WHY DOES SCALP COOLING WORK FOR TAXANES — BUT NOT FOR T-DXd?
The answer may be simple: it's a problem of exposure time.
✅ Taxanes → brief exposure → scalp cooling overlaps drug delivery → hair preservation is often possible.
⚠️ Anthracyclines → greater follicular toxicity → protection becomes less effective.
❌ T-DXd → DXd payload exposure may persist for ~5–6 days, while scalp cooling lasts only hours.
An umbrella can stop a storm.
It cannot stop a week of rain.
A biologic explanation for why scalp cooling appears most effective with taxanes, less effective with anthracyclines, and has not shown proven benefit with T-DXd.
#BreastCancer #ScalpCooling #TDXd #TrastuzumabDeruxtecan #Taxanes #Oncology #MedTwitter #OncTwitter #MVOnco
The full text of PADMA, presented at SABCS24, has now been published in @ESMO_Open
In predominantly postmenopausal patients with HR+/HER2− mBC considered to have an indication for chemotherapy, palbociclib + ET significantly prolonged PFS compared with mono-chemotherapy; no OS difference was observed.
RIGHT Choice tested ribociclib + ET against combination chemotherapy in a more aggressive pre/perimenopausal population and also showed a PFS advantage.
Both studies point in the same direction: in HR+/HER2− mBC, if there is no true visceral crisis(!), we should not start with chemotherapy.
https://t.co/lfH7pSAegu
#ASCO26 poster: High pCR with 12-week THP
NeoSphere, TRAIN-2, WSG-ADAPT HER2+/HR−, DAPHNe, CompassHER2-pCR/EA1181, neoCARHP, PHERGain, PHERGain-2, APHINITY, DB-05, DB-11...
Neoadjuvant therapy in HER2+ eBC continues to evolve.
Anthracyclines became less central. Carboplatin use became more selective. 12-week THP regimens generated consistent data. PET/pCR-adapted chemo-free anti-HER2 strategies were tested in selected patients. DB-05 showed EFS benefit with T-DXd in RD. DB-11 showed higher pCR with a neoadjuvant T-DXd-based approach.
This poster adds a small prospective series to the 12-week THP literature.
Seventy patients with early-stage HER2+ BC received 12 weeks of weekly paclitaxel + trastuzumab + pertuzumab.
No carboplatin.
No anthracycline.
Total duration: 12 weeks.
Overall pCR: 60%
HR−/HER2+ pCR: 82.1%
HR+/HER2+ pCR: 45.2%
Treatment completion: 100%
FN: 0%
Symptomatic cardiotoxicity: 0%
Most patients were stage IIA, and more than half were cN0. So I read this mainly in HR−/HER2+ disease with limited nodal burden.
My practical approach, based on these data and current access in my country, is roughly:
Stage I: adj TH (APT) — sometimes neoadj for T1c
Stage II: neoadj THP×4 or 6
Stage III: neoadj TCHP×6
If pCR: complete HP to 1 year.
If RD: HP (<1cm), T-DM1 or T-DXd in suitable patients.
For now, DB-05 is easier to translate into practice than DB-11. DB-05 has EFS data; DB-11 is still mainly a pCR story. In curative-intent disease, pCR helps, but EFS/OS matters more. I currently reserve T-DXd for high-risk RD, closer to the DB-05 setting.
🇮🇳 Practice-Changing ASCO 2026 Updates in Breast Cancer
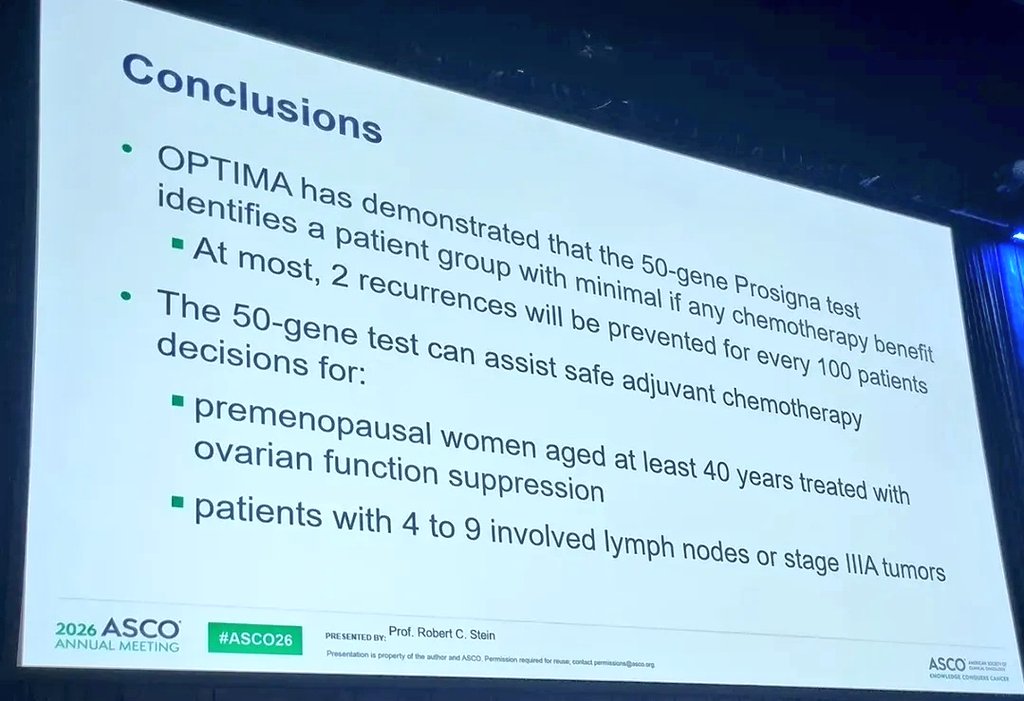
🔹 OPTIMA
• PAM50 genomics can help identify patients who may safely avoid chemotherapy
🔹 IRIS-A
• Selected Stage IA HER2+ tumors (≤0.5 cm) may not require taxane-based therapy
🔹 SENOMAC
• Some patients with 1–2 positive sentinel nodes can avoid completion ALND
🔹 ER-Low Analysis
• ER-low (1–10%) disease may behave differently from conventional HR-positive breast cancer
🔹 PATHWAY
• Tamoxifen remains a valid endocrine backbone with CDK4/6 inhibition
📌 Overall ASCO 2026 Message:
• Less chemotherapy
• Less surgery
• More precision
• More individualized treatment
#ASCO2026 #BreastCancer #Oncology #MedTwitter #MVOnco
Brilliant discussion at #ASCO26 by Prof Martine Piccart from @JulesBordet
One important take home message for our clinical practice from the OPTIMA trial ⬇️⬇️⬇️
@OncoAlert
#ASCO26 oral eBC: NATALEE biomarker data confirm broad RIB + ET benefit in HR+/HER2− eBC. Benefit was seen across PAM50 subtypes, with a trend for greater effect in high genomic-risk/proliferative tumors.
➡️ We are still missing predictive biomarker to better select pts that will actually benefit from CDK4/6i!
@ASCO@OncoAlert
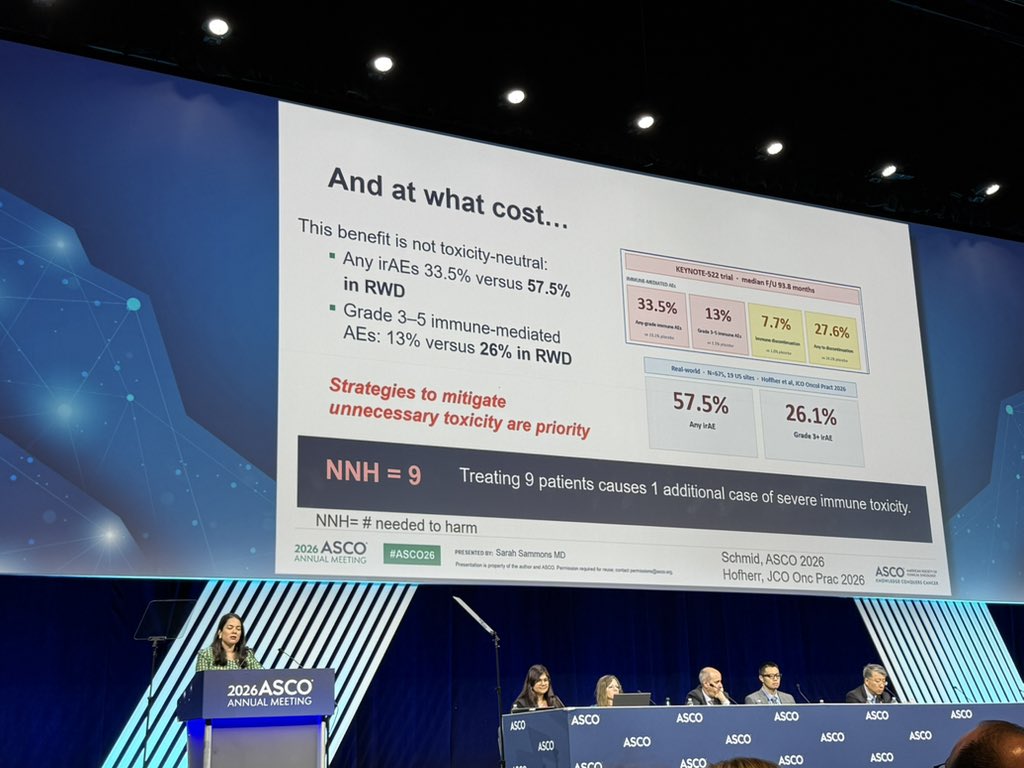
Tremendous discussion by @drsarahsam, highlighting the promise of several escalation/substitution strategies across breast cancer subtypes, but reminding the costs and caveat of each new option. #ASCO26
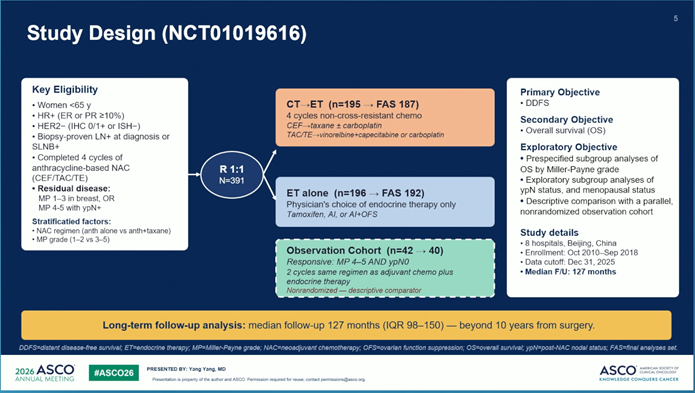
📌 Updated overall survival results from a randomized phase III trial of non-
cross-resistant adjuvant
chemotherapy plus endocrine
therapy versus endocrine therapy alone in HR+/HER2-/lymph node-
positive breast cancer with residual
disease following neoadjuvant
chemotherapy (NCT01019616).
Presented by Yang Yang
#ASCO26 @OncoAlert #OncoAlertAF #BreastCancer
OPTIMA Redefines Adjuvant Therapy in HR+/HER2− Breast Cancer
Molecular risk not nodal burden alone, should guide chemotherapy decisions.
Prosigna-directed de-escalation maintained excellent outcomes while reducing overtreatment.
#ASCO26#BreastCancer@OncoAlert#bcsm@ASCO
#ASCO26 A randomized clinical trial shows that post-neoadjuvant CT+ET vs ET alone⬆️non-significantly DDFS (primary endpoint) and OS (significant - secondary endpoint) in pts with ER+/HER2-neg BC with residual disease at surgery post NACT
@OncoAlert
#ASCO26
KEYNOTE-522 final analysis
Median follow-up: 7.8 years.
Neoadjuvant pembro + chemo followed by adjuvant pembro maintains its long-term OS benefit in high-risk early-stage TNBC.
7-year OS: 85.1% vs 77.2%
pCR achieved: OS 94.5% vs 91.1%
HR: 0.64; 95% CI 0.37–1.14
#ASCO26
ER+, HER2- breast cancer management is becoming less about “one-size-fits-all” and more about precision escalation vs precision de-escalation.
The future is clear:
🧬 Biomarkers decide who gets chemo
💊 CDK4/6 inhibitors move earlier
🩺 Endocrine therapy intensifies in high-risk disease
⚖️ Obesity and supportive care become survival interventions
Key themes from ASCO 2026:
▪️ Anthracyclines may still matter in selected genomically high-risk patients
▪️ Some node+ patients may safely avoid chemotherapy
▪️ OFS + AI remains critical for high-risk premenopausal disease
▪️ Adjuvant abemaciclib and ribociclib continue reshaping standards
▪️ Oral SERDs are entering early breast cancer
▪️ Weight management may become part of oncologic care itself
Breast oncology is shifting from anatomy-driven to biology-driven treatment selection.
Which biomarker do you think will have the biggest impact in early ER+ breast cancer over the next 5 years? 👀
@OncoAlert@ASCO@myesmo@esmo_open@larvol
#OncoTwitter #MedTwitter #BreastCancer #bcsm #PrecisionOncology
Current approved treatment options for HR+, HER2− mBC
ESMO Guidelines: Real World Cases Webinar: Metastatic Breast Cancer 2026 presentation
https://t.co/H3S9DZXsK2
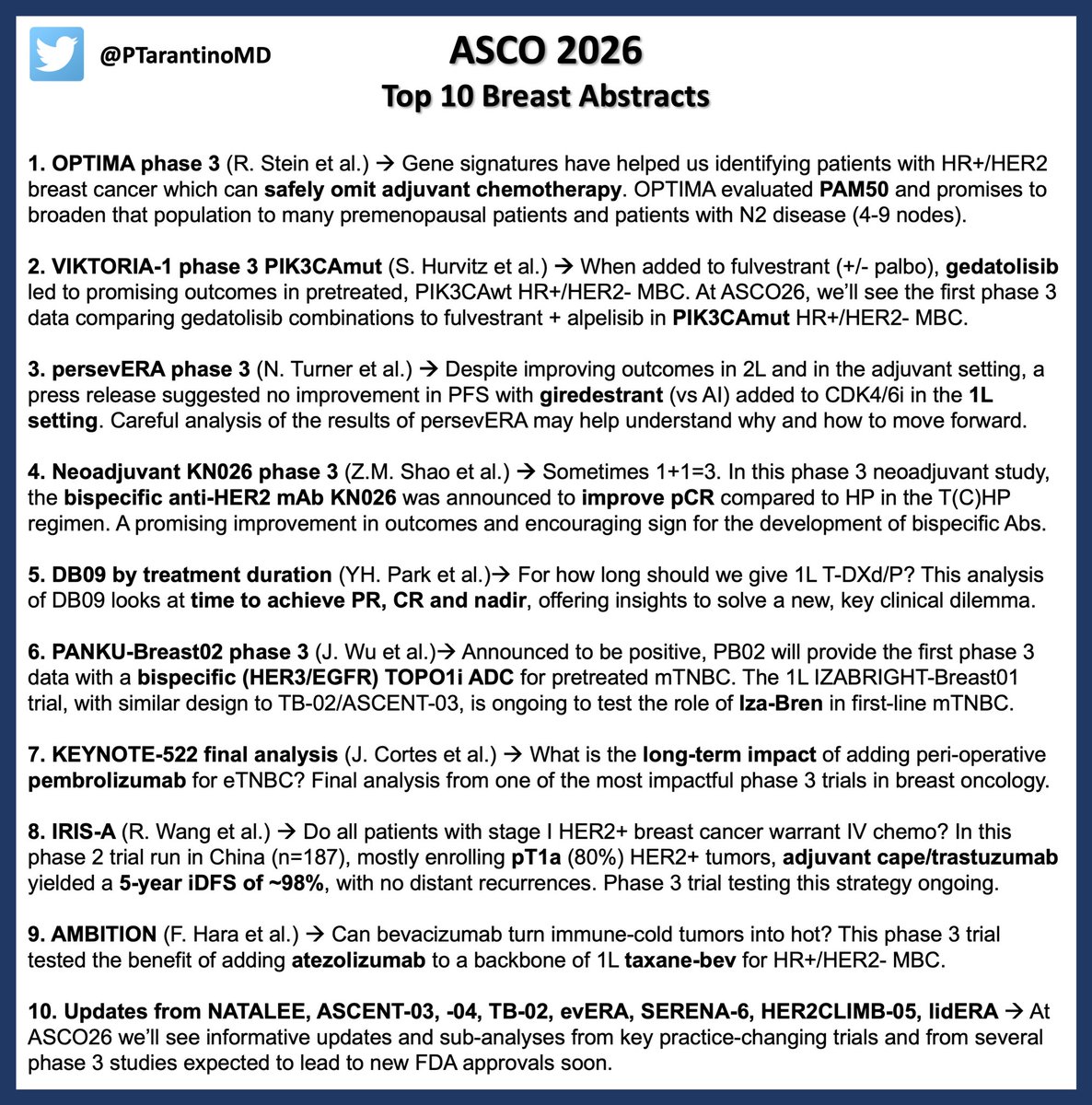
Only few days to #ASCO26. For breast oncologists, this edition will deliver a new promising biomarker to spare unnecessary chemo, informative updates from practice-changing trials across subtypes, and major innovations coming from China. See you in Chicago next week! #bcsm
Interesting data showing that upfront SLNB may be reasonable for select patients presenting with cN1 HR+/HER2- breast cancer - no recurrences in those with at least 12 months of f/u at time of analysis
What happened this week in #BreastCancer:
1⃣ FDA approval of PROTAC ER degrader in ESR1m
Regulatory clearance of vepdegestrant for ER-positive, HER2-negative, ESR1-mutated advanced or metastatic disease after endocrine therapy based on VERITAC-2 positions it as a new post CDK4/6i endocrine option with improved PFS vs fulvestrant and necessitates ESR1 testing via the simultaneously approved companion diagnostic to detect ESR1 mutations.
https://t.co/ACXPAzbwkY