A newly developed ICMR-NIN 13-Food-Group Score is simple, practical tool to assess dietary diversity among children. To enable healthcare professionals, teachers & community workers to quickly identify nutritional gaps n children at risk of micronutrient deficiencies etc....etc
By evaluating intake of 13 different food groups i.e. this tool promotes early nutrition screening, timely dietary counseling & targeted interventions. Its easy-to-use format makes it suitable for use in clinics, schools & community health programs, supporting improved child growth, development & overall nutritional well-being.
Early identification of dietary gaps can make a significant difference in preventing malnutrition & ensuring healthier futures for our children. https://t.co/asrCpUAhsz
@gmsubbarao@ICMRNIN@JPNadda@MoHFW_INDIA
Researchers at the University of Milan have identified that an enzyme called phospholipid transfer protein (PLTP) can effectively mobilize cholesterol from arterial plaques, sending it back into the bloodstream for natural disposal. This discovery is a potential game-changer because, unlike current treatments that primarily focus on preventing new plaque from forming, this method actually targets and dissolves existing blockages.
Atherosclerosis occurs when cholesterol and inflammatory cells create stable, hardened deposits in artery walls that resist traditional removal methods. When these plaques become too large, they severely restrict blood flow, often necessitating invasive procedures like stents or bypass surgery to prevent heart attacks or strokes.
The PLTP enzyme acts as a natural extraction system, pulling cholesterol out of the arterial wall and transferring it to HDL, or "good cholesterol," for transport to the liver. Scientists found that many people have naturally low levels of this activity due to genetic factors, which is why they have developed a gene therapy to boost PLTP expression directly where it is needed most.
In animal models, this localized boost in enzyme activity resulted in a 40% reduction in plaque volume in just three months, allowing narrowed arteries to reopen to nearly their original diameter. These results suggest that plaques not only become smaller but also more stable, which significantly lowers the risk of a sudden rupture that could cause a cardiac event.
While human clinical trials are currently focusing on patients with severe coronary artery disease who cannot undergo surgery, the long-term goal is a biological "reversal" of decades of arterial damage. If successful, this could shift cardiovascular medicine away from mechanical bypasses and toward a more natural, enzymatic cleaning of the circulatory system.
Researchers at the University of Milan have identified that an enzyme called phospholipid transfer protein (PLTP) can effectively mobilize cholesterol from arterial plaques, sending it back into the bloodstream for natural disposal. This discovery is a potential game-changer because, unlike current treatments that primarily focus on preventing new plaque from forming, this method actually targets and dissolves existing blockages.
Atherosclerosis occurs when cholesterol and inflammatory cells create stable, hardened deposits in artery walls that resist traditional removal methods. When these plaques become too large, they severely restrict blood flow, often necessitating invasive procedures like stents or bypass surgery to prevent heart attacks or strokes.
The PLTP enzyme acts as a natural extraction system, pulling cholesterol out of the arterial wall and transferring it to HDL, or "good cholesterol," for transport to the liver. Scientists found that many people have naturally low levels of this activity due to genetic factors, which is why they have developed a gene therapy to boost PLTP expression directly where it is needed most.
In animal models, this localized boost in enzyme activity resulted in a 40% reduction in plaque volume in just three months, allowing narrowed arteries to reopen to nearly their original diameter. These results suggest that plaques not only become smaller but also more stable, which significantly lowers the risk of a sudden rupture that could cause a cardiac event.
While human clinical trials are currently focusing on patients with severe coronary artery disease who cannot undergo surgery, the long-term goal is a biological "reversal" of decades of arterial damage. If successful, this could shift cardiovascular medicine away from mechanical bypasses and toward a more natural, enzymatic cleaning of the circulatory system.
Most adults who get a routine physical have their liver checked through one number: ALT. If it sits under 40, the system moves on. But ALT only rises when liver cells are actively dying in numbers large enough to spill enzymes into the blood. The slow scarring process that defines the dangerous form of fatty liver disease can advance for years without enough ongoing cell death to push ALT out of range. The standard panel reads normal. The liver is not.
A study in Hepatology biopsied 51 patients with fatty liver disease who all had normal ALT. Twelve had bridging fibrosis. Six had cirrhosis. That is 35 percent with advanced scarring while every blood test said the liver looked fine. The histologic picture in normal-ALT patients was indistinguishable from those with elevated ALT. Selection bias matters: the biopsied group was selected from unexplained liver enlargement and donor evaluations, not population screening. But the existence of substantial fibrosis behind a normal ALT is well established.
Fatty liver disease, recently renamed MASLD (metabolic dysfunction-associated steatotic liver disease) to reflect its metabolic origins, sits in about 25 percent of adults globally per a 2016 meta-analysis of 8.5 million people. Among MASLD patients: 51 percent obesity, 22 percent type 2 diabetes, 39 percent hypertension, 42 percent metabolic syndrome. The disease is the hepatic manifestation of insulin resistance. If you carry any of those metabolic markers, the question is not whether your liver is at elevated risk, but what your imaging and FIB-4 actually show.
Three things catch liver damage earlier than ALT. Imaging is the most direct. Abdominal ultrasound detects steatosis once hepatic fat exceeds roughly 30 percent. FibroScan measures liver stiffness as a non-invasive proxy for fibrosis. MRI-PDFF quantifies fat content with the highest accuracy. FIB-4 is a calculated score using age, AST, ALT, and platelet count: age times AST divided by (platelet count times the square root of ALT). A FIB-4 below 1.45 reliably excludes advanced fibrosis with a 95 percent negative predictive value. Above 3.25 warrants hepatology referral. Between those two numbers is an indeterminate zone that needs further workup. GGT is a sensitive marker of hepatic and biliary dysfunction that often rises before ALT does, particularly in the context of insulin resistance. All of these are available through direct-pay labs without a prescription.
Catching MASLD early matters because the intervention has strong evidence. A 52-week prospective study of 293 NASH patients showed that 5 percent body weight loss produced NASH resolution in 58 percent of patients. Ten percent body weight loss produced NASH resolution in 90 percent and fibrosis regression in 45 percent. Mediterranean diet, resistance training, and management of insulin resistance reduce hepatic fat independent of weight change. The window to intervene is wide on the left side of the trajectory and narrow on the right. By the time ALT flags the problem, the most damaging stage of the disease has usually already arrived.
Mofrad et al., Hepatology, 2003.
Younossi et al., Hepatology, 2016.
McPherson et al., Gut, 2010.
Vilar-Gomez et al., Gastroenterology, 2015
Source Courtsey William Wallace PhD
UACR: The Fifth Vital Sign for Cardiometabolic Risk
What Every Physician Should Know About UACR
✅ Urine Albumin-to-Creatinine Ratio (UACR) is not merely a kidney test—it is a window into systemic vascular health.
✅ Albuminuria reflects endothelial dysfunction and microvascular injury long before eGFR declines.
✅ A patient may have normal serum creatinine and normal eGFR but still have significant kidney and cardiovascular risk if UACR is elevated.
UACR Categories
🟢 <30 mg/g: Normal to mildly increased
🟡 30–300 mg/g: Moderately increased albuminuria (early kidney damage)
🔴 >300 mg/g: Severely increased albuminuria (high renal and CV risk)
Why UACR Matters Beyond the Kidney
An elevated UACR predicts: • Progression of CKD
• Heart failure hospitalization
• Myocardial infarction
• Stroke
• Cardiovascular mortality
• All-cause mortality
The Cardiometabolic Continuum
Albuminuria → Endothelial dysfunction → Vascular injury → Atherosclerosis → Heart failure, MI, Stroke
Who Should Be Screened?
✔ Type 1 diabetes ≥5 years duration
✔ All patients with Type 2 diabetes at diagnosis
✔ Hypertension
✔ CKD risk factors
✔ Established cardiovascular disease
✔ Obesity and metabolic syndrome
A Practical Clinical Message
A patient with:
eGFR = 90 mL/min/1.73m²
UACR = 150 mg/g
is at much higher cardiovascular risk than a patient with:
eGFR = 60 mL/min/1.73m²
UACR <30 mg/g
Treatment Implications
When UACR is elevated: ✔ Optimize BP control
✔ Intensify glycemic management
✔ Use RAAS blockade when indicated
✔ Consider SGLT2 inhibitors in appropriate patients
✔ Consider finerenone in eligible diabetic CKD patients
✔ Address obesity, smoking and dyslipidemia
CME INDIA Take-Home Message
🔹 Creatinine tells you how much kidney function is left.
🔹 UACR tells you how much vascular damage is occurring.
🔹 Never assess kidney risk with eGFR alone. Always pair eGFR with UACR.
Bottom Line
UACR is emerging as one of the most powerful and underutilized biomarkers for early detection of kidney disease, cardiovascular disease, and heart failure risk. Every physician should make UACR a routine part of cardiometabolic risk assessment.
CME INDIA Pearl:
"The kidney leaks albumin before it loses function. Detect the leak early, and you may prevent both kidney failure and cardiovascular events." — Dr N.K. Singh, CME INDIA.
🚨 Obesity care has changed dramatically since AGA first introduced the POWER framework in 2017.
Our new commentary in Gastroenterology, “Revisiting POWER in the GLP-1 Age,” updates the framework to reflect today’s treatment landscape, including:
☑️ GLP-1 receptor agonists
☑️ Endoscopic bariatric and metabolic therapies
☑️ Expanded bariatric surgery indications
☑️ Advances in precision medicine
The commentary emphasizes that medications are just one piece of comprehensive obesity care. Gastroenterologists and hepatologists are uniquely positioned to help patients navigate a growing range of treatment options while managing obesity-related conditions such as:
🫀 MASLD
🔥 GERD
🩺 Gallbladder disease
📖 Read more here: https://t.co/aqdd86hK3w
Join the authors for a live webinar on July 15: https://t.co/bCZomJRmJv.
Gastroenterology
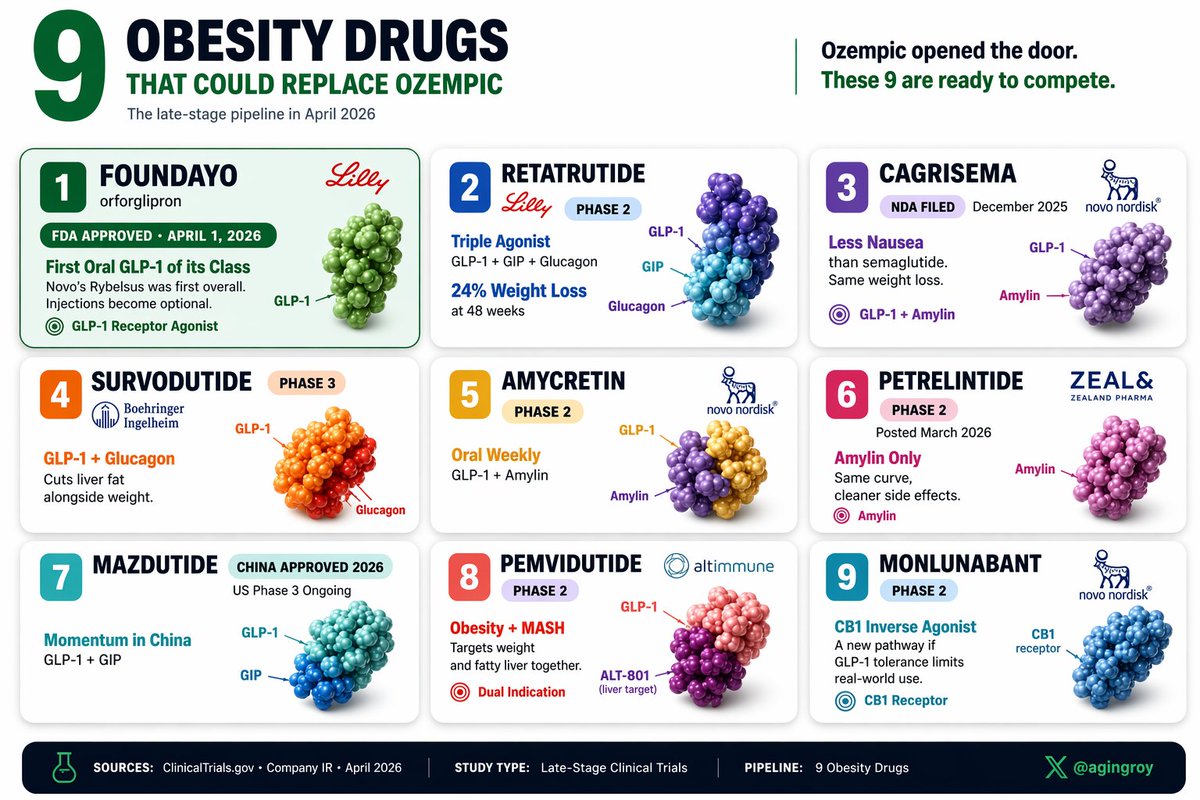
3 years ago, the obesity drug market was basically Ozempic.
Today, it's 9 drugs deep in late-stage. Here's what each one actually adds:
1. Foundayo: latest oral GLP-1. @US_FDA approved April 1, 2026. Injections become optional.
2. Retatrutide: 24% weight loss at 48 weeks (Phase 2). Triple agonist.
3. CagriSema: less nausea than semaglutide. NDA filed December 2025.
4. Survodutide: GLP-1 + glucagon. Cuts liver fat alongside weight.
5. Amycretin: oral weekly. GLP-1 + amylin. Phase 2.
6. Petrelintide: amylin only. Phase 2 posted March 2026.
7. Mazdutide: China approved 2026. US Phase 3 ongoing.
8. Pemvidutide: obesity + MASH dual indication.
9. Monlunabant: CB1 inverse agonist. Phase 2.
The next pharma cycle may not be Novo vs Lilly. It's shaping up as mechanism vs mechanism.
Ever feel like "healthy eating" advice changes every week? Science is finally fixing it
We are witnessing a paradigm shift in how we study food. No more guessing games or unreliable food diaries. Tech is finally giving us the clear answers we deserve
OA: https://t.co/aUOxrBswZN
Real world evaluation of tirzepatide vs semaglutide
In obese individuals without diabetes
Tirzepatide associated with a lower risk of cardiovascular events,
A similar safety profile.
https://t.co/R1XM1SqOTv
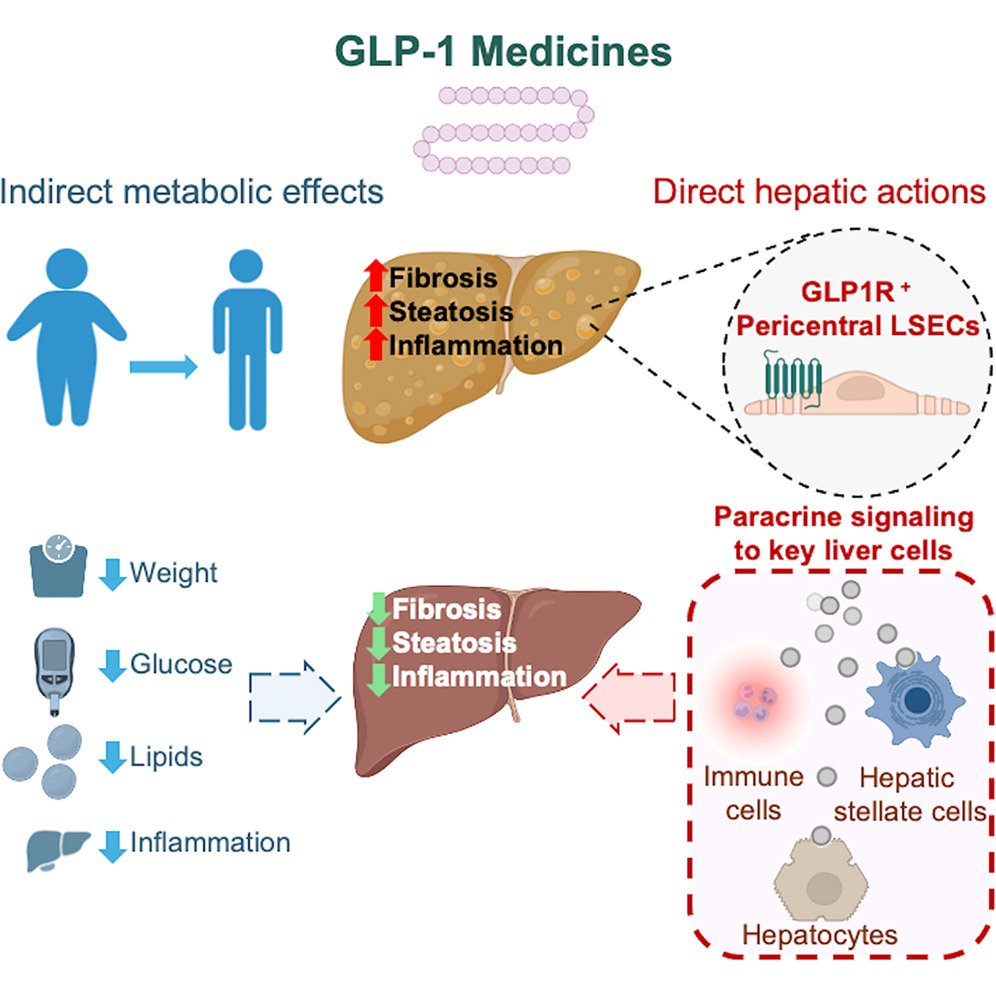
The weight-loss-independent hepatoprotective benefits of semaglutide are orchestrated by intrahepatic sinusoidal endothelial GLP-1 receptors.
https://t.co/xnMLLYA9bR
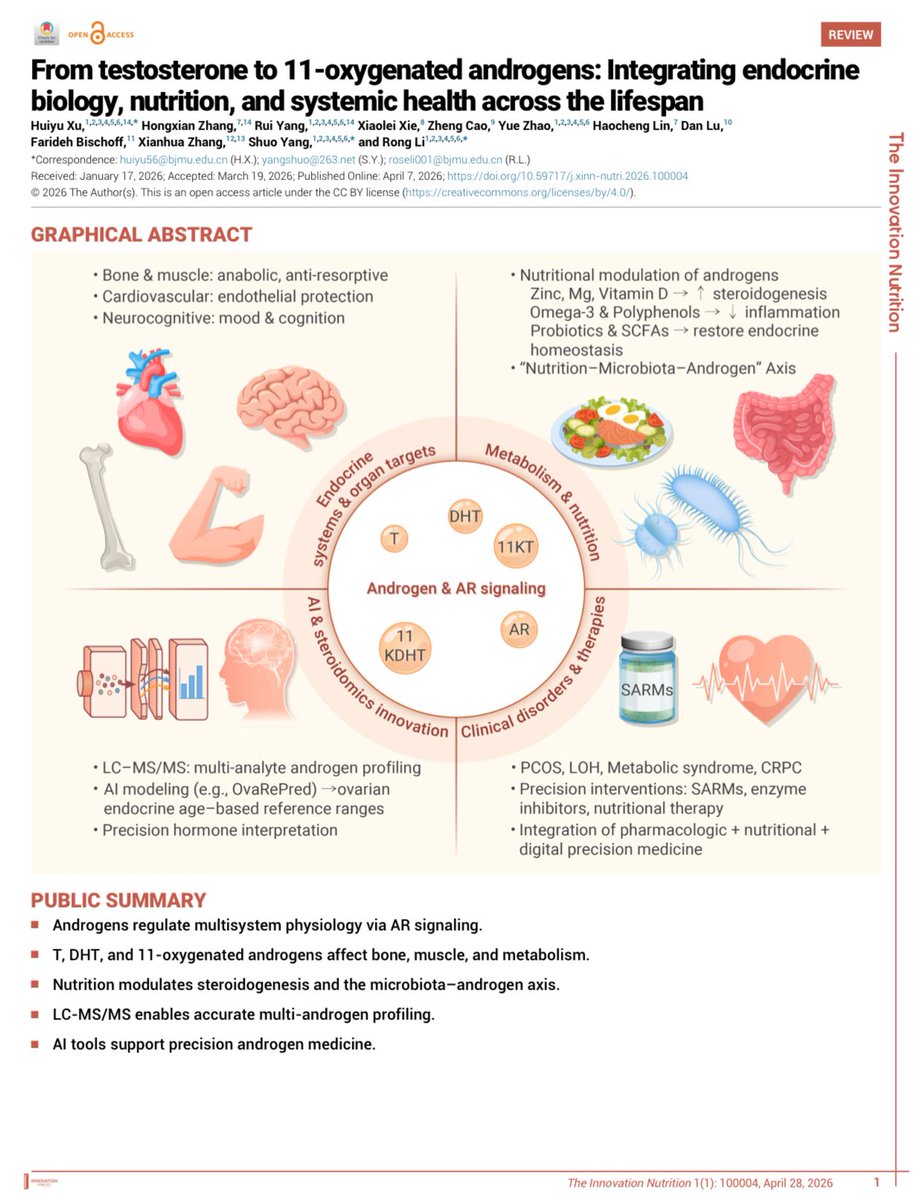
Zinc, Magnesium, and Polyphenols aren't just supplements, they're hormone modulators.
This latest review by Xu et al. explains how 11-oxygenated androgens link nutrition to systemic health.
OA: https://t.co/YXxBe5QEWJ
#MedTwitter#Biohacking#ScienceNews#Nutrition
@SafariBagsIndia what kind services u r providing to customers? So called trusted brand we believe u but u are refusing for warranty. U don’t have any record, neither confirmation mail from company regarding warranty after registration .