Medicare GLP-1 Bridge Program
“Pharmacies will be reimbursed at the wholesale acquisition cost of a drug, less the beneficiary copay of $50, plus a dispensing fee of $3 for each Medicare GLP-1 Bridge claim”
A whole $3 dispensing fee?
Golly gee, let me invest that into the S&P 500 and get my retirement fund set up!
Like it or not, the Inflation Reduction Act (IRA) is forcing unprecedented visibility into the 340B program.
@edsilverman of @statnews broke the story that @EliLillyandCo is requiring #340B hospitals to submit claims data or lose access to 340B discounts.
As I told Ed, this is a predictable consequence of the IRA's drug pricing provisions. The law created new pricing obligations for manufacturers, but policymakers never established a reliable way to identify which claims qualify for 340B pricing.
Here's the relevant section from his article:
"The issue has intensified thanks to the Inflation Reduction Act, which imposes a maximum fair price on drugs paid for by Medicare and obligates drugmakers to pay added inflation rebates in Medicare. But the requirement overlaps with the 340B program. Why? Drugmakers must offer hospitals the lower of the maximum fair price or the 340B price — and pay inflation rebates only on drugs not sold at the 340B price.
'The Inflation Reduction Act is forcing transparency into the notoriously opaque 340B program,' said Adam Fein, who heads the Drug Channels Institute and tracks prescription drug pricing and insurance coverage. 'The IRA’s maximum fair price requirements make it impossible to ignore the long-standing lack of visibility into 340B claims.'
He noted, however, that the federal government has not created a mechanism to identify 340B claims, and the HRSA maintains that it lacks the authority to do so. 'The result is a growing compliance dilemma that Congress never intended and regulators have yet to resolve,' he said."
Full article: https://t.co/XTgpm2X6EJ
𝐍𝐞𝐱𝐭 𝐅𝐫𝐢𝐝𝐚𝐲: 𝐃𝐫𝐮𝐠 𝐂𝐡𝐚𝐧𝐧𝐞𝐥𝐬 340𝐁 𝐈𝐧𝐝𝐮𝐬𝐭𝐫𝐲 𝐔𝐩𝐝𝐚𝐭𝐞 2026
The 340B program is at a crossroads.
Legal battles. Contract pharmacy restrictions. Rebate-model proposals. Expanding state legislation. New scrutiny of program economics.
Taken together, these developments are reshaping one of the most influential—and controversial—parts of the U.S. drug channel.
Next Friday, my colleague Tyler Novotny and I will present a live Drug Channels Institute webinar examining what these changes mean for manufacturers, covered entities, pharmacies, PBMs, employers, and other stakeholders.
We'll discuss:
• Will a 340B rebate model become reality?
• How the Net Pricing Drug Channel could reshape 340B economics
• The legal, regulatory, and legislative battles reshaping 340B
• Exclusive DCI data on the contract pharmacy marketplace and its leading participants
• How manufacturers are responding to the changing economics of 340B
• What comes next for 340B——and the stakeholders most likely to benefit or be affected
If your organization is affected by 340B, this session will help you understand what's changing, why it matters, and what may happen next.
📅 Friday, June 12
🕛 12:00 p.m. – 1:30 p.m. ET
Register here: https://t.co/OTVVdcutCQ
P.S. Can't attend live? Every registrant receives access to the full replay and slide deck.
#340B #DrugChannels #Healthcare #Pharmacy #PBM #HealthcarePolicy
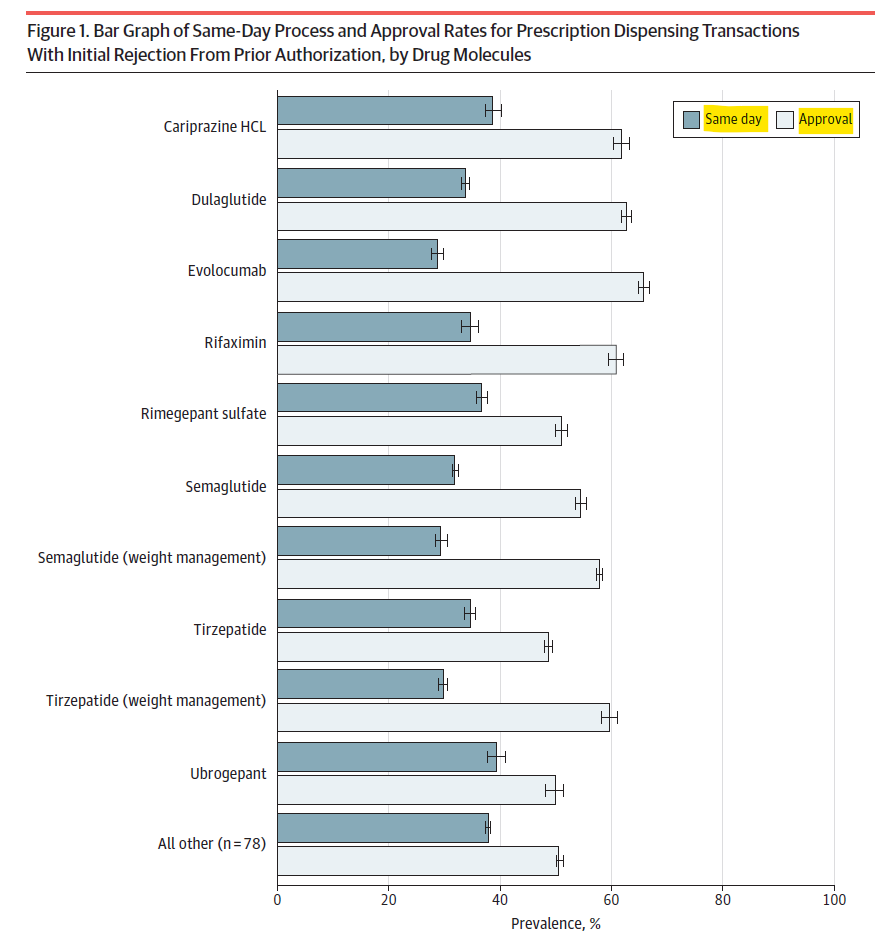
𝐏𝐫𝐢𝐨𝐫 𝐀𝐮𝐭𝐡𝐨𝐫𝐢𝐳𝐚𝐭𝐢𝐨𝐧: 𝐀𝐝𝐦𝐢𝐧𝐢𝐬𝐭𝐫𝐚𝐭𝐢𝐯𝐞 𝐂𝐨𝐦𝐩𝐥𝐞𝐱𝐢𝐭𝐲 = 𝐃𝐞𝐥𝐚𝐲𝐞𝐝 𝐂𝐚𝐫𝐞
New data on ~206,000 brand-name drug #prescriptions with initial prior authorization (PA) rejections:
• Only 35% cleared same day
• 65% delayed (median = 6 days)
• Nearly half (46%) were never approved
Multiple PA reviews and added rejection reasons significantly reduced same-day processing:
• Refills and complex cases were less likely to move quickly
• Medicaid patients and those with multiple conditions had lower approval rates
• Wide variation across drugs highlights uneven access 👇
For many patients, an initial PA rejection means delayed (or no) treatment.
Source: JAMA Health Forum https://t.co/LY2ryRhtmG
@DrugChannels Prior authorization isn’t just paperwork it delays cancer treatment.
• 90% of oncologists report delays (AMA/ American Society of Clinical Oncology)
• Delays linked to disease progression and lower survival
• 7% of physicians report delays contributing to patient death. #PBM
𝐇𝐨𝐬𝐩𝐢𝐭𝐚𝐥𝐬 & 𝐓𝐡𝐞𝐢𝐫 𝐅𝐚𝐤𝐞 𝐏𝐫𝐢𝐜𝐞𝐬
A must-read, hard-hitting piece from Anthony DiGiorgio @DrDiGiorgio on the economics of nonprofit hospitals and the growing gap between their public mission and financial reality.
He lays out the extensive subsidy ecosystem supporting hospitals:
• Property and sales tax exemptions
• Public funding (DSH payments, GME, research support)
• 340B Drug Discount Program revenues
• Market power–driven pricing from consolidated health systems
…among others
Then comes the key question:
"After all of those subsidy streams, what exactly is still unfunded"?
As he puts it, hospitals should provide a true accounting:
• What is the net Medicaid shortfall after supplemental payments?
• What is the real value of tax exemptions?
• Where does 340B revenue actually go?
• How are funds allocated across executive pay, administration, expansion, reserves, M&A, and lobbying?
Until we see that level of transparency, claims about underfunding deserve more scrutiny.
Strong, provocative piece.
👉 https://t.co/EJZ8DAHOQL
Great question. Answer: smart one.
Every dollar saved on benefits goes right to the bottom line. A public company with 100m shares can add 25c per share, annually, if they had a clue about their benefits.
You can start counting down to the shareholder lawsuits. This is money sitting on the table and every ceo is ignoring their fiduciary responsibilities.
Never trust your benefits vendors or consultants. Never.
Just run your name redacted contracts through an LLM, with training the AI vendor turned off
Most hospitals don't know their costs.
Things I've asked for that made them roll their eyes :
A BOM for surgeries
P&L for each insurance carrier
P&L for Medicaid or Medicare business
Why do they need consultants for everything. Why doesn't their CSuite know how to do any of it
Why do they use GPOs when prices are insane
Why do they work with carriers that underpay, late pay, deny everything, waste docs time with denial committees run by 97 yr old pediatricians.
Why do they make no effort to sell direct to employers (excluding those on https://t.co/WgRSm7lM7X to avoid all the carrier abuse , and avoid being sub prime lenders for patient OOP
Why do they abuse 340b
Why do facilities fees exist
Why do they abuse site neutrality
Why do they abuse patients with charge master based bills
Why do they not push for standard contract templates to reduce admin.
Why do they accept so many different ins plans
Anyone want to add more
And for context, remember I think the biggest insurance companies are worse
If you have a deal with the biggest PBMs you are getting ripped off
A simple way to realize this is to take both your insurance and PBM contracts and out them in @claudeai and just ask the following
"How am I getting ripped off and what can I do about it "
If you do, please post how it responds here so everyone can learn !
@HouseCommerce@RepHarshbarger Dead on the abuse of the 340B program. It has gone from “stretching scarce resources” to exploiting the entire healthcare system for huge profits that are often hundreds to thousands times more expensive than available generics drugs simply for profit.
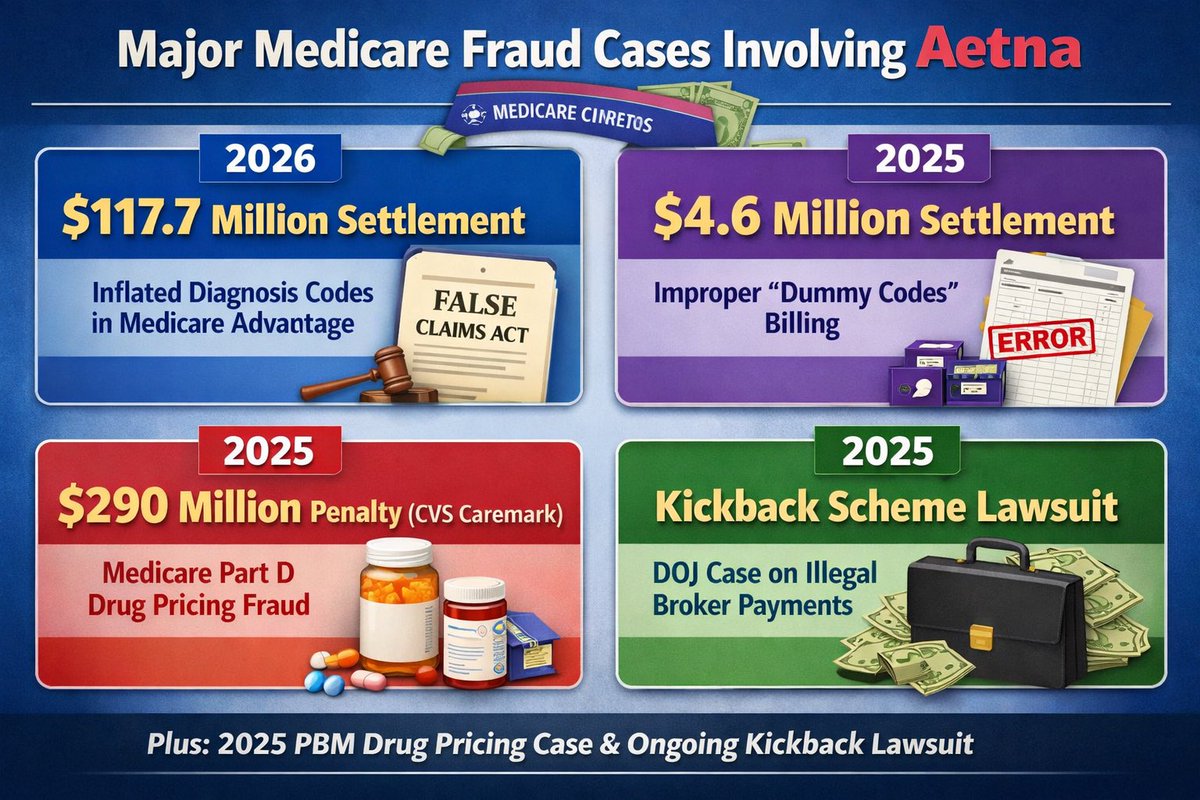
@Commpharmacy@BrandiChane Exactly. How are they not on the @JusticeOIG list. The @FTC has documented all the facts here and this isn’t the first time for Aetna or its subsidiaries including CVS Caremark. #FWA
Yesterday, CVS-Aetna agreed to pay $117.7 million to settle whistleblower claims that they defrauded Medicare by submitting incorrect diagnosis codes to increase their Medicare Advantage payouts.
Obvious question: Why are companies with documented histories of defrauding government programs still allowed to participate in them?
Read more about the settlement: https://t.co/NniIe56sef
VICTORY FOR PATIENTS!
After years of advocacy, @POTUS signed my PBM reforms into law, improving access to quality, affordable health care.
As a pharmacist, I know firsthand how TRANSFORMATIVE this is for patients and pharmacies.
More to come - this is just the start!
Greg Gutfeld spoke for millions of us 🔥🔥🔥
“We had dozens of deaths where you guys didn’t say sh*t… here’s 3 pages of women who have been m*rdered by illegal aliens.”
“You can’t call me a monster for saying all these people get deported. I don’t care!”
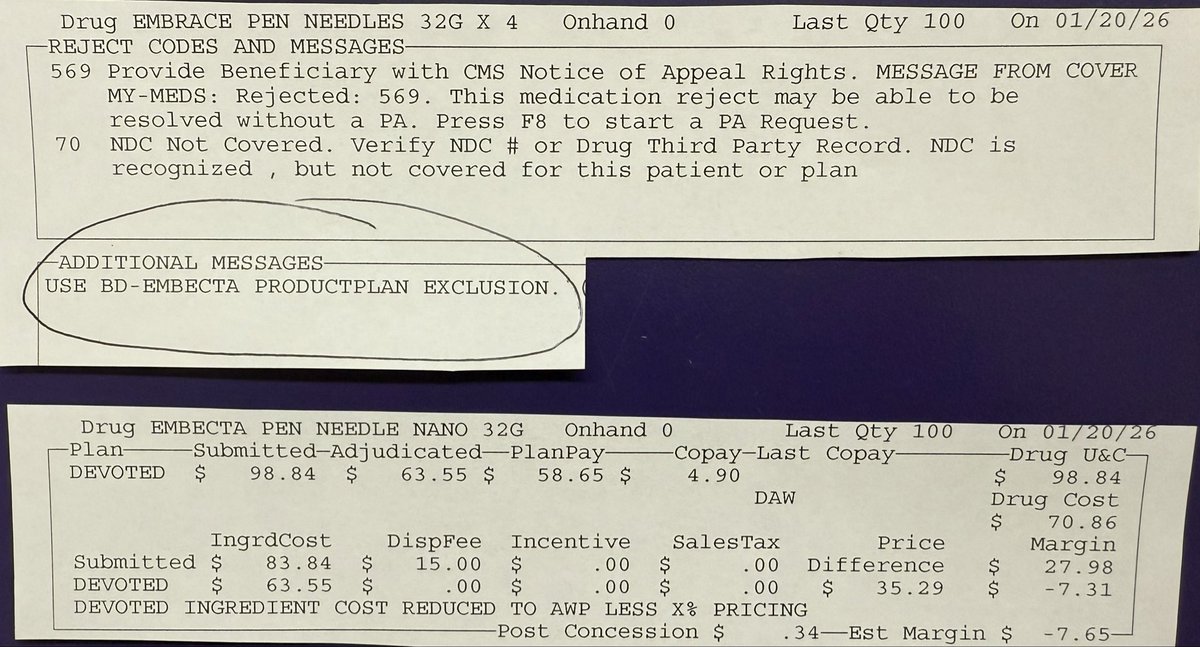
Send a claim for a Medicare Advantage patient for some pen needles for their insulin pens…
Find an inexpensive brand for $6.31 for a box of #100
NDC not covered.
Use BD-EMBECTA PRODUCT ONLY.
Find the Embecta Brand they want, box of #100 costs $70.86
Bill the @DevotedHealth plan for the pen needles:
Patient copay $4.90
Plan pays $58.65
Total paid $63.55
Loss of $7.65 before I even order the product.
I’d be better off cashing the cheap one out matching their $4.90 copay (this patient would bitch hard about the price) and losing $1.41
But why can’t the PBM @CVSHealth just cover the cheaper product to begin with?
Follow the money. Always. They get a kickback out of the more expensive product. Plain and simple. Doesn’t matter what’s cheaper for the patient or what the pharmacy can purchase it from their wholesaler.
The PBM cares only about what their profit margin will be. Nothing else matters to them.