Should we continue cetuximab beyond first line in RAS/BRAF WT metastatic colorectal cancer? 🤔
The #ESMOGI26 CAPRI-2 GOIM trial suggests the answer may depend on ctDNA hyperselection. 🧬
Patients with:
✅ RAS/BRAF V600E WT
✅ MSS mCRC
✅ No acquired resistance alterations on plasma ctDNA (“negative hyperselected”)
derived substantial benefit from continuing cetuximab while switching chemotherapy.
1L: FOLFIRI + Cetuximab
📈 ORR: 78% vs 54% (OR 3.0; P=0.003)
📈 mPFS: 13.8 vs 9.6 months (HR 0.55)
2L: FOLFOX + Cetuximab
📈 mPFS: 8.3 vs 4.7 months (HR 0.43; P=0.003)
📈 OS: NR vs 22.4 months (HR 0.47; P=0.001)
Take-home 🎯
Instead of automatically discontinuing anti-EGFR therapy after progression, serial ctDNA profiling may identify patients who can continue benefiting from cetuximab across treatment lines.
This moves us one step closer to dynamic, biomarker-guided treatment sequencing in metastatic CRC.
Will ctDNA-guided anti-EGFR continuation become the new standard?
@myESMO@OncoAlert
#ESMOGI26 #ColorectalCancer #ctDNA #PrecisionOncology
🧬 Largest Real-World Evidence for Neoadjuvant Immunotherapy in dMMR/MSI Colorectal Cancer
Key findings from the AGEO-NEO-MSI study presented at ESMO GI 2026:
✅ 316 patients across 30 international centers
✅ 67% complete response (CR) overall
✅ Organ preservation with non-operative management:
• 25% in colon cancer
• 77% in rectal cancer
✅ Pathological CR: 64%
✅ 24-month event-free survival: 86%
✅ Grade ≥3 immune-related adverse events: 6.3% (more frequent with dual ICI)
Take-home message:
These real-world data support neoadjuvant immune checkpoint inhibitors as an effective strategy for localized dMMR/MSI colorectal cancer, with high complete response rates and substantial opportunities for organ preservation—particularly in rectal cancer.
📖 Reference: Gandini A, Overman MJ, et al. AGEO-NEO-MSI Study. Rapid Oral Presentation, ESMO GI Congress 2026.
#ESMOGI2026 #ColorectalCancer #dMMR #MSI #Immunotherapy #Neoadjuvant #Oncology #OncoTwitter #MedTwitter #MVOnco
SBRT vs Microwave Ablation for Colorectal Liver Metastases
LAVA-CRLM Phase II Trial | ESMO GI 2026
Key findings:
• Randomized phase II trial in patients with 1–3 colorectal liver metastases (≤4 cm)
• 1-year freedom from local progression: SBRT 83.0% vs MWA 77.7% (HR 0.87; P=0.70)
• Significantly lower toxicity with SBRT:
• Grade ≥2: 3% vs 25%
• Grade ≥3: 0% vs 8%
• One treatment-related death occurred in the MWA arm.
Clinical takeaway:
For carefully selected patients, SBRT provides comparable 1-year local tumor control with substantially lower toxicity, making it an attractive non-invasive local treatment option where expertise is available.
Reference:
LAVA-CRLM Phase II Trial • Rapid Oral Presentation • ESMO GI 2026
https://t.co/CPwTJ8KDHF: NCT03654131
#ESMOGI2026 #ColorectalCancer #LiverMetastases #SBRT #RadiationOncology #SurgicalOncology #Oncology #MedTwitter #MVOnco
ESMO GI 2026 is almost here.
After going through the scientific program, these are the 10 trials I’m watching most closely 👇
1️⃣ KRYSTAL-10
Can KRAS G12C-targeted therapy finally outperform chemotherapy in second-line mCRC?
2️⃣ STAR-221
Will TIGIT become the next immunotherapy breakthrough in advanced gastric cancer?
3️⃣ ATOMIC
Could this redefine the duration of adjuvant chemotherapy and immunotherapy in dMMR colon cancer?
4️⃣ TRIPP-FFX
A novel intratumoral radiation strategy aiming to improve outcomes in locally advanced pancreatic cancer.
5️⃣ EMERALD-1 (OS Update)
The overall survival results that could strengthen immunotherapy + TACE in HCC.
6️⃣ GALAXY ctDNA
Can postoperative ctDNA truly guide adjuvant therapy after colorectal liver metastasis resection?
7️⃣ BREAKWATER Biomarker Analysis
Who benefits the most from first-line encorafenib + cetuximab ± mFOLFOX6?
8️⃣ KANDLELIT-001
The first major efficacy update of next-generation KRAS G12C inhibitor calderasib (MK-1084).
9️⃣ GLEAM
Can CLDN18.2-targeted therapy expand beyond gastric cancer into pancreatic cancer?
🔟 Zoldonrasib + Chemotherapy
Early first-line data for one of the most anticipated KRAS G12D inhibitors in pancreatic cancer.
I’ll be covering every major study with concise summaries, infographics, and clinical takeaways throughout the meeting.
Which trial are you most excited about?
#ESMOGI26 #ESMOGI #oncology @myESMO@OncoAlert
PATINA is now an FDA-approved standard.
One year after the practice-changing data, the FDA has officially approved palbociclib + trastuzumab (± pertuzumab) + endocrine therapy as maintenance for HR+/HER2+ metastatic breast cancer.
PATINA
• HR+/HER2+ LA/MBC after induction taxane + trastuzumab ± pertuzumab
• Palbociclib + anti-HER2 + ET vs anti-HER2 + ET
• PFS: HR 0.76 (95% CI 0.59-0.97; P=0.0134)
• OS: Not mature
This is the first FDA approval of a CDK4/6 inhibitor in HER2-positive metastatic breast cancer and formally establishes maintenance CDK4/6 inhibition as a new treatment standard.
Will PATINA change your first-line maintenance approach?
@FDAOncology@ASCO@myESMO@OncoAlert@Pfizer
#BreastCancer #HER2 #MedTwitter #Oncology
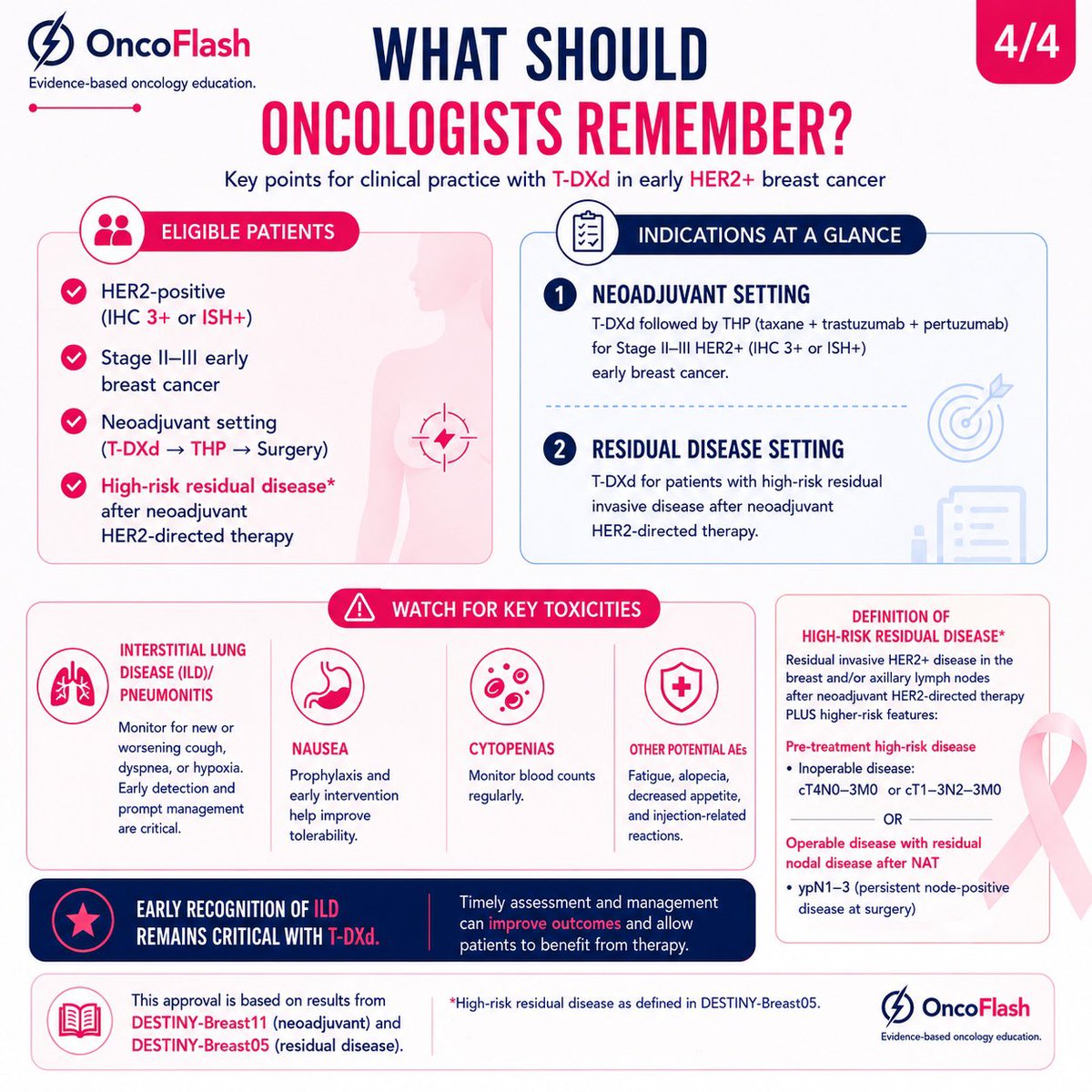
HER2+ THERAPY IS BECOMING RESPONSE-ADAPTED
A simple algorithm proposed by Tarantino et al. (JCO 2026):
▪️ Stage IIA → THP → Surgery → HP
▪️ Stage IIB → THP → Response assessment → Continue THP or escalate to T-DXd
▪️ Stage III → TCHP or THP → T-DXd → Surgery
▪️ pCR → Complete planned HER2-directed therapy
▪️ Residual disease → T-DXd or T-DM1
The concept is simple:
✓ Stage
✓ Biology
✓ Treatment response
Together determine treatment intensity.
We are moving beyond a one-size-fits-all approach toward more personalized HER2-directed therapy.
Adapted from Tarantino et al., JCO 2026.
#BreastCancer #HER2 #HER2Positive #Oncology #JCO #ASCO #TDXd
Postmenopausal HR+ Breast Cancer
How long should we continue Aromatase Inhibitor therapy — 5, 7, or 10 years?
New high-yield infographic with risk-stratified approach:
• High risk (≥4 nodes, T3/T4, Grade 3, high CTS5, multiple adverse features) → Consider 10 years
• Intermediate risk (1–3 nodes, T2 without multiple adverse features) → ~7 years often adequate
• Low risk (T1N0, low grade, low genomic risk) → 5 years is enough
Includes key evidence (MA.17R, NSABP B-42, ABCSG-16) + practical viva one-liner.
Important nuance: Extending to 10 years gives only small additional benefit over 7 years for many patients, but comes with more bone toxicity.
Save for clinic or exam prep!
What’s your current practice for intermediate-risk patients with good tolerance?
#BreastCancer #Oncology #EndocrineTherapy #AdjuvantTherapy #MedTwitter #HRPositiveBreastCancer
Axillary treatment options in clinically node-positive breast cancer whose nodes become pathologically node-negative after neoadjuvant chemotherapy: a pairwise and network meta-analysis
https://t.co/lO9YSrEPF9
Desmoid Fibromatosis (Aggressive Fibromatosis) – Management Algorithm
The treatment landscape has changed.
Active surveillance is now the preferred first step for most patients.
Surgery is no longer routine first-line.
Nirogacestat (gamma-secretase inhibitor) has become the preferred systemic therapy for progressive disease based on the DeFi trial.
This high-yield infographic covers: • What it is & key mutations (CTNNB1 / APC) • Initial workup (biopsy, imaging, molecular) • When to treat (clear indications) • Limited role of surgery & radiotherapy today • Systemic options: Nirogacestat (preferred), TKIs, chemotherapy • Hormonal/NSAIDs – why they’re no longer routine • FAP-associated desmoid management • Practical exam algorithm + viva pearls
Perfect for residents, fellows & exam prep (DrNB/Medical Oncology).
Save it for quick reference. Share with your team.
What’s your current approach for a progressive mesenteric desmoid in a young patient?
#Desmoid #DesmoidTumor #AggressiveFibromatosis #Sarcoma #Oncology #MedicalOncology #CancerEducation #MedEd #ClinicalPearls
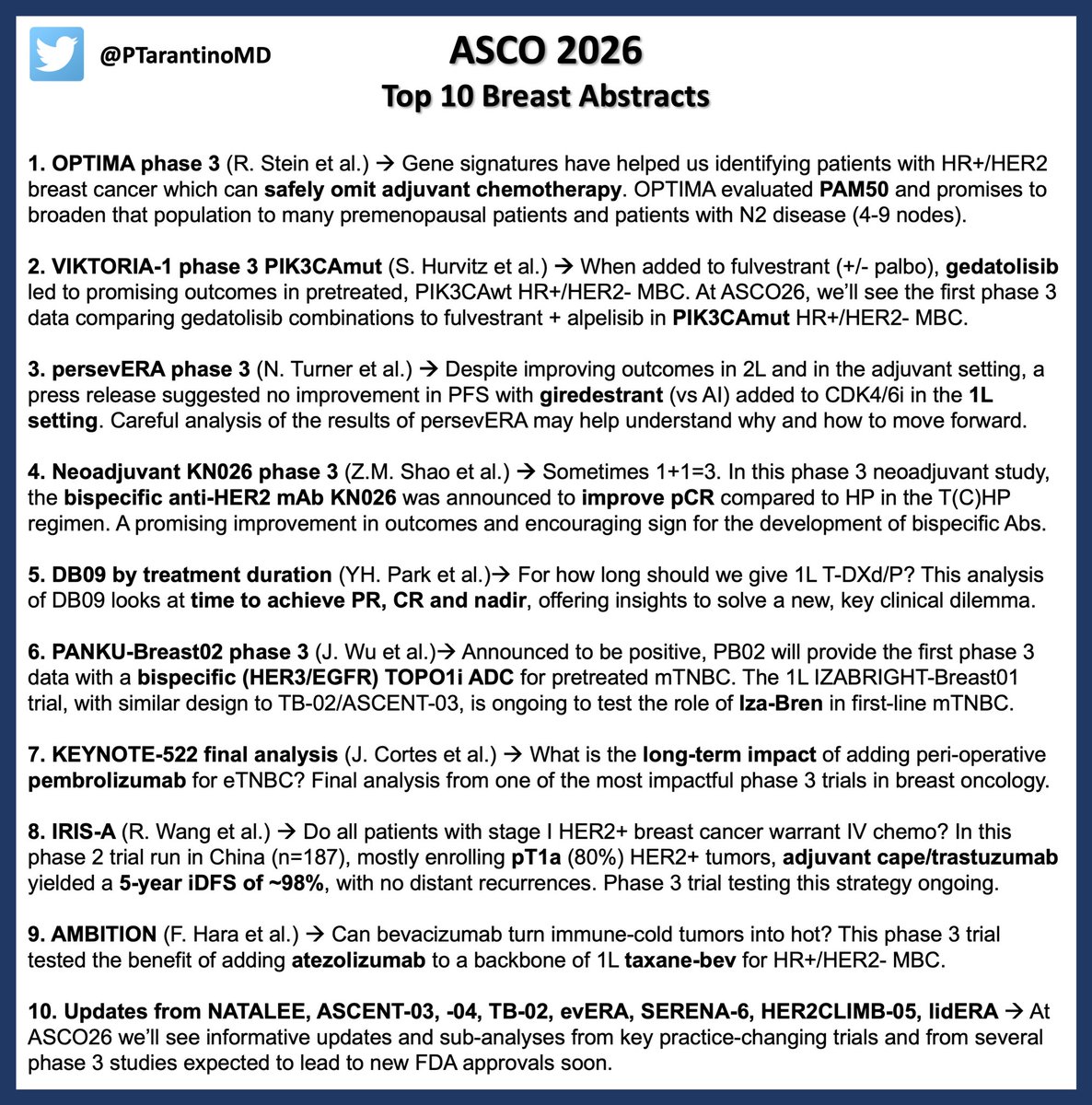
Only few days to #ASCO26. For breast oncologists, this edition will deliver a new promising biomarker to spare unnecessary chemo, informative updates from practice-changing trials across subtypes, and major innovations coming from China. See you in Chicago next week! #bcsm
🔬 MSI-High / dMMR Rectal Cancer After Neoadjuvant Immunotherapy with Complete Response: What Next?
In the rapidly evolving landscape of precision oncology, patients with localized MSI-High (MSI-H) or deficient mismatch repair (dMMR) rectal adenocarcinoma are benefiting from one of the most dramatic paradigm shifts in gastrointestinal cancer care.
Neoadjuvant immunotherapy — using agents such as dostarlimab, pembrolizumab, nivolumab ± ipilimumab — can produce extraordinarily deep and durable responses. Many patients achieve clinical complete response (cCR) or even pathologic complete response (pCR), raising a critical question:
“If the cancer is gone, do we still need surgery?”
The Key Principle
For MSI-H/dMMR rectal cancer, the goal is clear:
Avoid overtreatment while maintaining cure.
Immunotherapy-first strategies now allow selected patients to safely pursue organ preservation through non-operative “Watch-and-Wait” management when a sustained complete response is confirmed.
What the Infographic Breaks Down:
• Clinical scenario for neoadjuvant IO followed by cCR/pCR
• A. Non-operative management (“Watch-and-Wait”) – preferred when sustained cCR is achieved → No immediate surgery, no chemoradiation, no routine adjuvant chemotherapy
• B. Post-surgical true pCR (ypT0N0) → Observation + surveillance only
• Why this works MSI-H tumors are highly immune-sensitive → exceptional pCR/cCR rates Surgery carries real long-term risks: permanent colostomy, infertility, sexual dysfunction, bowel issues, neuropathy
• Evidence that changed the game Dostarlimab MSKCC study (and supporting trials) → very high clinical complete response rates, many patients avoided surgery entirely, durable responses maintained on long-term follow-up
• Strict surveillance protocol (MRI pelvis, endoscopy, DRE, CEA, selective CT) — essential because cCR ≠ pCR (microscopic disease can still exist)
• 2025–2026 Practical Standards table: clear next steps for cCR without surgery, pCR after surgery, residual disease, or progression
• Unresolved questions still evolving: optimal IO duration, role of radiation omission, long-term regrowth risk, ctDNA, ideal patient selection
This approach represents one of the biggest modern advances in GI oncology: Immunotherapy-first organ preservation for MSI-H/dMMR localized rectal cancer — combining evidence, precision, and quality-of-life focus.
Designed as a quick, high-yield reference for oncologists, surgeons, radiation oncologists, fellows, residents, and anyone involved in rectal cancer care.
📌 Save • Share • Discuss
What are your experiences with IO-first strategies in MSI-H rectal cancer? Have you adopted Watch-and-Wait in your practice?
Follow for more visual, evidence-based explanations of complex oncology concepts.
Dr Rupam Manna, MD
Medical Oncologist
X: @DrRupamOncology
#RectalCancer #MSIHigh #dMMR #Immunotherapy #OrganPreservation #WatchAndWait #PrecisionOncology #CancerResearch #GIOncology #pCR #NeoadjuvantTherapy
What to see in a Breast Mammogram – A Systematic Approach 🔥
Step-by-step guide to reading mammograms like a pro:
✓ Basic details
✓ Density (A–D)
✓ Masses, calcifications, distortion
✓ Asymmetries, skin/nipple, axilla
✓ Prior comparison → BI-RADS
Fully aligned with the latest ACR BI-RADS® v2025 Manual (Dec 2025 update). Minor calcification terminology refinements only — core teaching points remain unchanged.
Perfect for residents, oncologists, radiologists & anyone wanting to understand breast imaging better.
Save & share! 👇
#BreastCancer #Mammogram #BIRADS #Radiology #BreastImaging #CancerAwareness #MedEd #Oncology
Follow for more: @DrRupamOncology
🚨 2026 Melanoma Management Algorithm – Fully Updated!
The definitive practical guide for cutaneous melanoma is here.
Key 2026 update:
✅ Perioperative immunotherapy is now preferred for resectable macroscopic Stage III (clinically positive nodes, satellites/in-transit, nodal recurrence)
→ Neoadjuvant PD-1 ± CTLA-4 (or relatlimab) → Surgery → Response-adapted adjuvant therapy (NADINA + SWOG S1801)
Plus:
• Precise surgical margins & SLNB criteria
• BRAF-driven decision tree for Stage IV
• Brain mets, mucosal & uveal melanoma pathways
• Current preferred philosophy & landmark trials
Aligned with NCCN v2.2026 & ESMO 2025. Designed for real-world oncology practice.
Save this. Share with your team. Use it daily.
What’s your biggest takeaway from the new perioperative approach? Drop it below 👇
Follow for more high-yield cancer algorithms → @DrRupamOncology
#Melanoma #Oncology #Immunotherapy #NCCNGuidelines #CancerCare #MedEd
Survival and Recurrence With GLP-1 Receptor Agonists in Breast Cancer
A provocative signal, but not yet an anticancer effect
1. Retrospective EHR-based study; association does not prove causality.
2. High risk of residual confounding despite propensity score matching.
3. Possible healthy-user effect: GLP-1 RA users may have better follow-up, access, adherence, and metabolic care.
4. Strong calendar-time bias: GLP-1 RA use increased in more recent years, when breast cancer care also improved.
5. Weak exposure definition: ≥2 prescriptions do not prove sustained treatment.
6. No time-varying exposure model; immortal-time bias may persist.
7. Landmark analyses reduce bias but do not replace proper time-varying modeling.
8. The signal weakens against the active comparator SGLT2 inhibitors.
9. Insulin/metformin is a problematic comparator because it may represent a sicker diabetes population.
10. Limited tumor biology: ER/HER2 status, grade, nodal burden, tumor size, Ki-67, and genomic risk are inadequately captured.
11. ER-positive rates appear unrealistically low, suggesting incomplete EHR capture.
12. Cancer treatment data appear incomplete; surgery and radiotherapy rates look clinically implausible.
13. RFS is code-based, not a true clinical recurrence endpoint.
14. No breast cancer–specific survival; all-cause mortality may reflect cardiometabolic benefit rather than anticancer effect.
15. No competing-risk analysis despite substantial non-cancer mortality risk.
16. No weight-loss data; the actual metabolic effect is unknown.
17. Effective follow-up is short despite reporting 10-year estimates.
18. Few patients remain at risk beyond 5 years, weakening 10-year KM estimates.
19. High administrative censoring limits late outcome interpretation.
20. Mechanism remains unclear: anticancer effect, weight loss, metabolic control, or patient selection?
https://t.co/gWWEIUTSi5
Stage I TNBC is not “low-risk by default.”
We still treat by tumor size.
But the real story is biology.
Here’s where the field stands 👇
🧩 Current approach (size-driven)
T1mic/T1a → often no chemo
T1b → surgery ± adjuvant chemo
T1c → neoadjuvant chemo
⚠️ Problem:
Stage I patients were largely excluded from major trials.
🧬 Biology is changing decisions
High TILs
→ Excellent outcomes even without chemo
→ Being tested in OPTImal, ETNA, TIL-CHOICE
Low TILs
→ Higher relapse risk despite small tumor
→ May need escalation
💊 Anthracycline debate (still unresolved)
• ABC trials → slight iDFS benefit
• PlanB / SUCCESS C → no OS benefit
• EBCTCG meta-analysis → modest recurrence reduction
👉 Net: small gains vs real toxicity
💡 Anthracycline-free strategies
• PATTERN → Cb + taxane ↑ DFS
• NeoSTOP → similar pCR, less toxicity
• WSG-ADAPT-TN → response-adapted de-escalation
🧪 Immunotherapy + de-escalation
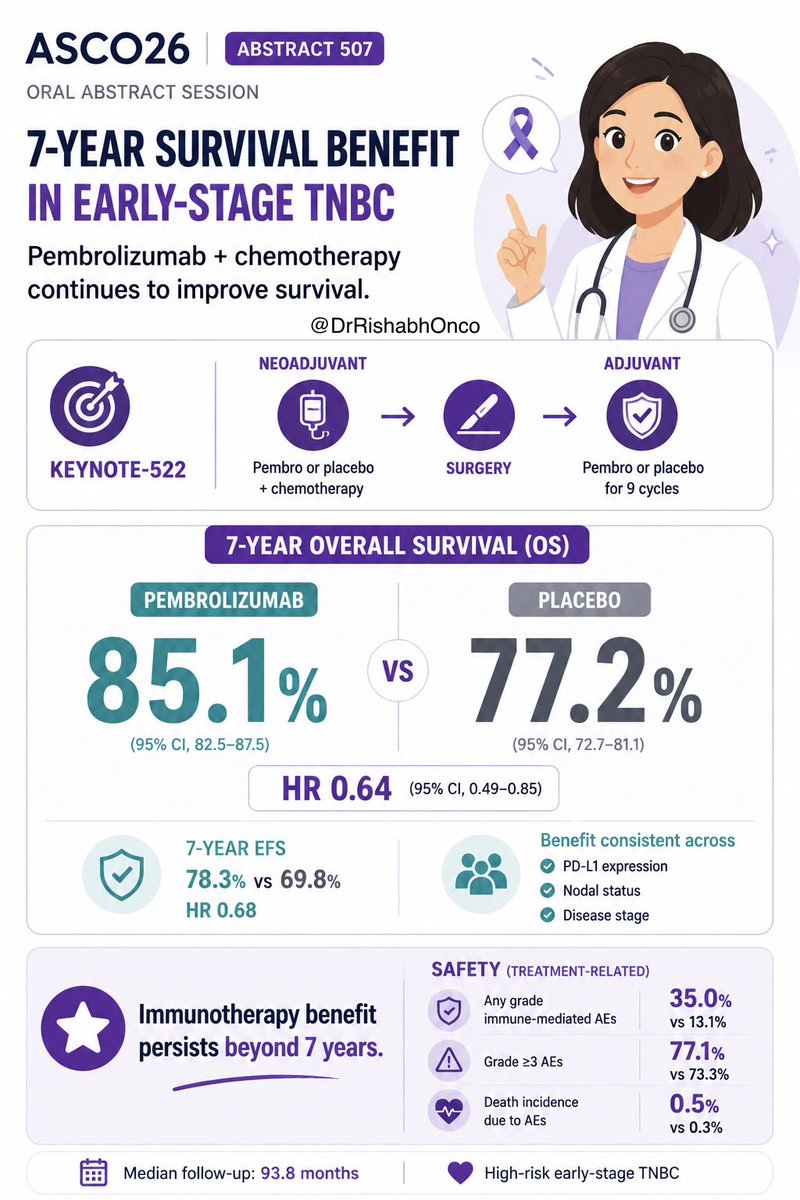
• KEYNOTE-522 → standard in stage II–III
• NeoPACT, Neo-N → strong pCR signals
• SCARLET (ongoing) → testing chemo de-escalation
🧬 gBRCA subgroup
• NEOTALA, OlympiaN, TBCRC 056
→ PARP inhibitor–based chemo-free strategies emerging
🔮 Where we are going
From: Tumor size alone
To:
Tumor size + TILs + genomics + ctDNA + response
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #BreastCancer #TNBC
@OncoAlert@myesmo@asco@JCO_ASCO@esmo_open