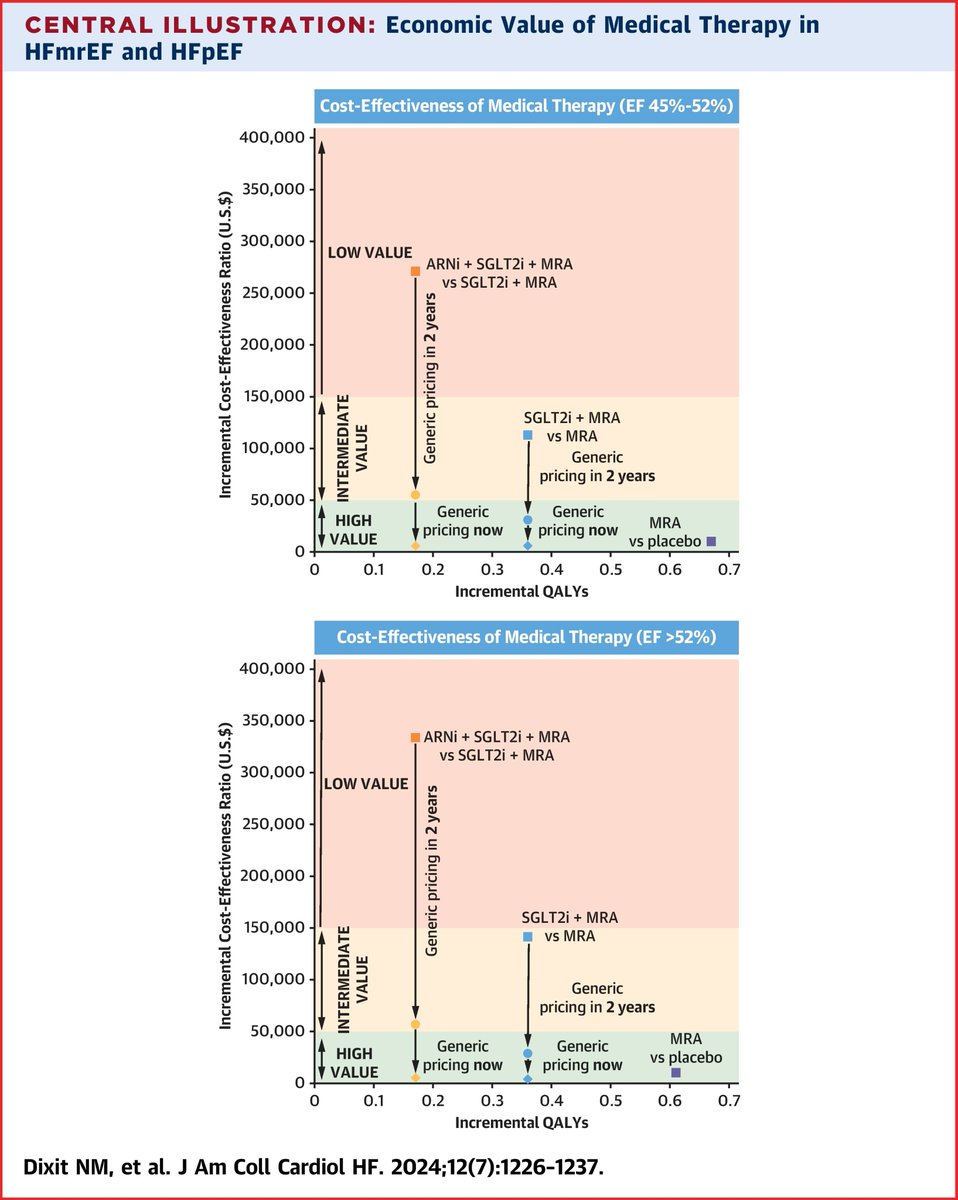
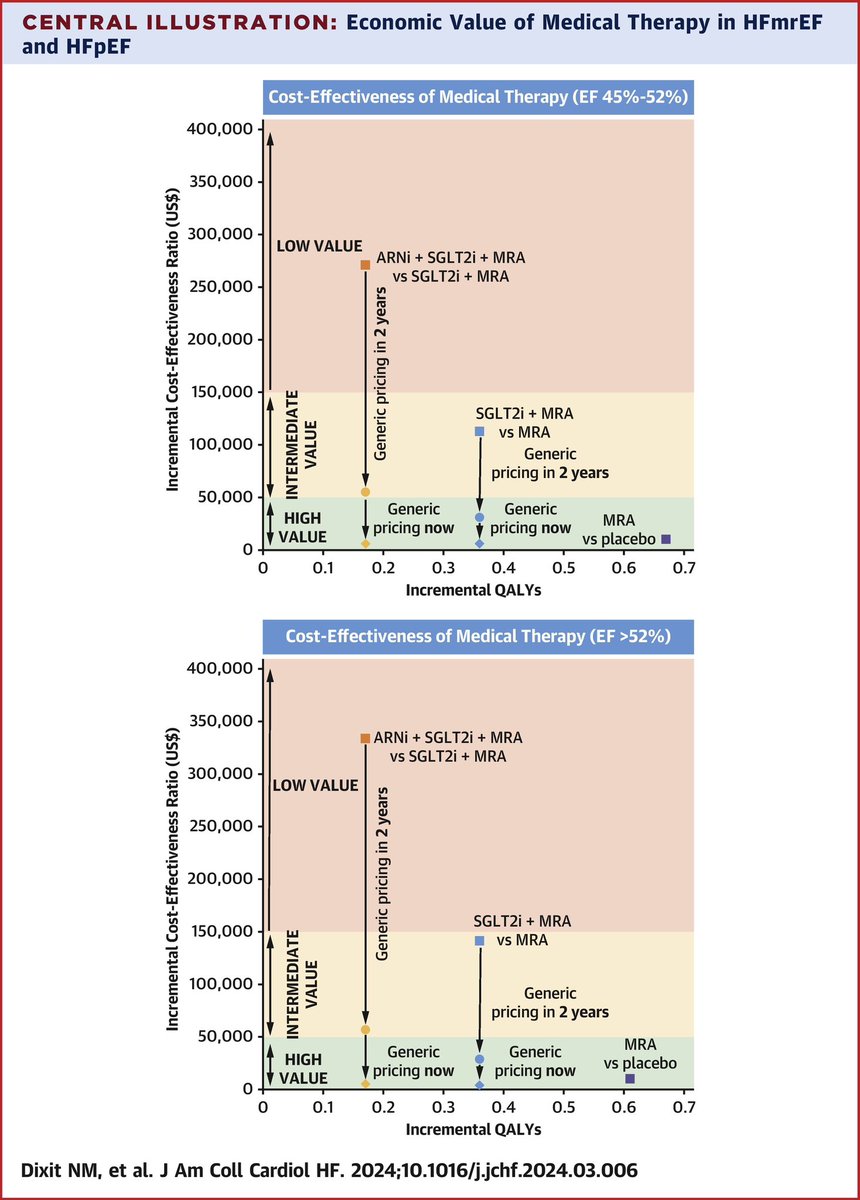
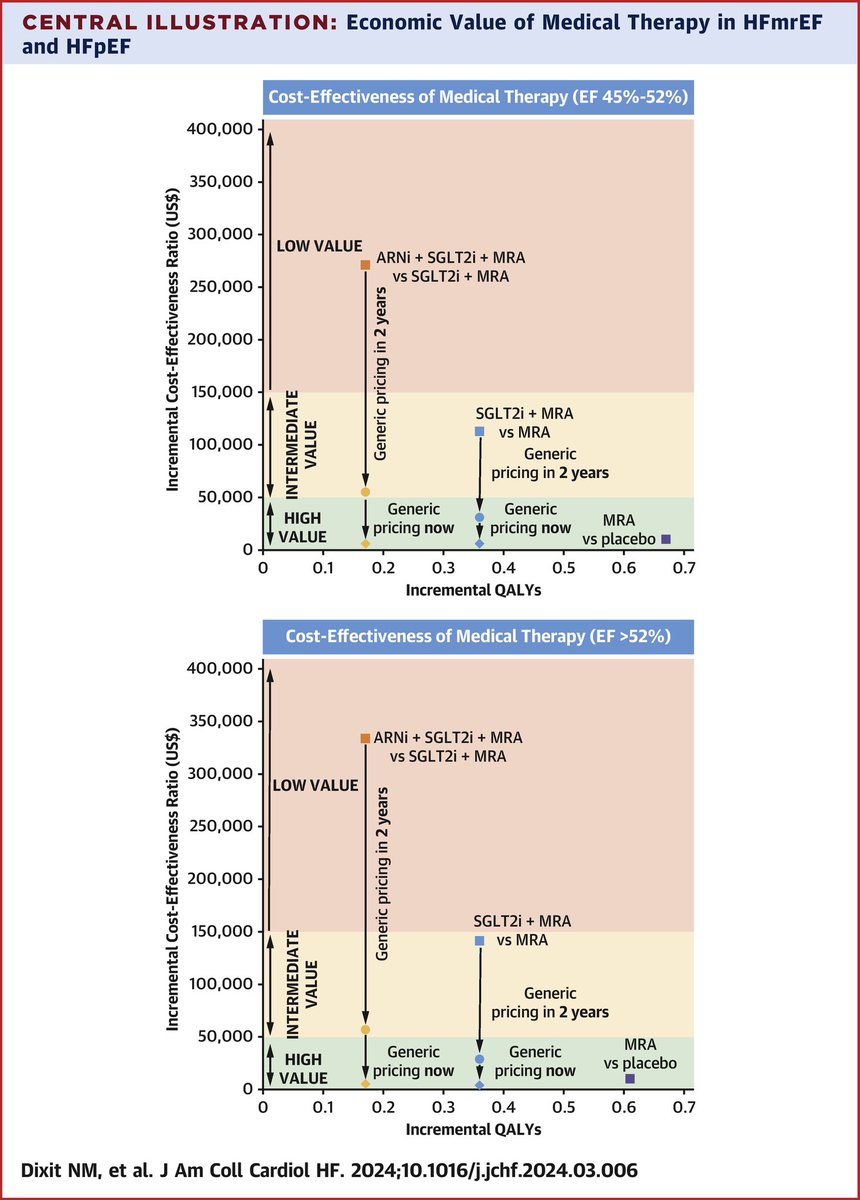
For patients with #HFmrEF and #HFpEF, Tx with MRA was of high value and #SGLT2i was of intermediate value and should be encouraged in implementation efforts. ARNI is of low value at the current cost. If generic, all are of high value. https://t.co/WU5L2ojrvk #JACCHF
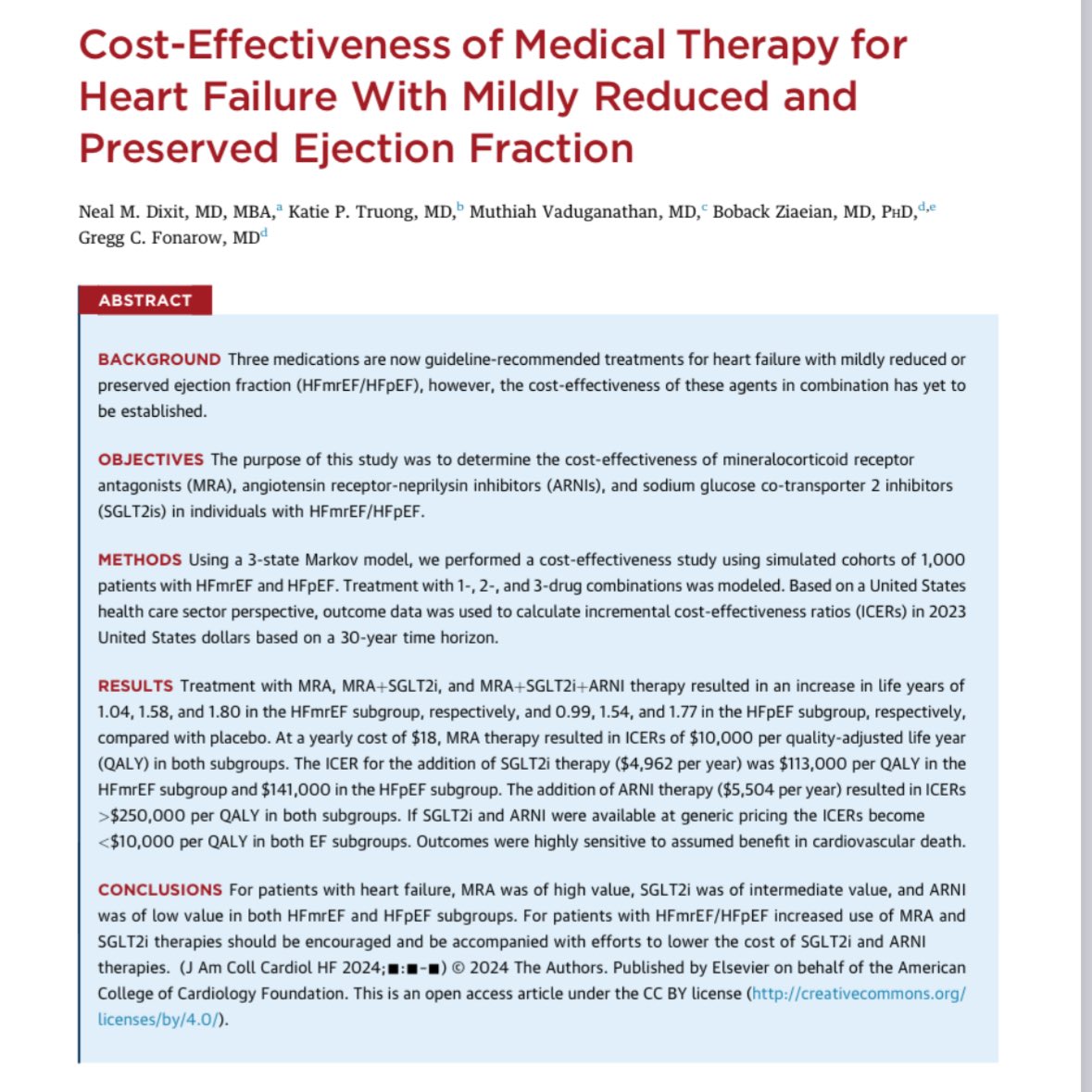
What is a cost-effective GDMT strategy for HFmrEF/HFpEF?
We built a model w/ clinical trial data (TOPCAT, PARAGON-HF, EMPEROR/DELIVER) and simulated outcomes w/ regimens of MRA/SGLT2i/ARNi.
Best 💊 combo?
MRA + SGLT2i
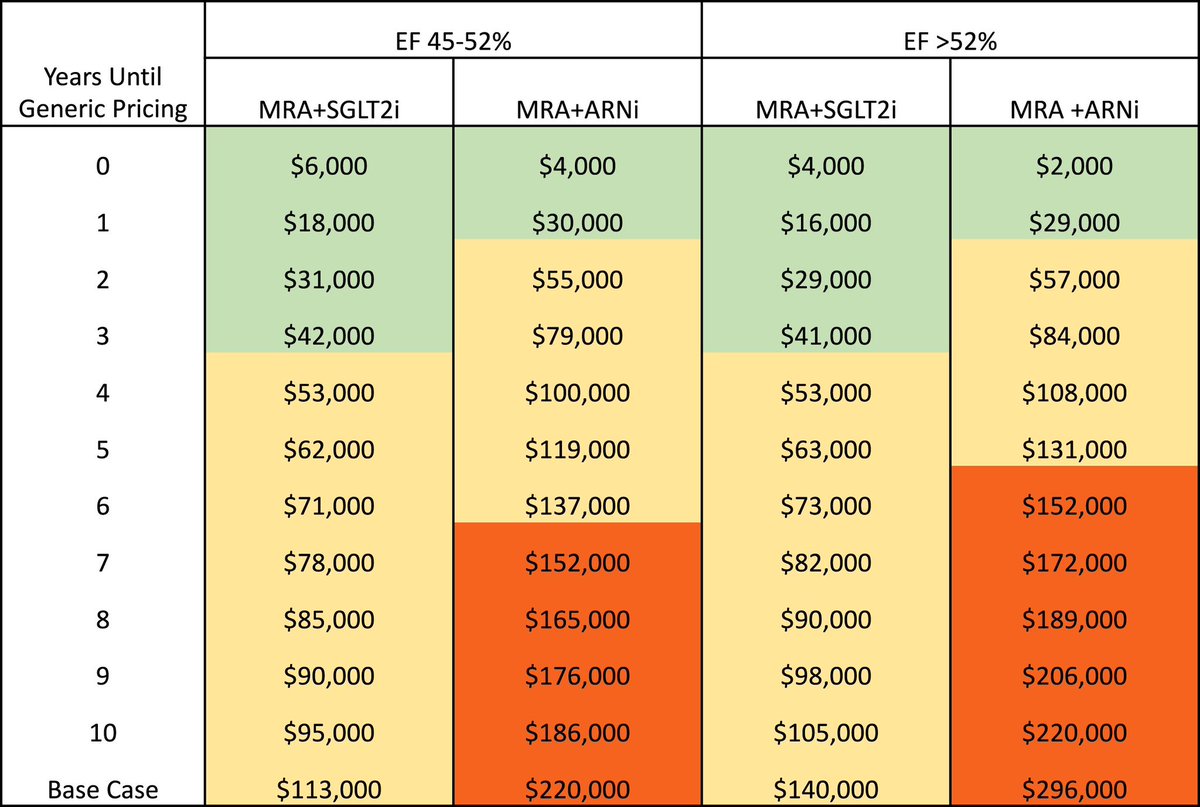
ARNi ⬇️ value at current 💵
Treat HF with urgency!
With the growing interest of #TEER in the tricuspid space...what is its utility in radiation valvulopathy & other #cardioonc sequelae in the cancer survivor?
@UWCardiology ❤️fellow @katieptr presents this dramatic case of cardiogenic shock & interesting hemo findings in @CircHF!
Check out our editorial on the importance of bystander CPR for all cases of out of hospital cardiac arrest just published in @JACCJournals ! Led by my incredible co-fellow @cooperbkersey @uwashfellows
https://t.co/Pt7DWkQfof
We explore tricuspid TEER in this unique case of #cardioonc associated valvulopathy and constriction. The hemodynamics of this case are 🤯. Thankful for the opportunity by my incredible mentor @datsunian
Check out this 🧵👇🏼 on our recent publication in @CircHF !
For more on the Heart Failure Guideline, explore ACC's #HeartFailure Guideline Hub. Here you will find patient resources, related education & resources, slides, apps, tools and more. https://t.co/Q0Ux5GaliM #ACC23#WCCardio
File this under “Epic.”
Over 100 Women IM residents who aspire to be cardiologists on a call with some of the nation’s foremost women cardiologists. Courtesy of @ACCinTouch’s #Diversity Committee. Only 13% of cardiologists are women. But the future is bright. Join us!
Very excited to be in the inaugural cohort of the ACC Women’s Internal Medicine program! Looking forward to learning from and meeting #WomenInCardiology mentors. Shoutout to my co-residents who are also representing @uclaimchiefs ! @ACCinTouch
Thankful to have learned from clinical masterminds like @AndreMansoor and @PeteSullivanPDx during my training. Hypotheses are generated with the history and PE — it’s just knowing what to ask, and where to look. Also, a plug for https://t.co/CjqljhS4nq.
1/9
A middle-age man presents with dyspnea on exertion, orthopnea, and weight gain. His BP is 112/40.
This should generate a hypothesis.
And you begin to test your hypothesis by evaluating for specific physical findings. What do you notice in this video?
Unique, multidisciplinary case of PCI in a pt with progressive angina + Glanzmann Thrombasthenia led by star UCLA IM resident @katieptr! To quote @drmortkern, a “zebra with polka dots” we hope folks learn from! @jcurrier17@marwahshahid
Our complex case of a patient with Glanzmann thrombasthenia🩸& high-grade CAD requiring PCI was published in @JACCJournals today!
⁃ Refresher: GT is a Gp IIb/IIIa receptor deficiency resulting in impaired platelet aggregation (1/3) https://t.co/bcVzhAcmuZ
Take aways:
➡️ Unclear if the mech of GT alone has adequate antiplatelet activity in setting of PCI
➡️ Antiplatelet agents such as ASA and P2Y12 inhibitors act on platelet activation
➡️ We propose short term DAPT course with mono therapy after PCI in patients with GT (2/3)
Grateful for the opportunity to present this interesting case showing the effects of chemoradiation on the heart leading to LBB pacing! ⚡️
The most common complications of radiation include:
🫀 Ischemic heart dz
🫀 Left sided valvular stenosis
🫀 Pericardial dz