🧬Does this change the overall safety assessment of AAV gene therapy? After treating over 6,000 patients with AAV gene therapy without evidence of major long-term toxic effects, now the first published case of human oncogenesis linked to AAV integration has been documented: A 5-year-old boy with severe mucopolysaccharidosis type I (MPS I, Hurler syndrome) developed a neuroepithelial tumor four years after intracisternal magna administration of AAV9 gene therapy.
🔬 The molecular detective work is fascinating:
Clonal integration of rearranged AAV vector elements into the PLAG1 gene, creating a chimeric AAV-PLAG1 transcript that drove tumor development. The integrated AAV DNA included duplicated enhancer-promoter sequences that upregulated PLAG1 expression 298-fold compared to other CNS tumors
✅ The tumor was successfully resected, and the patient maintains advanced cognitive function.
⚖️ Does this change the overall safety assessment?
Not fundamentally, but it sharpens our focus. While AAV vectors predominantly persist as episomal concatemers, rare genomic integration has been known from neonatal murine models and liver biopsies in gene therapy patients.
👉 This case should translate into more stringent pharmacovigilance, with systematic long-term follow-up and tumor surveillance embedded into all AAV-based gene therapy programs.
🎯 Context is everything:
The risk-benefit calculation varies dramatically by disease, vector design, dose, and delivery route. This case involved:
- High vector concentrations (intracisternal magna delivery)
- Ubiquitous promoter elements (necessary for lysosomal storage disease)
- Possible host factors (prior HSCT)
For conditions like haemophilia treated with lower systemic administration and liver-specific promoters, the profile differs markedly from CNS-directed therapy for MPS I, which requires ubiquitous promoters and high CNS transduction.
#genetherapy #haemophilia @NEJM Rebecca Ahrens-Nicklas @DrSamelsonJones@LindseyAGeorge
https://t.co/zk1gq1ESkZ
🧬 AAV Gene Therapy: Manufacturing DNA in Patient Livers—A Critical Safety Signal 🚨 A groundbreaking @NaturePortfolio Portfolio Medicine case study by Sarah Buddle, and co-authors reveals an alarming discovery in a 7-year-old girl with SMA type 1 who developed severe hepatitis after onasemnogene abeparvovec (Zolgensma®).
The Case
💉 Dose: 2.2×10¹⁵ vg
🔴 Outcome: Severe hepatitis within 7 weeks requiring 19 months steroids + 7 months tacrolimus
💔 While hepatotoxicity affects ~31% of Zolgensma recipients, this case suggests atypical immune drivers requiring prolonged dual immunosuppression.
🔍The Novel Finding
🔬 Metagenomic sequencing and in situ hybridization detected manufacturing plasmid DNA in 5-6% of hepatocytes—approximately 10-fold higher than controls . This is the first direct evidence of persistent bacterial plasmid backbone sequences in human liver following systemic AAV treatment.
⚗️ An possible explanation: Triple-plasmid AAV manufacturing creates residual DNA contamination (bacterial origins of replication, antibiotic resistance genes) that current GMP purification may not fully eliminate.
Limitation of the study
⚠️ Single case—requires validation in larger cohorts
❓ Unknown: manufacturing contamination vs. in vivo amplification
❓ Unknown: whether plasmids directly caused hepatitis or acted as co-factors
🧪 Original vector batch unavailable for comparison
🎯Key Takeaway
This case reinforces urgent need for enhanced manufacturing oversight, real-world pharmacovigilance, and comprehensive liver tissue studies to characterize vector fate in AAV-treated patients.
#onasemnogene #Zolgensma #SMA
Open access:
https://t.co/UqLV2xL7Zc
🛌 Sleep < 7 hours shortens life expectancy almost as much as physical inactivity. New US county-level data (2019–2025) show that, among common health behaviors, only smoking and obesity have stronger negative associations with life expectancy.
❌ What it did not measure: Specific causes of death (cardiovascular, cancer, infections, etc.) or underlying pathophysiological mechanisms
🩸Hypothesis: Sleep deprivation creates a prothrombotic state through inflammation, endothelial damage, platelet hyperactivation, and altered coagulation factor expression and may lead to an increased cardiovascular and mortality risk.
Congratulations to Andrew Mc Hill and co-authors. @SleepResearch_ #sleep
link: https://t.co/iZb1Eb5nXj
📊 Excellent 4-Year Data of Etranacogene Dezaparvovec in Haemophilia B: The Subgroup (N=33) With No Neutralizing Anti-AAV Antibodies (NAb-Negative):
✅ 100% expressed endogenous FIX at therapeutic levels (mean 39.0 IU/dL)
✅ 100% remained prophylaxis-free over 4 years—zero returned to prophylaxis
✅ 99% decrease of exogenous FIX consumption
✅ 85% reduction in bleeds (all, spontaneous, joint)
✅ Safety: Treatment-related AEs only first 3 months; transient ALT elevations 18%, all manageable
This enables direct comparison to other haemophilia B gene therapies where only NAb-negative patients were enrolled.
🔬 🚀 HOPE-B's Inclusive Design:
HOPE-B is the first—and currently only—haemophilia gene therapy trial to include patients with pre-existing AAV neutralizing antibodies for treatment with etranacogene dezaparvovec. Very recently, the NEJM paper presented 5-year data of the full cohort (NAb-negative and NAb-positive; N=54).
Congratulations to Priyanka Raheja and co-authors! @RPTHjournal #haemophilia #genetherapy
https://t.co/Wd57VWSAuj
🩸 First reports of inhibitors to FVIII in PTPs treated with Efanesoctocog Alfa. Important real-world data from Japan by Katsuyuki Fukutake and co-authors: Three previously treated patients (PTPs) with haemophilia A developed de novo inhibitors after switching to Efanesoctocog Alfa (Altuviiio):
🔹 Patient 1: Mild HA (50s) → Inhibitor 3.0 BU at day 14
History of HCC; switched to Efanesoctocog Alfa during radiochemotherapy
🔹 Patient 2: Moderate HA (50s) → Inhibitor 7.0 BU at day 62
Developed massive bleeding and autoimmune hemolytic anemia (AIHA) shortly after switching to emicizumab and rFVIIa
🔹 Patient 3: Severe HA (70s) → Inhibitor 9.0 BU at day 146
Post-surgical switch (ulnar nerve transposition); inhibitor detected after painful swelling/bleeding.
✅ All inhibitor patients were successfully treated by switching to emicizumab prophylaxis and inhibitors disappeared without ITI at 10, 2, and 5 months respectively.
⚠️ Context Matters: Two patients had non-severe disease (limited risk data). Complex clinical scenarios—recent surgeries, malignancy treatment, high-intensity FVIII exposure during cancer therapy—likely influenced individual risk profiles and may have promoted inhibitor development.
🔍 While PTP inhibitor development is considered rare (~2/1000 patient-years) and Efanesoctocog Alfa showed a clean inhibitor profile in Phase III (XTEND-1), this real-world snapshot of a small patient cohort suggests an inhibitor incidence in PTPs of ~7.9% (3/38 EA-treated patients) across three Japanese centers. This emerging signal highlights the need for close laboratory and clinical monitoring when switching products in immunologically challenged patients and reinforces the critical role of robust post-marketing surveillance systems.
#Haemophilia #Inhibitors #EfanesoctocogAlfa #Altuviiio @haemophilia_jnl
https://t.co/P8TnPl7Bab
iTTP and Pregnancy: Moving from "Contraindication" to "Careful Planning"
Is a history of immune-mediated TTP (iTTP) an absolute contraindication for pregnancy? The answer from #ASH25 is a resounding no—but it requires precision medicine and a team approach.
In the second part of his excellent education session, Dr. Senthil Sukumar (Baylor College of Medicine) tackled the complex landscape of pregnancy during remission.
Here are the critical clinical pearls for managing our patients who wish to conceive:
👶 The Risks are Real but Manageable
We cannot sugarcoat the data. Complication rates remain high:
Preeclampsia: ~28%
Clinical Relapse: ~25%
Miscarriage: ~18%
🤰 The "Pre-Conception" Window is Vital
Success starts months before conception. Dr. Sukumar’s expert opinion suggests:
Check ADAMTS13 6–12 months prior to planned conception.
Target: If ADAMTS13 is <20%, consider preemptive rituximab and defer pregnancy for 6–12 months to ensure a safe baseline.
🏥 During Pregnancy: A Tiered Strategy
Management shouldn't be static. The presented algorithm (adapted from Ferrari et al. and Brown et al.) proposes adapting therapy based on ADAMTS13 levels:
>20-25%: Close monitoring (CBC & ADAMTS13 every 3-4 weeks).
10-20%: Consider low-dose steroids.
<10%: Consider plasma exchange to prevent overt relapse.
Prophylaxis: Low-dose aspirin after 12 weeks is recommended (per USPSTF guidelines for high-risk preeclampsia).
The takeaway? With a multidisciplinary team (Hematology + Maternal-Fetal Medicine) and enhanced monitoring, we can support our iTTP patients in building their families safely.
#ASH25 #Hematology #iTTP #WomensHealth #PregnancyInMedicine #HighRiskOB #ADAMTS13 #PatientCare
🚨 iTTP remission ≠ cure. The vascular injury persists. TTP as a cardiovascular disease equivalent. Just finished Dr. @senthilsukumar 's excellent #ASH25 session on long-term iTTP management. This completely changed how I think about these patients.
The Numbers Hit Different:
🫀 28.6% of survivors → major cardiovascular events
🧠 50% → silent cerebral infarcts (vs 16.6% controls)
💔 Cardiovascular complications 10–20 years EARLIER
😰 80% depression | 35% post traumatic stress disorder
📉 >60% measurable neurocognitive impairment
🪤 71% moderate-severe headaches
💼 20% can't work due to complications
The Game Changer: Endothelial Damage That Doesn't Heal
Patients are not "fine" after remission. The endothelium stays injured. Stress cardiac MRI shows reduced perfusion + impaired coronary vasodilation—the heart can't increase blood flow under stress even when ADAMTS13 normalizes.
The Actionable Part ���
ADAMTS13 ≤70% = 27.6% stroke rate
ADAMTS13 >70% = ZERO ischemic strokes
As a consequence, treat iTTP as CVD Equivalent
✅ Comprehensive cardiovascular risk factor optimization (lipids, A1C, smoking, BP, weight, activity)
✅ Baseline mood + neurocognitive screening for ALL survivors
✅ Neuropsych testing every 1–2 years
✅ Multidisciplinary teams (neuro, psych, cardio)
#TTP
🧬⚡For the first time ever, the progression of Huntington's Disease can be significantly slowed. UniQure announced on September 23, 2025 excellent results from their pivotal Phase I/II study of AMT-130.
🧠 What is Huntington's Disease?
Huntington's disease is a rare, inherited neurological disorder caused by a mutation in the huntingtin gene, leading to progressive breakdown of brain cells, particularly in the striatum. This results in motor dysfunction, cognitive decline, and psychiatric disturbances, typically proving fatal within 10-30 years of symptom onset. Currently, no FDA-approved treatments exist to slow disease progression.
👥 The AMT-130 Study Population
This pivotal trial enrolled 29 patients with early-stage Huntington's disease, with 17 receiving high-dose treatment and 12 receiving low-dose AMT-130. At the 36-month analysis, 12 patients per dose group had complete follow-up data.
High-dose treatment: 6 × 10¹³ vector genomes (60 trillion vector genomes)
Low-dose AMT-130: 6 × 10¹² vector genomes (6 trillion vector genomes)
🔬 The Vector Technology 🔬
AMT-130 utilizes an AAV5 (Adeno-Associated Virus 5) vector (similar to the vector technology used in approved gene therapy products for haemophilia A and haemophilia B) carrying an engineered microRNA (miHTT) that specifically targets huntingtin mRNA.
This one-time gene therapy is delivered directly into the brain's striatum (caudate and putamen) through MRI-guided stereotactic neurosurgery. The microRNA enters cells, gets processed by natural cellular machinery, and ultimately reduces production of both mutant and normal huntingtin protein by targeting the mRNA before translation.
📊 Remarkable Efficacy Results 📊
The high-dose AMT-130 demonstrated statistically significant 75% disease slowing at 36 months as measured by the composite Unified Huntington's Disease Rating Scale (cUHDRS) compared to propensity score-matched external controls.
Reduced neurodegeneration biomarkers: CSF neurofilament light protein levels were 8.2% below baseline at 36 months, despite expected increases over three years
✅Safety Profile
AMT-130 demonstrated a manageable safety profile with no new drug-related serious adverse events reported since December 2022. The most common adverse events were related to the surgical procedure itself, all of which resolved.
Congratulations to Prof Sarah Tabrizi of the University College London, the co-authors and uniQure. #Huntington's Disease #genetherapy
🧬 The Bi8 Study demonstrates a novel single-chain FVIII-mimetic antibody gene therapy approach that could enhance treatment options for haemophilia A. The AAV8-Bi8 system delivers the genetic blueprint (DNA sequence) for the Bi8 antibody directly to hepatocytes through. Hepatocytes are naturally equipped with sophisticated protein synthesis and secretion machinery that makes antibody production entirely feasible.
🔬 What Makes Bi8 Special?
- Compact Design, Maximum Impact: Unlike traditional approaches that struggle with oversized FVIII genes, Bi8 is elegantly designed as a compact 54.5 kDa single-chain antibody that fits comfortably within AAV8 vectors using just a 4.4 kb expression cassette. This solves the major packaging challenge that has limited previous gene therapies.
- Dose-dependent, durable expression across three dose levels (4×10¹¹, 4×10¹², and 1.2×10¹³ vg/kg)
- Peak plasma concentrations of 4.5, 47.4, and 178.8 nM respectively at 2 weeks post-infusion
- Complete phenotypic correction of bleeding - even at the lowest dose, blood loss was reduced from 760.4 μL to 401.2 μL
🎯 Key Advantages Over Current Approaches
- Excellent Safety Profile: The 12-week study showed no toxicity or anti-drug antibody responses in any treated animals. Transgenic expression remained stable throughout the study period with no immunogenicity concerns.
- Enhanced Durability Potential: While current FVIII gene therapies like Roctavian show declining expression over time, Bi8's antibody-based approach within optimal AAV packaging constraints may offer more stable long-term expression patterns.
- Broader Patient Applicability: The approach could potentially benefit patients with FVIII inhibitors, expanding treatment options beyond current gene therapies.
🚀 Looking Forward
The study demonstrates that haemostasis was secured across all dose groups, including complete bleeding correction at clinically relevant doses.
AAV8-Bi8 has the potential to offer sustained, life-long haemostatic control, including in patients who have developed inhibitors to FVIII.
★ However, do we still need gene therapy on FVIII mimetics when the first oral FVIII mimetic is in clinical development?
Congratulations to @amitnathwani and co-authors of the University College London. #genetherapy #haemophilia
https://t.co/ZtI0wQKPln
🩸 Promising results in new subcutaneous von Willebrand disease treatment presented at BIC 2025! @carolynmiller presented Phase I results for VGA039:
This monoclonal antibody targets Protein S to restore balance in blood clotting by inhibiting both tissue factor pathway inhibitor α (TFPIα) and activated protein C (aPC), enhancing thrombin generation during both initiation and propagation phases of coagulation.
The VIVID 2 study enrolled 10 VWD patients (ages 21-52) with diverse VWD subtypes, including those with mild hemophilia A. Results showed increased thrombin generation lasting 4+ weeks without dose-limiting toxicities:
✅ Safe and well-tolerated across all VWD types (1, 2A, 2M, 2N, 3)
✅ Single subcutaneous injection maintained therapeutic concentrations for ~4 weeks
✅ Significant bleed reduction: 75-88% reduction in annualized bleeding rates in high-bleed patients
✅ Universal approach: Works across all VWD types by targeting Protein S
Unlike current VWD treatments requiring multiple weekly IV infusions, VGA039 may offer convenient subcutaneous dosing with sustained multi-week protection.
#vonWillebranddisease #StarTherapeutics #VegaTherapeutics #BIC2025
🚨 Gene therapy of haemophilia A in patients with current or recent inhibitors to FVIII. Exciting Phase 1/2 results from GENEr8-INH presented by Konstantia Maria Chavele at the 13th BIC International Conference demonstrate valoctocogene roxaparvovec's potential in haemophilia A patients with inhibitor history – historically our most challenging population to treat.
📊 Current Enrollment & Safety Profile
Part A (active inhibitors): 3 participants
Part B (prior inhibitors): 7 participants
⚠️ Safety Overview
📈 ALT elevations dominant safety signal: 90% (9/10 participants)
💊 Corticosteroid management required: 80% (8/10)
🛡️ Prophylactic corticosteroids: 40% (4/10)
🎉 Zero inhibitor recurrence across both cohorts
✅ No thromboembolic events or malignancies reported
🎯 Prior Inhibitor Population (n=7)
✅ 🩸 Zero bleeds after prophylaxis cessation – no treated bleeds, no FVIII infusions required
✅ 📊 Sustained therapeutic FVIII levels: Week 26: 50.1 IU/dL (SD 43.8) → Week 52: 25.8 IU/dL (SD 18.2)
✅ ⚗️ Chromogenic assay kinetics consistent with GENEr8-1 results
✅ 🆓 100% freedom from prophylaxis throughout follow-up
✅ 🛡️ No inhibitor recurrence
🔬 Active Inhibitor Cohort (n=3)
📈 All 3 participants showed increased FVIII inhibitor titers post-infusion
⭐ One participant achieved detectable FVIII activity despite initial inhibitor rise
🧠 Immune tolerance evidence: Inhibitor became undetectable in responder, suggesting FVIII production overcame inhibitory response
#GeneTherapy #Haemophilia #Inhibitors
@BioMarin #Roctavian #BIC2025
🚨 First reported inhibitor development in haemophilia A gene therapy 🧬Presented by Davide Matino at Hashtag#BICmeeting at Phase 3 giroctocogene fitelparvovec (AAV6, 3×10¹³ vg/kg, n=74).
Patient Profile:
🧬 Genetic: Intron 22 inversion
🩸 History: ITP + splenectomy
🦠 Comorbidities: HCV & HIV co-infection
📅 Experience: 6,000 exposure days with FVIII
Clinical Timeline:
📈 Peak FVIII (day 75 after gene therapy): 441.7%
⚠️ Post-infusion: Multiple steroid courses for ↑ALT/AST
🔴 Inhibitor development more than 1 year after treatment
#BIC2025, #haemophilia, #genetherapy, #inhibitor
🧬 Updated Ph3 data on gene therapy for haemophilia A with giroctocogene fitelparvovec (AAV6, 3e13 vg/kg in 74 participants), presented by Davide Matino at BIC meeting 2025:
🌟 ~35% of participants maintained near-normal to normal FVIII activity (40–150%) at 2 years post-infusion
🔄 Durability data is impressive: sustained efficacy approaches three years of follow-up, demonstrating the transformative potential of this AAV6 approach
📈 Slow decline pattern:
- Year 1 mean: 51.7%
- Year 2 mean: 51.9% (stabilization)
- Year 3 mean: 40.7% (median: 38.0%)
Note: Only 8 participants had 3-year follow-up
✅ Sustained FVIII levels >5% in >80% of participants at 15 and at 24 months
✅ 98.3% reduction in treated bleeding episodes (4.08 → 0.07 ABR post-infusion)
🔹 Transient FVIII activity >150% in nearly 50%, managed with low-dose prophylactic DOAC in 30%
- ⚠️ One participant developed a thrombotic event (history of thrombosis & risk factors)
🔁 2 participants resumed FVIII prophylaxis
✅ Generally well-tolerated safety profile with manageable ALT elevations (ALT ↑ in 61%)
🔥 High rate of infusion-related reactions (75%), but no discontinuation of study drug administration
🦠 One case of new cancer at 35 months (oral squamous cell carcinoma, not related to study drug); in total 2 malignancies reported
🛡️ One case of FVIII inhibitor development (more to follow)
❌ Despite these results, Pfizer has discontinued this program and terminated their collaboration with Sangamo Therapeutics in December 2024
#BICmeeting #genetherapy #haemophilia #bic2025
New study on AAV5 antibodies in haemophilia B gene therapy ��. We just published in Molecular Therapy – Methods & Clinical Development on how AAV5 antibodies behave over time in adults with haemophilia B.
This analysis is based on the HOPE-B phase 3 trial with 67 patients in the US and Europe.
Importantly, for etranocogene dezaparvovec, AAV5 NAb positivity is not a strict contraindication. But very high titers may reduce transduction efficiency. That’s why NAb screening is an essential part of assessing eligibility for commercial gene therapy.
Key findings:
1️⃣ 48% of patients had neutralizing antibodies (NAbs) at screening (median titer 58; range 9–3440)
2️⃣ Levels remained stable over 8 months (📈 median variation 25%; range 2–154%)
3️⃣ Strong correlation between NAbs and IgG (r=0.96)
4️⃣ Fewer than 5% switched from negative to positive 🔄
5️⃣ ~10% seroreverted from positive to negative
🎂 NAb positivity was more frequent in patients ≥50 years (p=0.0065)
⏰ Why this matters?
NAb test results were consistent over months. Screening can be done up to 8 months before gene therapy infusion, giving more flexibility for clinical planning.
🙏 Thanks to Robert Klamroth, @SandraLeQuellec and Jacqueline Tarrant for leading this work, and to @CSL for supporting the study.
#Hemophilia #GeneTherapy #AAV5
https://t.co/1Rh65NIgGE
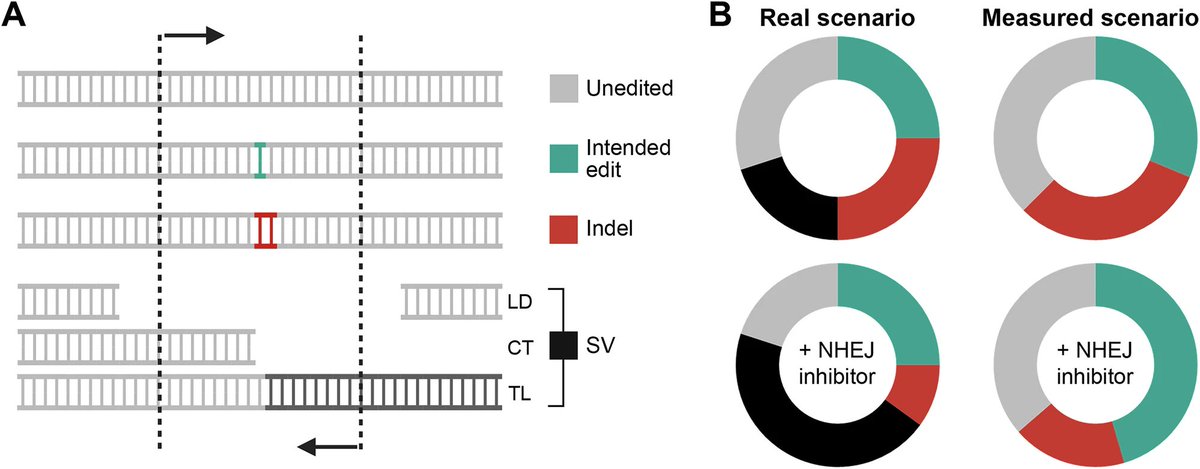
🚨 CRISPR's hidden danger: New Nature Communication from genome editing safety experts Toni Cathomen, Carla Fuster García and Clotilde Aussel reveals concerns about "precision" enhancers!
⚠️ It's beyond off-target effects and possibly a worse problem: The field has been focused on off-target effects (off-target sites prediction, and off-target activity measurement)- where CRISPR cuts at unintended sites with similar sequences to the target.
But this paper reveals something different: structural variations (SVs) including massive chromosomal chaos that happens even at the intended target site.
DNA-PKcs inhibitors like AZD7648 - compounds used to make CRISPR more precise by promoting homology-directed repair (HDR) over error-prone repair - cause a 1000-fold increase in chromosomal translocations.
💣 The catastrophic outcomes:
· ⚡ Megabase-scale deletions spanning millions of DNA bases
· 🧬 47.8% of cells losing entire chromosome arms
· 📈 Kilobase-scale deletions increased up to 35-fold
· 🔀 Chromosomal translocations between different chromosomes
· 💀 Chromothripsis - catastrophic chromosome shattering
🏥 Clinical reality check:
Casgevy - the first approved CRISPR therapy - targets BCL11A for sickle cell disease. BCL11A editing frequently causes large kilobase-scale deletions in stem cells. 8% of African ancestry patients carry variants creating additional off-target sites.
⚠️ Repair pathway problems:
In human cells, there are two main DNA repair pathways after CRISPR cuts:
· NHEJ (Non-Homologous End Joining) ⏩ fast but error-prone
· HDR (Homology-Directed Repair) 🔬 precise but inefficient
By inhibiting DNA-PKcs to boost HDR, researchers accidentally created genomic chaos.
🙈Detection crisis:
Standard sequencing completely misses these changes because large deletions remove PCR primer sites, making them "invisible" and leading to massive overestimation of success rates.
💡Solutions from the authors:
The authors discuss better detection methods (CAST-Seq, long-read sequencing), safer enhancement approaches(53BP1 inhibition), alternative strategies (base editors), and rethinking necessity of ultra-high efficiency.
Their conclusion: We need "holistic, treatment-centered evaluation of both off-target and aberrant on-target effects to ensure therapeutic efficacy is not achieved at the expense of unintended consequences".
open access link: https://t.co/6UO2W0bhz4
@NatureComms #geneediting
📰 Check the recently published @haemophilia_jnl
article on Qualification Criteria of Gene Therapy for Haemophilia - Opinion of the EAHAD Gene Therapy Working Group. Read the full article 👉 https://t.co/FFjC3SIVtj