🚨 Can first-line FOLFIRINOX beat mFOLFOX6 in HER2-negative advanced gastric/GEJ adenocarcinoma?
At #ESMOGI26, the phase III IRIGA trial says: not in the overall population.
🧵 391MO | IRIGA
Patients:
▪️ HER2-negative advanced gastric/GEJ adenocarcinoma
▪️ 1:1 randomization to FOLFIRINOX vs mFOLFOX6
▪️ 318 analyzed (157 vs 161)
Primary endpoint: PFS
Key results
🔹 PFS: 7.2 vs 6.8 mo
HR 0.82 (95% CI 0.64–1.05)
🔹 OS: 13.4 vs 13.2 mo
HR 0.86 (95% CI 0.64–1.14)
🔹 ORR: higher with FOLFIRINOX
But the cost?
⚠️ More toxicity with FOLFIRINOX
Higher nausea, vomiting, diarrhea, asthenia
More G-CSF prophylaxis needed
Interesting signal
Benefit appeared more likely in selected patients:
▪️ No peritoneal metastases
▪️ Retroperitoneal/supraclavicular nodal disease
▪️ Patients able to undergo conversion surgery
Take-home
For unselected HER2-negative advanced gastric/GEJ cancer, mFOLFOX6 remains a very reasonable standard.
FOLFIRINOX may be worth reserving for carefully chosen oligometastatic / conversion-intent patients, but this is not a practice-changing win for triplet therapy.
Would you still use upfront FOLFIRINOX in any subgroup?
#GastricCancer #GastroesophagealCancer @myesmo@oncoalert
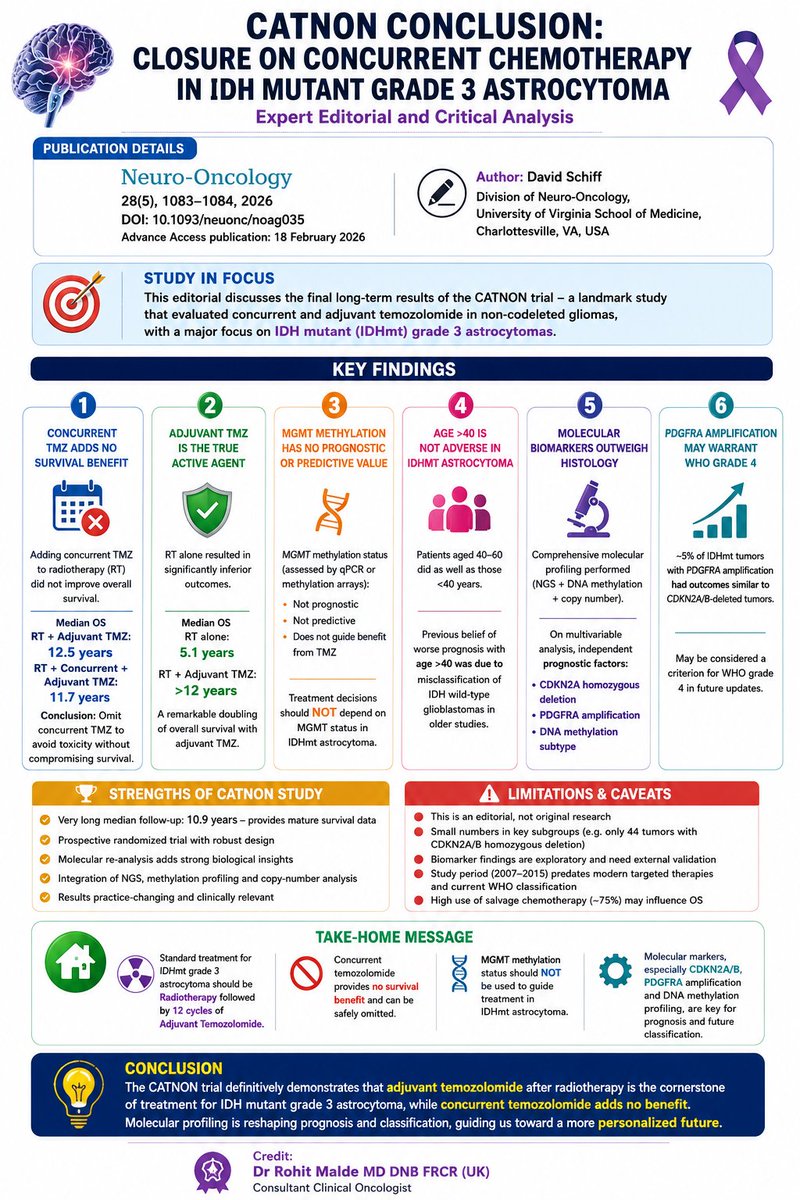
CATNON trial lessons
Concurrent temozolomide provides no survival benefit in IDHmutant Gr3 astrocytoma
Adj Temozol (12#) is the component that improves survival
Modern molecular biomarkers (esp CDKN2A/B, PDGFRA amp & DNA methylation profiling) are stronger prognostic markers
#ESMOGI2026
Surprising news for mCRC out of ESMOGI.
KRYSTAL-10: Adagrasib + cetuximab misses its primary endpoint in 2L KRAS G12C mCRC.
After the accelerated approval and encouraging activity from KRYSTAL-1, many expected dual KRAS/EGFR inhibition to outperform chemotherapy in the second line. That didn't happen.
Quick hits:
• Primary endpoint (PFS): Negative
• mPFS 7.5 vs 8.1 months
• HR 0.89 (95% CI 0.71-1.13)
• Response rate dramatically improved
• ORR 47% vs 16%
• CR 7% vs <1%
• No improvement in OS at the final analysis despite the higher response rate.
So what happened?
This is a reminder that response rate ≠ durable disease control. Nearly half of patients responded, but those responses did not translate into longer PFS or OS compared with modern chemotherapy. Targeted therapy works, but mCRC can overcome via resistance mechanisms (such as via massive KRAS upregulation). Will be interesting to see how novel degraders come into the mix here... Remember, this is a first gen KRASi, the future is still bright here.
What does this mean for clinic tomorrow? Honestly, I still love a chemo-free option that is at least on par with chemotherapy.
This isn't the end of KRAS G12C in CRC. Far from it.
The focus now shifts to moving targeted therapy earlier, where combinations with chemotherapy may produce deeper, more durable responses before resistant clones emerge. Multiple frontline studies are already underway.
@TheGutOncLab@OncoAlert@Onco_Nexus@myESMO
🚨 COMPETE may change sequencing in advanced GEP NETs.
First phase 3 head-to-head:
☢️ ¹⁷⁷Lu-edotreotide PRRT
vs
💊 Everolimus
Population:
Advanced, progressive, SSTR+ G1-2 GEP NETs
N=309 | 58% pancreatic | 85% second-line
Key results 👇
✅ PFS
23.9 vs 14.1 mo
HR 0.67, p=0.022
✅ ORR
22% vs 4%
p<0.0001
✅ QoL
Decline with everolimus, preserved with PRRT
✅ Safety
TR grade 3-4 AEs:
18% vs 40%
OS immature:
63.4 vs 58.7 mo
HR 0.78, p=0.21
Take-home:
For progressive SSTR+ G1-2 GEP NETs, PRRT moves ahead of everolimus for disease control, response, QoL and tolerability.
This is not just “another PRRT trial.”
It is sequencing evidence.
Full paper in first comment.
🚨 Liquid biopsy may be the key to anti-EGFR rechallenge in chemorefractory mCRC. 🩸
At #ESMOGI26, the phase II PARERE trial suggests that in RAS/BRAF WT, ctDNA-selected patients, panitumumab may outperform regorafenib after prior anti-EGFR benefit. 👀
#PARERE trial
Liquid biopsy-guided anti-EGFR re-treatment in chemorefractory RAS/BRAF WT mCRC
Who were included?
▪️ RAS/BRAF WT mCRC
▪️ Prior benefit from 1L anti-EGFR-based therapy
▪️ ≥1 anti-EGFR-free line before rechallenge
▪️ ctDNA tested for RAS/BRAF V600E resistance alterations 🧬
Study design
🔹 Arm A: Panitumumab → regorafenib at progression
🔸 Arm B: Regorafenib → panitumumab at progression
Key findings in ctDNA-WT patients (n=213)
✅ Panitumumab-first performed better than regorafenib-first
📈 ORR1: 16% vs 2%
📈 ORR2: 17% vs 0%
📊 DCR1: 59% vs 32%
📊 DCR2: 56% vs 37%
⏳ PFS1: 4.1 vs 2.4 mo
⏳ PFS2: 3.9 vs 2.7 mo, p=0.03
Who seemed to benefit most?
🎯 Patients with a longer anti-EGFR-free interval
▪️ ctDNA-WT patients had a longer interval since last anti-EGFR: 14.3 vs 11.2 months
▪️ >6 months since prior anti-EGFR was associated with greater benefit from panitumumab
Important nuance ⚠️
About 9% of ctDNA-WT patients still harbored other putative anti-EGFR resistance mutations, and in that subgroup the benefit signal was lost.
Take-home 💡
This is an important proof-of-concept for ctDNA-guided hyperselection in anti-EGFR rechallenge.
For chemorefractory RAS/BRAF WT mCRC, the message is becoming clearer:
👉 Don’t rechallenge blindly. Rechallenge by liquid biopsy.
@myesmo@OncoAlert #mCRC #ColorectalCancer #LiquidBiopsy
Continue Anti-EGFR or Switch to Anti-VEGF?
Key takeaways from the ESMO GI 2026 IPD Meta-analysis:
• Included 405 patients from 5 randomized trials with RAS/BRAF wild-type, MSS/pMMR metastatic colorectal cancer.
• Continuing anti-EGFR with a new chemotherapy backbone was associated with longer overall survival than switching to anti-VEGF.
➜ 25.8 vs 16.9 months (HR 0.60)
• Progression-free survival and objective response rate were similar between the two strategies in the overall population.
• Patients with an anti-EGFR-free interval ≥4 months had:
✓ Better PFS (11.0 vs 8.8 months)
✓ Higher response rate (53% vs 40%)
Bottom line: Anti-EGFR retreatment may be a reasonable option for carefully selected patients after first-line progression, but prospective ctDNA-guided validation is needed before changing standard practice.
Reference: ESMO GI 2026 | Abstract 4RO | Individual Patient Data Meta-analysis of 5 Randomized Trials.
EMERALD-1 Final OS Analysis
Durvalumab ± Bevacizumab + TACE in Unresectable Embolization-Eligible HCC (eeHCC)
Key findings
• Previous EMERALD-1 showed a significant PFS benefit.
• Final analysis showed no overall survival benefit with the addition of durvalumab ± bevacizumab to TACE.
• Combination therapy was associated with higher toxicity and treatment discontinuation.
• PFS improvement did not translate into an OS benefit.
Clinical implication
• Improved disease control alone should not be assumed to improve survival in eeHCC.
• Treatment decisions should balance PFS benefit against toxicity, treatment burden, and cost.
Reference
Sangro B, et al. EMERALD-1 Final Overall Survival Analysis. ESMO GI Congress 2026.
#ESMOGI2026 #HCC #LiverCancer #Oncology #MedTwitter #MVOnco
💥 JCOG1008 5-year update is here.
The long-standing debate over weekly vs 3-weekly cisplatin in postoperative head & neck cancer may finally have an answer.
📌 JCOG1008
👥 Postoperative high-risk LA-SCCHN
⚖️ Weekly cisplatin (40 mg/m²) + RT vs 3-weekly cisplatin (100 mg/m²) + RT
Key results (median follow-up: 5.6 years):
✅ 5-year OS
• 71.2% vs 58.7%
• HR 0.76 (95% CI 0.52-1.12)
• Noninferiority confirmed
✅ 5-year RFS
• 64.3% vs 53.0%
• HR 0.81
✅ 5-year Local RFS
• 68.8% vs 57.2%
• HR 0.79
🛡️ No clinically meaningful increase in late toxicity.
⬇️ Acute toxicity remained more favorable with weekly cisplatin.
🎯 Take-home:
Weekly cisplatin is no longer just the “more convenient” option.
It now has mature 5-year randomized data supporting it as a standard postoperative CRT regimen for high-risk LA-SCCHN.
Will this change your practice?
@ASCO@myESMO@oncoalert
#HeadNeckCancer #RadOnc #MedOnc
HER2+ THERAPY IS BECOMING RESPONSE-ADAPTED
A simple algorithm proposed by Tarantino et al. (JCO 2026):
▪️ Stage IIA → THP → Surgery → HP
▪️ Stage IIB → THP → Response assessment → Continue THP or escalate to T-DXd
▪️ Stage III → TCHP or THP → T-DXd → Surgery
▪️ pCR → Complete planned HER2-directed therapy
▪️ Residual disease → T-DXd or T-DM1
The concept is simple:
✓ Stage
✓ Biology
✓ Treatment response
Together determine treatment intensity.
We are moving beyond a one-size-fits-all approach toward more personalized HER2-directed therapy.
Adapted from Tarantino et al., JCO 2026.
#BreastCancer #HER2 #HER2Positive #Oncology #JCO #ASCO #TDXd
HR+/HER2+ metastatic breast cancer now has two positive phase III maintenance strategies after THP induction.
🔹 PATINA Palbociclib + trastuzumab/pertuzumab + endocrine therapy PFS: 44.3 vs 29.1 months HR 0.75
🔸 HER2CLIMB-05 (HR+ subgroup) Tucatinib + trastuzumab/pertuzumab PFS: 25.0 vs 18.1 months HR 0.73
But these trials are not directly comparable.
Important differences: • PATINA enrolled only HR+/HER2+ disease • Endocrine therapy was mandatory in PATINA • HER2CLIMB-05 included all HER2+ disease • Endocrine therapy was optional in HER2CLIMB-05 (~45% received ET) • Tucatinib offers CNS-active HER2 blockade • Palbociclib addresses ER/CDK4/6 resistance
For now, PATINA establishes CDK4/6-based maintenance as the reference standard in HR+/HER2+ disease.
The next question is no longer whether maintenance matters.
The question is: Should we target ER/CDK4/6 resistance, persistent HER2 signaling, or both?
#ASCO2026 #BreastCancer #HER2Positive #HRPositive #MetastaticBreastCancer #PATINA #HER2CLIMB05 #Palbociclib #Tucatinib #CDK46 #Oncology #MedTwitter #BreastOncology #MVOnco
CHEMO-IO VS IO ALONE IN PD-L1 ≥50% NSCLC
• IPD network meta-analysis of 24 phase III trials (n=5,546)
• OS: 29.2 vs 19.8 months (+9.4 months)
• PFS: 11.3 vs 6.8 months (+4.5 months)
• Fewer early progressors with chemo-IO
• Greater toxicity with combination therapy
• Not a head-to-head randomized comparison
PD-L1 ≥50% may not be enough reason to omit chemotherapy.
Di Federico et al. • JAMA Oncology 2026
#NSCLC #LungCancer #Immunotherapy #MVOnco
Practice-Changing ASCO 2026 Updates 🇮🇳
Several ASCO 2026 studies reinforced a common message: improve outcomes by treating earlier, personalizing therapy, and avoiding unnecessary treatment.
🔹 PROTEUS showed that perioperative apalutamide improved pathologic response and reduced future metastatic events in high-risk localized prostate cancer.
🔹 ARACOG highlighted that treatment choices can affect cognition, with darolutamide associated with less cognitive decline than enzalutamide.
🔹 EMERALD-3 moved immunotherapy-based combinations earlier into the management of embolization-eligible HCC.
🔹 ASTRUM-006 demonstrated that biomarker-selected perioperative immunotherapy can improve outcomes in resectable gastric cancer.
🔹 CHRONO reminded us that more treatment is not always better—additional chemotherapy improved surgical outcomes but did not improve DFS.
The key takeaway:
✅ Intensify earlier when it matters
✅ Preserve quality of life
✅ Move immunotherapy earlier
✅ Personalize treatment intensity
✅ Avoid overtreatment
#ASCO2026 #Oncology #CancerResearch #GUOnc #GIOnc #GynOnc #MedTwitter #MVOnco
EARLY-STAGE NSCLC #ASCO2026
Three key lessons:
✅ RET joins EGFR and ALK as a validated adjuvant target (LIBRETTO-432)
✅ Perioperative lorlatinib may convert unresectable ALK+ disease into a surgical disease (LORIN)
❌ Routine adjuvant nivolumab was not supported in EGFR/ALK-negative resected NSCLC (EA5142)
Test every resected NSCLC.
Target the driver.
Avoid overtreatment.
#LungCancer #NSCLC #ThoracicOncology #PrecisionOncology #ASCO2026 #MVOnco
Does PD-L1 ≥50% always mean pembrolizumab alone? 🤔
This retrospective NSCLC study says: not necessarily.
👥 Advanced NSCLC, PD-L1 TPS ≥50%, EGFR/ALK negative
n=206
PC: pembro + chemo
PM: pembro alone
📊 Key results:
PFS: 12.37 vs 9.60 mo
HR 0.44, p<0.001
OS: NR vs 28.91 mo
HR 0.40, p=0.005
ORR: 61.7% vs 46.9%
🧠 My take:
For fit patients with high disease burden, chemo-IO may still be the stronger first-line option, even in PD-L1 high disease.
But this is retrospective. Selection bias matters. Prospective data remain key.
🔖 Save this for clinic discussions.
📖 Full paper in comment ⬇️
#LCSM #OncoTwitter #MedTwitter @OncoAlert@myesmo@esmo_open
CAPTURE Trial #ASCO2026
A targetable mutation does not automatically mean targeted therapy is the best next treatment.
In PIK3CA-mutant HR+/HER2− metastatic breast cancer after CDK4/6 inhibitor progression:
• Alpelisib + fulvestrant: PFS 7.4 months
• Capecitabine: PFS 9.4 months
• Higher ORR and fewer grade 3/4 toxicities with capecitabine
Key ASCO pearl:
PIK3CA-mutant ctDNA ≠ PI3K addiction.
Biomarker positivity does not always mean biomarker dependence.
Geoghegan et al. #ASCO2026
#BreastCancer #MBC #Oncology #MedTwitter #MVOnco
DRIVER-MUTATED ADVANCED NSCLC #ASCO2026
Three landmark trials. One clear message.
🟢 CROWN: 7-year PFS 55% in 1L ALK+ NSCLC
🔵 WU-KONG28: Targeted therapy era begins for EGFR Ex20ins disease
🟢 CHRYSALIS-2: Median OS 41 months in atypical EGFR NSCLC
🧬 Test early
🎯 Treat precisely
🧠 Protect the brain
⏳ Think in years, not months
Driver testing is no longer optional—it helps define the patient's future.
#LungCancer #NSCLC #ThoracicOncology #PrecisionOncology #ASCO2026 #MVOnco
CAR-T may finally be showing signs of breaking through in MSS metastatic colorectal cancer.
In a phase I study of GUCY2C-targeted CAR-T (IM96), heavily pretreated mCRC patients achieved:
🔹 ORR: 26.3% overall
🔹 ORR: 40% at the recommended phase II dose
🔹 mPFS: 7.0 months at RP2D
🔹 Responses seen even in patients with liver metastases
🔹 Grade ≥3 CRS: only 5%
Current 3L+ MSS CRC options rarely achieve response rates above single digits.
Small, single-center phase I study, but this is one of the more encouraging CAR-T signals we’ve seen in colorectal cancer.
The key question:
Can GUCY2C-directed CAR-T overcome the historical barriers that have limited cellular therapy in solid tumors?
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #ColorectalCancer #CAR-T @OncoAlert@myesmo@esmo_open
Why were there TWO trials—SOFT and TEXT?
Because there were TWO different questions:
❤️ SOFT: Does ovarian function suppression (OFS) add benefit?
🏆 TEXT: If OFS is used, is exemestane better than tamoxifen?
Together, these landmark trials established OFS as an important strategy in higher-risk premenopausal HR+ breast cancer and identified exemestane + OFS as the most effective option for reducing recurrence risk.
Francis et al. • SOFT/TEXT Trials
#BreastCancer #Oncology #SOFT #TEXT #MVOnco