Great presentation by Dr. Pavlos Msaouel. Panitumumab-based EGFR blockade in SMARCB1-deficient renal medullary carcinoma: ORR 53.9% (15.4% CR) and mOS 9.5 mo in heavily pretreated pts, far exceeding historical benchmarks. Wild-type EGFR dependency as a new therapeutic vulnerability in this rare, aggressive disease. #ASCO26 #RCC @OncoAlert@ASCO@OncBrothers
Durvalumab + BCG is FDA approved in high risk NMIBC , by hitting its DFS - HR 0.68 (plus a ~⬇️ cystectomy rate). OS & M1 data show these patients have low cancer mortality & IO has about a 10% chance of serious side effects. Therefore, this is not a treatment for all HR NMIBC IMO. It’s hard to know who to select. Inconsistency with other data for Sasanlimab + atezo means there is no subset that consistently benefits. It will be interesting to see whom urologists recommend for treatment. #ASCO26 https://t.co/12cmVfA6Rl
@staceyabrams Thank you. My great grand father fought for the Union (Iowa Volunteers). He was captured by the south and escaped. He survived because he was hidden in the quarters of enslaved people and directed to the underground railroad.
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
Shortly before 3am on June 4, 1993, a mechanic at Miami airport looked in the wheel well of a DC-8 cargo jet from Bogotá. He saw the body of a teenager, curled in a ball, wearing only a t-shirt and shorts and frozen like an "ice cube."
The first paramedic pronounced him dead. The second found a weak pulse.
Somehow he had just survived 5 hours at 35,000 feet without heat or air pressure.
This should have killed him three different ways.
A🧵& blog post on how he survived.
1/
LBA1/Plenary #ASCO26: PROTEUS trial
Perioperative apalutamide + ADT vs. placebo + ADT with radical prostatectomy in HR localized or locally advanced PC
Our very own #DrMaryEllenTaplin from @DanaFarber_GU will take the stage at #ASCO26 and present phase 3 PROTEUS trial. This is a key multimodal treatment question and could shift the paradigm on how we think about systemic therapy in the perioperative setting. Dr Taplin has worked on countless Neoadjuvant Strategies in prostate cancer and it is rewarding to see her work materialize at the big stage !
@DanaFarber@DanaFarber_GU@ASCO@OncoAlert
Shocking disparities in utilization of essential cancer meds across the US. Or maybe not so shocking anymore . By the way, if you want great care, start in Massachusetts @DanaFarber
The final analysis (9 year follow up) of checkmate 214 (IPI/Nivo vs sunitinib - 1st line RCC) @Annals_Oncology. Durable remissions with 31% 9 yr OS. Long-term benefit for IMDC good risk despite lower initial response rates (HR 0.80). OS HR for int/poor at 0.68. It remains a standard of care, and the best 1st line option for some (including good risk). @DrChoueiri@OncoAlert
In 1980, DeBakey operated on the Shah of Iran. He declares success. Soon, the patient is dead. Reoperation is psychologically brutal: how bias delay truth & what might save us from the same trap. https://t.co/5nZdjJEcmA #MedTwitter#Surgery#MedEd
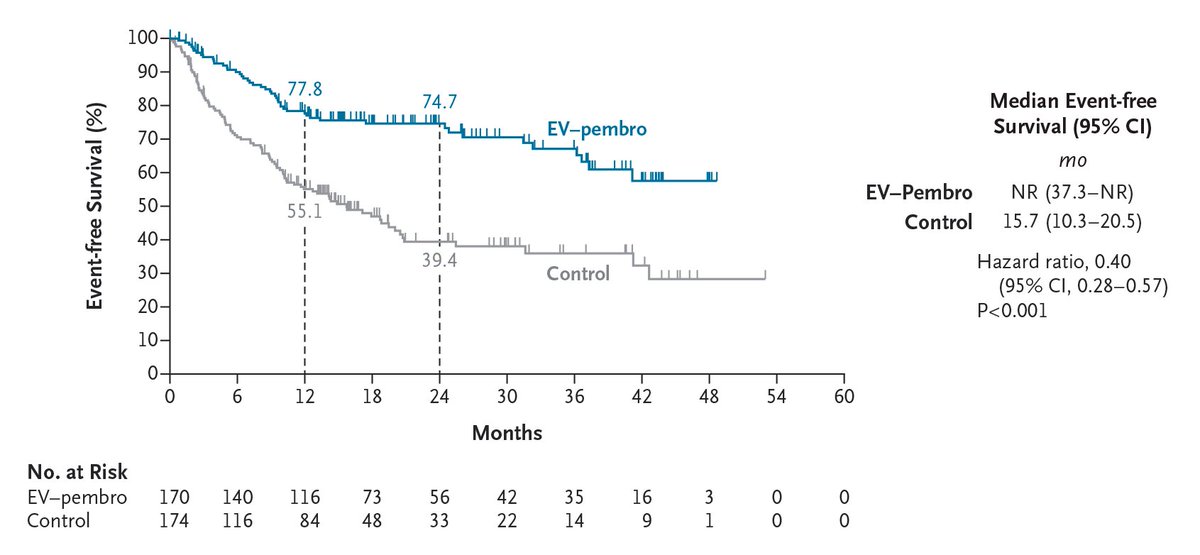
In cisplatin-ineligible patients with muscle-invasive bladder cancer, enfortumab vedotin–pembrolizumab plus surgery led to better event-free survival (74.7%, vs. 39.4%) and overall survival (79.7%, vs. 63.1%) than surgery alone at 2 years. Full phase 3 KEYNOTE-905/EV-303 trial results: https://t.co/6M3xhml0ou
Editorial: Enfortumab Vedotin plus Pembrolizumab as Perioperative Therapy https://t.co/3uNr9TUukQ
Very interesting. We can get a bit sidetracked by CRS and possible ICANs risk with bispecific antibodies. And yes, important to manage properly. But infection is what we must always be on the look out for with these agents.