Don't miss this great opportunity to learn #BSTpath from fantastic lecturers, with 150 cases to preview & a structured approach to this beautiful subspecialty.
Been attending since 2024 and it never disappointed me.
On-site & virtual! Maybe at some point I'll be able to attend in-person 🥺
#pathresidents #pathtwitter
Three variations on seminoma #testiscancer#gupath
#1 - seminoma w/transitions to embryonal carcinoma - differences in cytoplasm, nuclear contour, & nucleoli - both OCT-4(+); diffuse membranous labeling for CD117/D2-40 (seminoma) vs. CD30 (EC) = helpful differential stains
28 y/o M w/ 12 cm retroperitoneal mass attached to and infiltrating bowel wall.
What are your thoughts? 🔬
Credits🙏🏼: https://t.co/wQ8vnqUsZJ (check out free WSI here & many others! Great learning resource)!
@DanGrahamMD Oh cool that's a good point to see if prior biomarkers are abnormal! We called residual hyperplasia and see comment, mentioned the architecture changes.
No definite answer but more of sharing the findings. EMB with hormone therapy after initial dx of atypical hyperplasia/EIN. How would you sign out with these findings?
Another one from the same scenario that post tx bx with only focal papillary growth in the current bx. Figure 2-5 are PTEN in the papillary area compared to the normal adjacent gland, B-Catenin, PAX-2; In short, none of the biomarkers are helpful in this case.
@DanGrahamMD Amazing! In the third picture, we can still see some cells with bubbly pink cytoplasm, likely secondary to chemotherapy. Some tumor cells may not be affected by the treatment, giving it a "biphasic" appearance. The case was diagnosed as clear cell carcinoma based on morphology.
@DanGrahamMD The three markers are not always helpful and it would also be challenging to compare with the prior bx because the hormonal effect. Also I've learned that sometime these papillary structures are from endocervix and if it's very fragmented, it's not easy to tell apart.
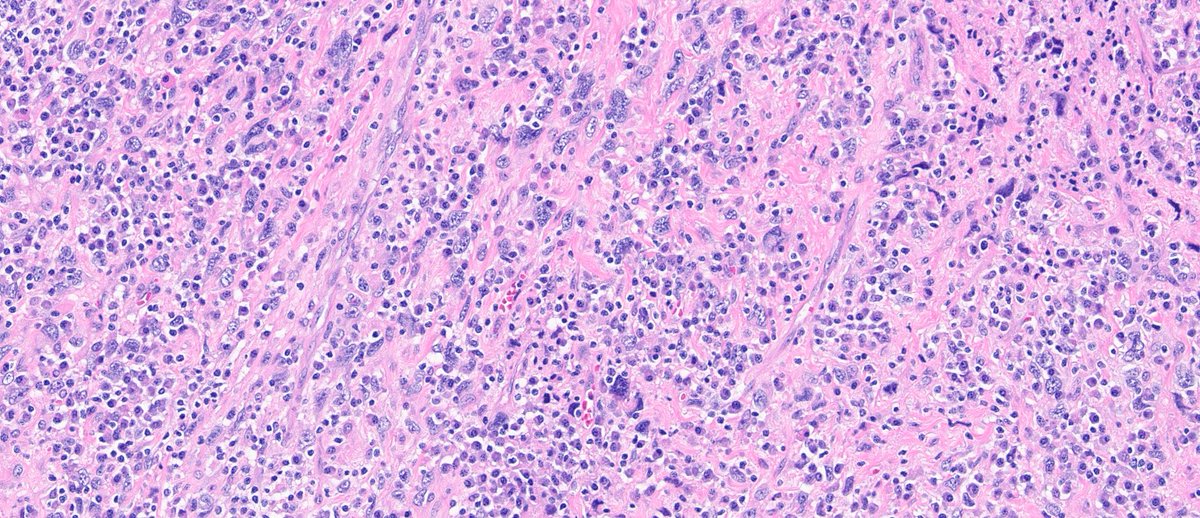
@LeukocyteLuke Great differentials! The case was worked up for sarcoma and negative for panK, CD34, S100, SMA, desmin, ALK, ALK DSF3. Eventually given the location, MDM2 was amplified.
@_Wondweson64 Nice! The case was worked up for sarcoma and negative for panK, CD34, S100, SMA, desmin, ALK, ALK DSF3. Eventually given the location, MDM2 was amplified.
@DanGrahamMD Excellent Dan! Great ddx. it is a intimal sarcoma eventually proven by MDM2. The dense plasmacytic infiltration really dilute the morphology in some way.
@slusagar Great thought! Not a transplant patient. The case was worked up for sarcoma and negative for panK, CD34, S100, SMA, desmin, ALK, ALK DSF3. Eventually given the location, MDM2 was amplified.