Interesting to take part in today’s panel debate with @NIH Director, Dr Jay Bhattacharya @DrJBhattacharya , at a USC event hosted by Dean Carolyn Meltzer and Dr Neeraj Sood (USC School of Public Policy). Some takeaways:
💡The NIH budget will likely remain flat next year, but an increase in “forward funding” (now 37% of grants, up from 20%) will likely mean fewer grants awarded. Forward funding is intended to allow projects to spend much more in their first year than if the budget was constant in all years, and some investigators, e.g. a junior researcher, may need initially larger funding to set up their lab.
💡If a clinical trial is fully funded at the start, it avoids having nothing to show if each continuation year depends on annual funding appropriations (which are unstable). Forward-funding leads to a temporary very large drop in numbers of grants awarded but “at equilibrium” the same number of grants will be awarded.
💡Calls to increase the 500k/year budget for R01s (the standard type of NIH grant) have to be carefully balanced with the recognition that raising this would lead to fewer grants overall.
💡There is very high priority on reproducibility of research, as not prioritizing this has led to loss of public trust in science. Consortia can address this. Some audience members (incl Rob McConnell) noted it might make sense to expand reproducibility to include experimental work where multiple lines of converging evidence point to a conclusion, from multiple different approaches, rather than just repeating the experiment. But this can be expensive.
💡Paylines (where the top x% of grants are funded, and x is known) are being replaced by a system where NIH institute directors and POs have more discretion. This is because the top-N by score may not be necessarily more impactful than the best selection of grants that collectively as a portfolio could make the greatest impact. If there is redundancy, this can be traded off by funding a lower-scoring grant with higher risk/higher impact.
💡Foreign components on grants are welcome, but must use the new PF5 format with higher expectations of auditing and reporting for the foreign site, including making primary research records available to the funder via the prime site. Foreign subawards are no longer being used as they involve less oversight which can lead to loss of public trust.
💡Panelists noted the need to speed up reviews and the time-to-funding, which has greatly increased. Dr Bhattacharya noted that some ideas take time to incubate in the community before they can be reliably funded, whereas others (perhaps AI, clinical trials) can lose impact if delayed or review is too slow.
💡There is a proposal being entertained that K awards (for junior faculty) be given as an allocation to the institution to give out to people they vet, rather than directly awarded.
💡NIH wants to “spread out” funding to more institutions, across more of the country, to reduce the concentration of funding at some institutions.
💡Innovation is sometimes killed by reviewers who put too much emphasis on the certainty of the approach working. Often Aims 2 and 3 of a project depend on a high-risk, high-payoff Aim 1 working. Forward funding of 2-3 years can allow a checkpoint to be included on a high-risk Aim, before more funding.
💡Thank you to @KECKSchool_USC for hosting the event, and to Neeraj Sood for his "Open Dialogues" project.
A remarkable result supported by remarkably clean data.
A recent study published in Cell tackles a difficult and important question:
Can a routine vaccine influence dementia risk?
Instead of relying on correlations, they use a quasi-experimental design built around age-based eligibility for the shingles vaccine. Individuals just above and below the cutoff are nearly identical, except for vaccination status. This creates a rare opportunity in human populations: something close to randomization at scale.
The result: vaccinated individuals show a lower incidence of dementia over time. The separation is gradual, internally consistent across analyses, and robust to multiple checks. Even among people already diagnosed with dementia, vaccination is associated with slower progression and lower mortality.
No mechanism is claimed. No overreach. Just a clear signal from a well-constructed natural experiment.
The implication is hard to dismiss: a single, widely used vaccine — given for an unrelated reason — may meaningfully alter the trajectory of one of the most complex diseases in medicine.
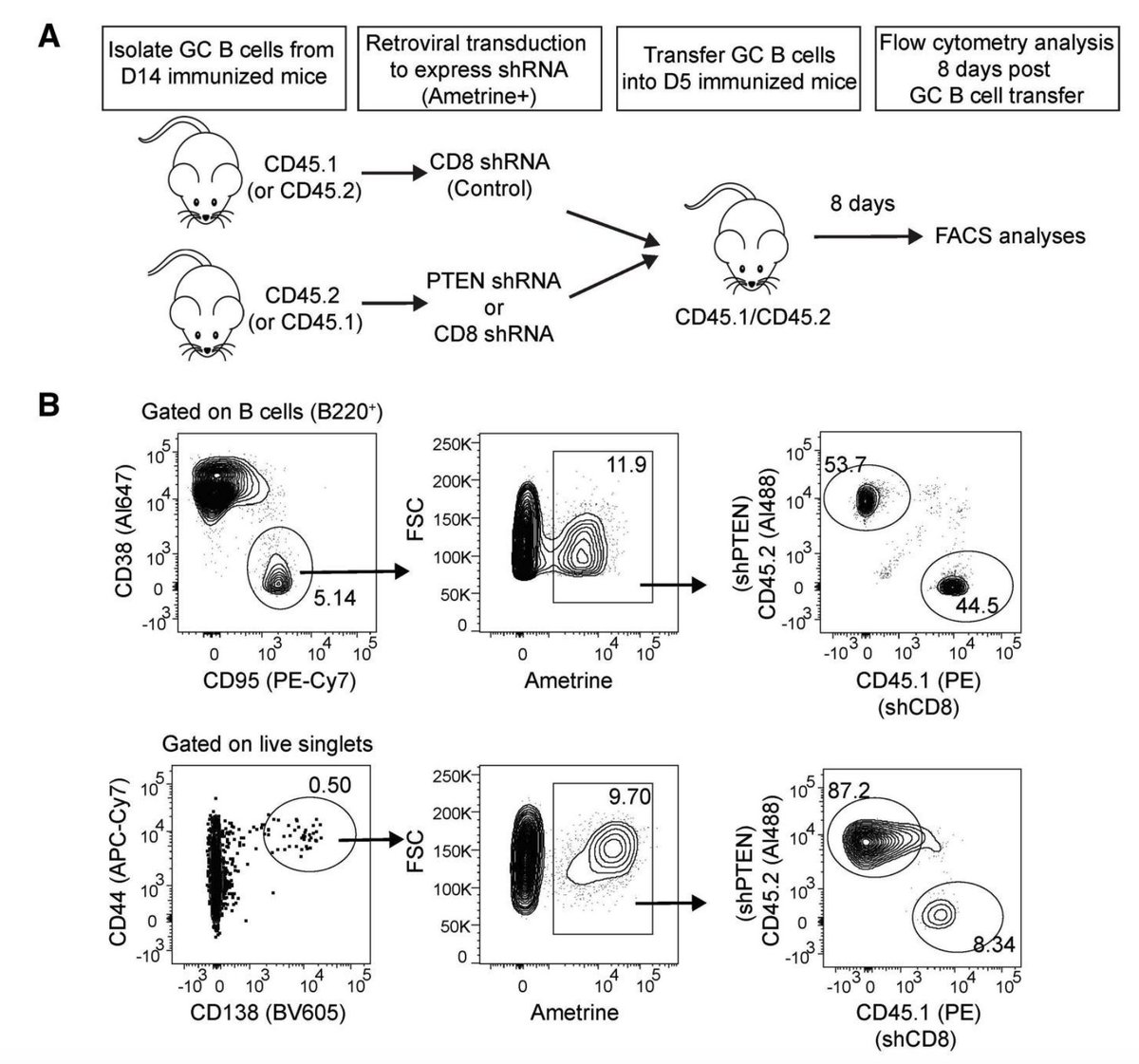
This November #TopRead from @luoweicool and @ShlomchikLab demonstrated that PTEN deficiency selectively expanded germinal center B cells in Peyer’s patches but had no impact on those induced by immunization, revealing an unknown role for PTEN. Read more: https://t.co/Yy6OzLobNO.
Thrilled to share our new publication in
@NatImmunol - Huge credit to my postdoc @HaoxinZhao and team for their hard work and persistence, and sincere thanks to our fantastic collaborators who made this possible!
@OhioStatePIIO@OSUCCC_James
https://t.co/tvZW3TynF9
Thrilled to share our new work out today in @SciImmunology!🥳 @sanidad_kz
We show that neonatal gut bacteria make serotonin to promote gut regulatory T cells and immune tolerance against gut bacteria & food antigens.
https://t.co/dsb9pW80J1
@WeillCornell@WCMpeds@CornellCFI
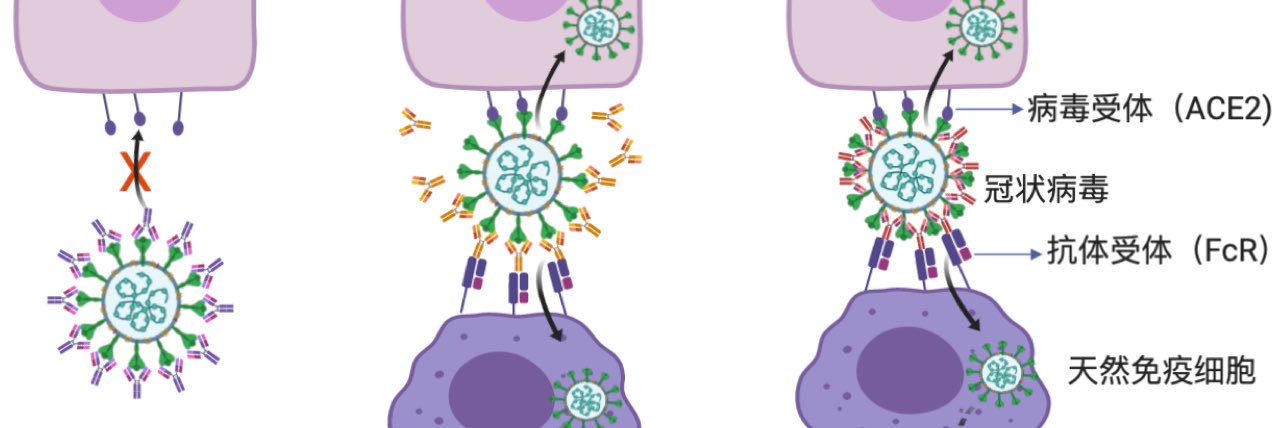
Current i.m. COVID and Flu vaccines induce good immunity in the blood, but not well in the mucosa. Our new study @ImmunologyTang@arka_sc uncovers how mucosal boosters drive powerful IgA responses, essential to block infection at the site of entry.
https://t.co/4UvxQbR7GO