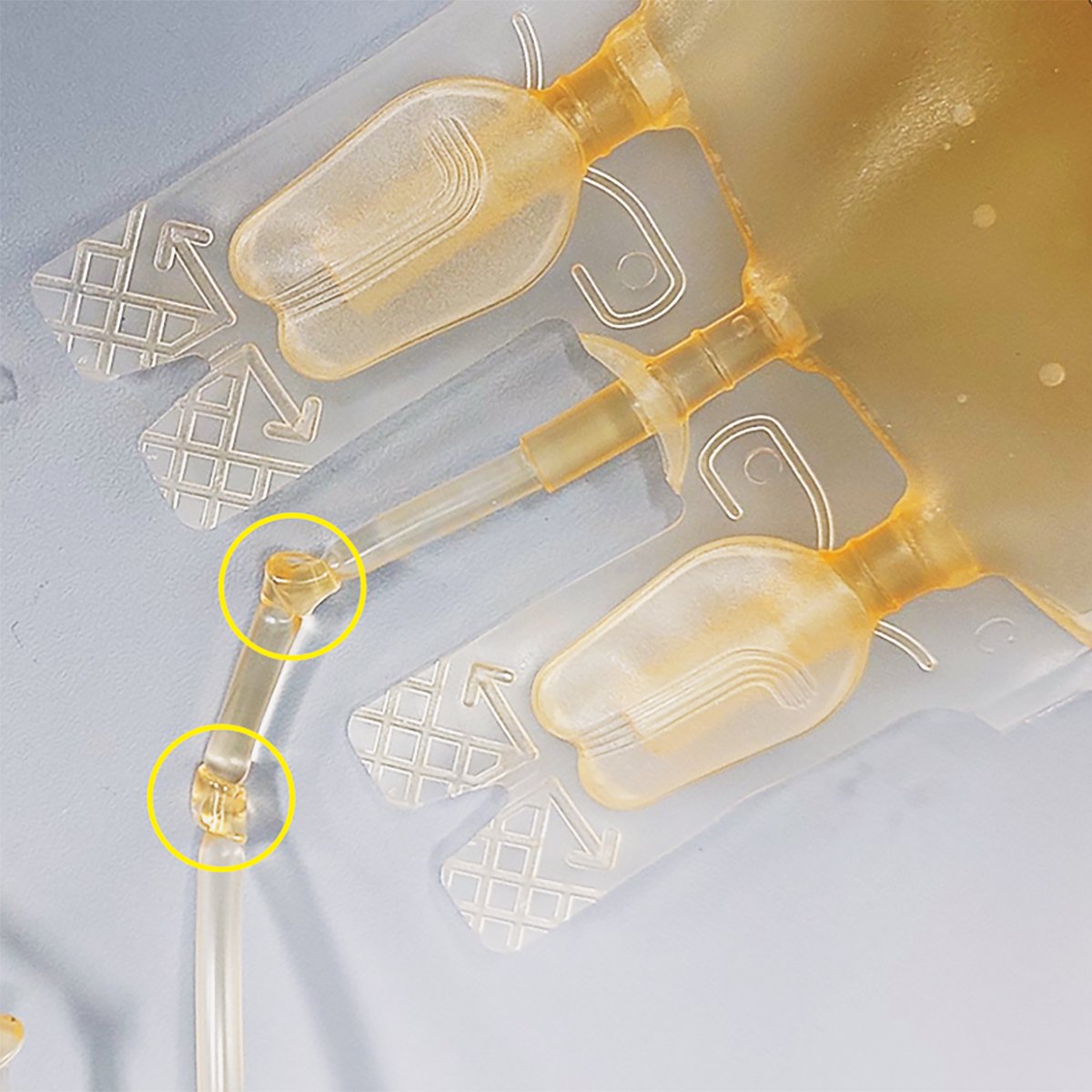
In a study involving 180 blood bags, use of a double-knot closure rather than the usual single knot prevented bacterial contamination. This strategy may reduce the risk of blood-product contamination in resource-limited settings. Full study results: https://t.co/HIvnLXDNJY
An 86-year-old man presented to the neurology clinic with 2 years of progressive memory loss and difficulty walking. An MRI showed microbleeds that appeared as hypointense foci throughout the lobar regions.
Read the full case details in the Images in Clinical Medicine article “Cerebral Amyloid Angiopathy”: https://t.co/Q3Otm9lH9q
Learn more about cerebral amyloid angiopathy in a new Review Article: https://t.co/dEMf0G2Nky
Dr. Sanjiv Shah explains the H2FPEF score used to support clinical decision making. Watch “HFpEF Explained — Prevalence, New Advances, and How to Diagnose,” a new Double Take video, now available on our YouTube channel.
Sign of the day.
CARNETT SIGN
Clinical finding
Describes an examination finding used to distinguish pain arising from the abdominal wall from pain arising from within the abdomen itself.
Testing for CARNETT SIGN is performed as a two stage procedure.
1. The examiner locates the point of maximal tenderness through palpation of the abdomen with the patient’s abdominal muscles relaxed.
2. The patient then tenses their abdominal muscles -
A) By lifting their head from the pillow or
B) raising their legs with the knees straightened
Examiner then applies pressure to the same point of tenderness.
The test is positive if the pain remains the same or worsens with tension of the rectus muscles .
A positive test is suggestive that the source of the pain is within the abdominal wall as opposed to the abdominal cavity.
Differentials of a positive test include
- Rectus sheath Hematoma.
- Anterior cutaneous nerve entrapment
The sign was first described in 1926 by JOHN BERTON CARNETT an American surgeon
🤓 AKI in the ICU is not just kidney failure.
It is a hemodynamic and congestion failure.
🚨 Reality check
👉 AKI occurs in:
▪️ 13-36% of acute HF patients
▪️ Up to 80% in cardiogenic shock
👉 Dialysis needed in up to 13%
👉 Strongly linked to mortality
⚠️ The key mistake
We treat AKI as a creatinine problem
💥 But it is actually:
👉 A perfusion + congestion problem
🧬 Core physiology
Renal perfusion pressure = MAP - CVP - IAP - airway pressure
📌 The nephron needs ≈ 40 mmHg to function
🔥 So what kills the kidney?
Not just low pressure
But:
▪️ Venous congestion (↑CVP)
▪️ Fluid overload
▪️ Intra-abdominal hypertension
▪️ Low forward flow
🧩 Step-by-step mindset
1️⃣ Confirm congestion
👉 JVP, no fluid responsiveness, VExUS ≥1
2️⃣ Optimize hemodynamics
👉 Maintain MAP ≥65 mmHg
3️⃣ Decongest
👉 Diuretics = cornerstone
4️⃣ Escalate
👉 CRRT if failure
📌 It’s a flow-pressure-congestion algorithm
💊 Pharmacology reality
❌ “Renal-dose dopamine” → useless AND harmful
❌ No drug prevents AKI
✔️ Loop diuretics → first-line
✔️ Sequential nephron blockade if resistance
⚡ Diuretic resistance = turning point
👉 Think:
▪️ Gut edema → poor absorption
▪️ Hypoperfusion
▪️ Tubular dysfunction
👉 Solutions:
▪️ Higher doses
▪️ Combination therapy (thiazides, acetazolamide)
▪️ Consider hypertonic saline strategy
🚨 CRRT is NOT first-line
👉 Indications = AEIOU:
▪️ Acidosis
▪️ Electrolytes
▪️ Intoxication
▪️ Overload
▪️ Uremia
👉 Early CRRT?
❌ No mortality benefit
✔️ Wait-and-see + optimize first
🧠 Advanced insight
👉 The kidney fails more from:
✔️ Congestion than hypotension
✔️ Venous pressure than arterial pressure
🔥 Take-home
AKI management in ICU is:
✔️ Hemodynamic
✔️ Congestion-driven
✔️ Stepwise
🚨 Final message
👉 Don’t chase creatinine
👉 Don’t reflexively dialyze
Treat:
Perfusion + Decongestion + Time
📚 Riccardi et al.
European Heart Journal Acute Cardiovascular Care, 2025
https://t.co/OLnrbCQ8Y2
Brief, positionally triggered vertigo with transient nystagmus on the Dix-Hallpike test is characteristic of #BPPV, a common and treatable cause of dizziness.
📊 Learn more in this JAMA Insights. https://t.co/3eokmi6hix
New in the April 23, 2026, issue of NEJM:
Antihypertensive Pill after Intracerebral Hemorrhage (TRIDENT trial) https://t.co/0tiij1H7tb
Oral Nirmatrelvir–Ritonavir for Covid-19 (PANORAMIC and CanTreatCOVID trials) https://t.co/5djnYnxMmn
tE2 Patches in Locally Advanced Prostate Cancer (STAMPEDE-1 and PATCH trials) https://t.co/sKJ6Sr6WiW
Ketamine or Etomidate for Tracheal Intubation (RSI trial) https://t.co/SN8naUiPYM
Subscribe to NEJM for the latest medical research: https://t.co/M7z7dzIiUA
Spinal epidural abscess is an infection in the epidural space commonly caused by 𝘚𝘵𝘢𝘱𝘩𝘺𝘭𝘰𝘤𝘰𝘤𝘤𝘶𝘴 𝘢𝘶𝘳𝘦𝘶𝘴. Symptoms include back pain, neck pain, fever, and neurologic symptoms. Prompt evaluation is important.
Learn more in the Review Article “Spinal Epidural Abscess” by Aaron J. Tande, MD, Bradford L. Currier, MD, and Douglas R. Osmon, MD, from @mayoclinic: https://t.co/f1uImZ7uHD