Groundbreaking CREST-2 Results: CAS Role in Asymptomatic Carotid Stenosis Evolving!
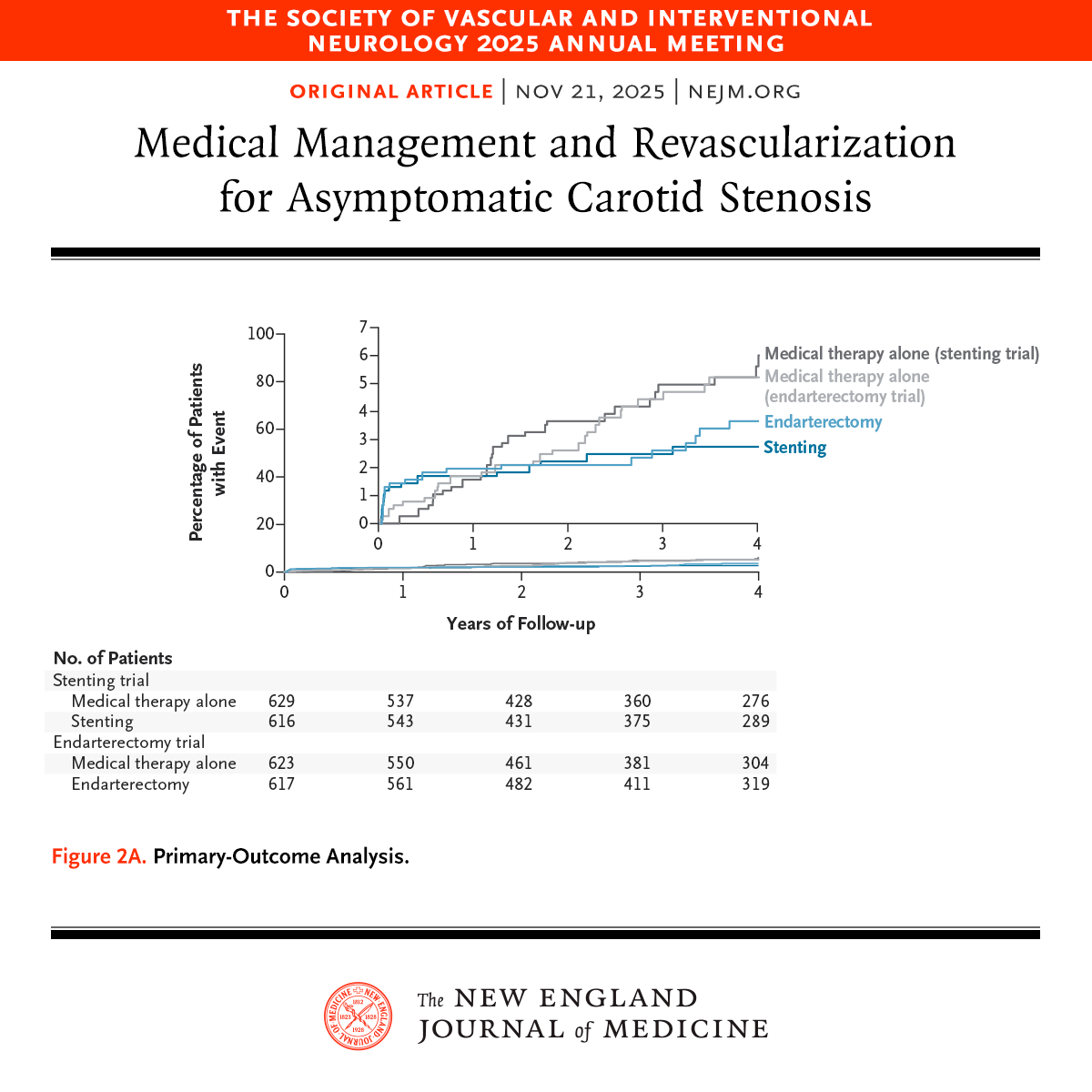
Thrilled by today's NEJM publication of CREST-2—two RCTs with 2,485 patients showing intensive medical management (IMM) alone yields excellent outcomes, but revascularization adds targeted value.
In the stenting arm (n=1,245), IMM + TCAS cut 4-year primary events (stroke/MI/periprocedural death) to 2.8% vs. 6.0% with IMM alone (HR 0.45; P=0.02)—a clear win for TCAS!
The endarterectomy arm (n=1,240) was closer: 3.7% vs. 5.3% (HR 0.70; P=0.24), no significant edge for CEA, highlighting periprocedural risks.
Paradigm shift: Prioritize TCAS + IMM for high-risk cases to slash strokes—modern meds are powerful, but selective intervention saves lives! Why the uptick in events for CEA between 3-4 years? Thoughts on guideline updates? #CREST2 #StrokePrevention #CarotidStenting #CAS #EmbolicProtection #CAS
Presented at #SVIN25:
CREST-2: In high-grade asymptomatic carotid stenosis, addition of stenting to medical therapy led to a lower risk of stroke over a 4-year period. Endarterectomy did not lead to a significant benefit. Full results: https://t.co/ojge1CjqiU
Editorial: Managing Asymptomatic Carotid Stenosis https://t.co/D9LH89Edyk
@svinsociety
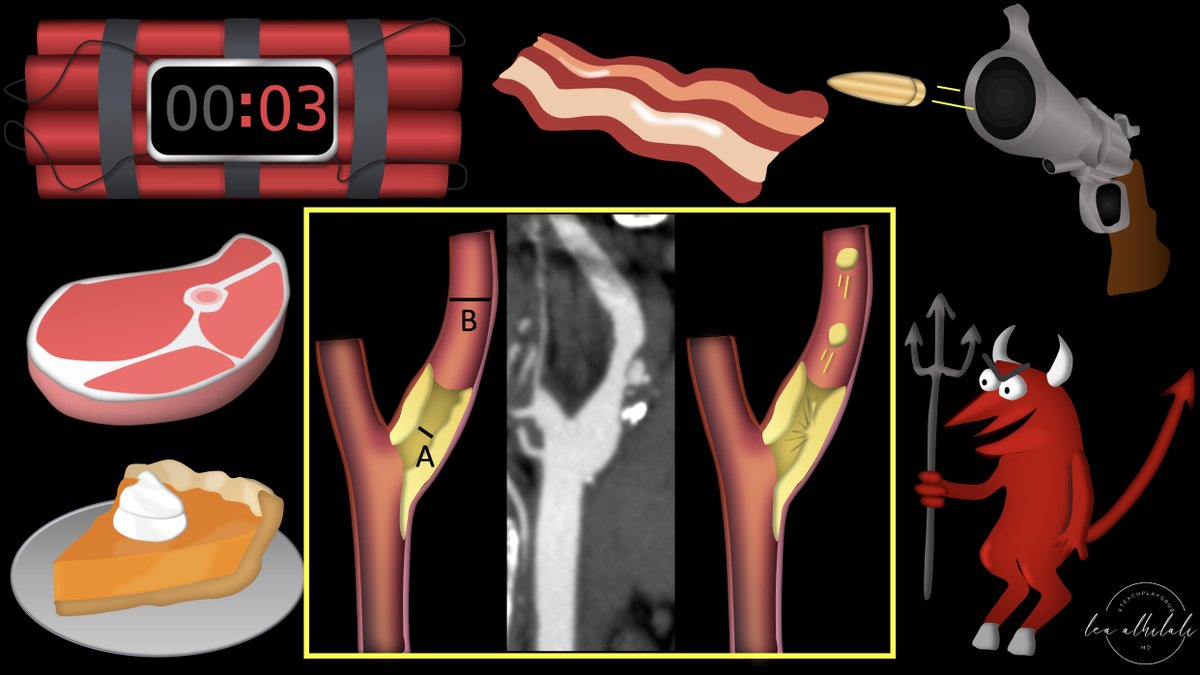
1/The 90s called & wants its carotid imaging back!
It’s been 30 years--why are you still just quoting NASCET?
Do you feel vulnerable when it comes to identifying plaque vulnerability?
Here’s a thread to help you identify high risk plaques with carotid plaque imaging
@Darcy_ID_doc There is alphavac now that doesn’t require VV ECMO. Regardless if the PFO is that big a concern, the aortic arch vessels can be protected with a filter, although the likelihood of embo is rare bc the VV ECMO filters the veg out before returning the blood. Hope it held
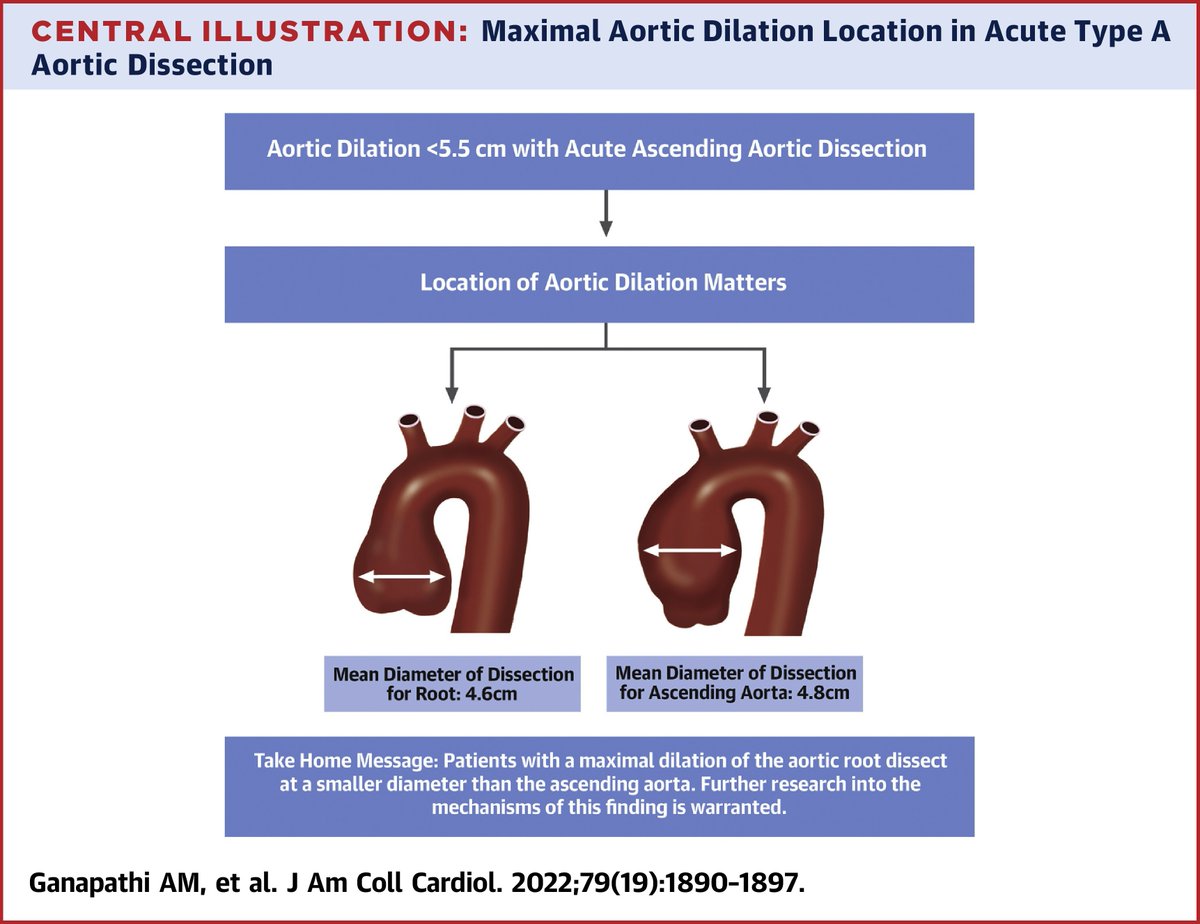
Does dissection occur at different diameters based on aortic location? See more on this important question on type A aortic dissection in #JACC: https://t.co/4OUgrC96Jo
#CardioTwitter@MarkELindsay@keaglemd
@AvrahamCooperMD@KinturSanghvi Can be retrieved with lasso technique w endovascular approach. Always a god reminder for RHC to assess fluid status before venous stents, having fluids on and ultilizing ivus.
“The primary utility of IVUS appears to be accurate vessel sizing with the benefit of this being in cases treated with DCB." @Flinders@EricSecemskyMD https://t.co/k7s8IUKPkh