A Mayo Clinic-developed artificial intelligence (AI) model can help specialists detect pancreatic cancer on routine abdominal CT scans up to three years before clinical diagnosis. It identifies subtle signs of disease before tumors are visible, when curative treatment may still be possible. The findings, published in Gut, mark a milestone in Mayo Clinic's multiyear research effort to enable earlier detection of one of the deadliest cancers.
Learn more: https://t.co/EJySSkaW3P
@otis_reid@j_kalla We still don’t really know what’s optimal start time though. Data is unclear with some retrospective studies showing improved outcomes with 1pm as cuttoff.
@otis_reid@j_kalla The good news is most patients get their first 4 of doses b4 3p anyway bc most community infusion centers close 5p & you need more time for chemo-IO . But w/ single agents, shorter infusion times being adopted and subcut injections being approved this could affect survival.
@JimmySteier@EricTopol 77% vs 83.8% stage IV in early vs late ToD arm. I don’t think that numerical difference would have created these significant HRs for PFS and OS. I’m sure @Nature peer reviewers would have addressed if it was and issue. The data is consistent with prior retrospective studies.
@j_kalla@otis_reid 77% stage IV in early ToD arm and 83.8% in late ToD arm. I don’t think that numerical difference would have created these significant HRs for PFS and OS.
@dr_yakupergun Adds to the mounting data that show ToD impacts survival outcomes across many tumor types(mainly retrospectice/MA until now) . Do we really need more randomized data to operationalize this cost-neutral intervention that could dramatically affect survival? @TumorBoardTues
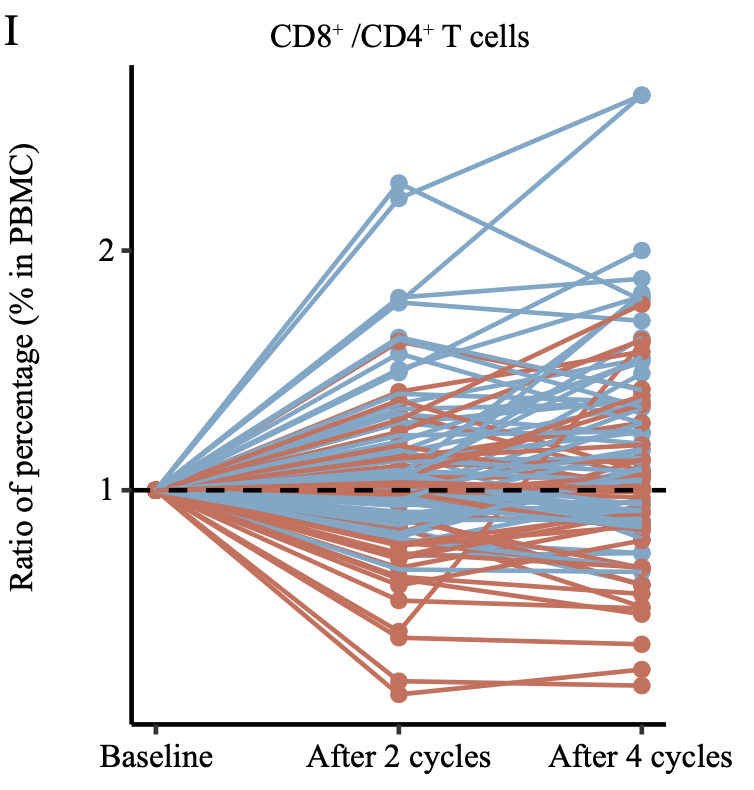
More evidence that #immunotherapy works better in the morning.
In a prospective, randomized phase III trial, giving first-line chemo-immunotherapy earlier in the day (<15:00) nearly doubled PFS (11.3 vs 5.7 mo, HR 0.40) and improved OS (28.0 vs 16.8 mo; HR 0.42) in advanced NSCLC.
More effective, no added cost and easy to implement.
Likely reflects circadian immune rhythms with greater CD8⁺ activation and less T-cell exhaustion.
https://t.co/q4JrFU4yws @OncoAlert
“You’re too young” is not a diagnosis.
Colorectal cancer is now the leading cause of cancer death for men and women under 50.
It is one of the only major cancers still increasing in incidence.
This is not a future problem. This is already here.
A few things that matter:
• Screening works. Average-risk screening starts at 45, earlier if you have risk factors.
• Symptoms in young people are real and should never be brushed off.
• New rectal bleeding, constipation, diarrhea, bowel habit changes, abdominal pain, or unexplained anemia are warning signs.
If symptoms are new or persistent, push for evaluation.
If you’re eligible, get screened.
If someone you know is being dismissed, advocate for them.
https://t.co/LV9uxWJLKK
I <3 my ‘26 @Tesla MY w FSD v14.2.2.2. This tech is going to save a lot of lives when more widely adopted. Feels amazing to be contributing to the FSD training miles for AVs. My only complaint is their maps/nav is not the best. Hopefully will be> google/apple maps over time.
⏱️ Oncologists: save patients time & reduce infusion center overload - infuse pembro in 10 minutes instead of 30. ⏱️
Safety data now out in @JCOOP_ASCO, IRR low (4%) & similar to 30 min infusion. @Oncoalert@JCO_ASCO
https://t.co/oWlAq5zujn
@YJanjigianMD@Aiims1742@NEJM@OncoAlert In practice, after ESOPEC many medoncs give the full Peri-op FLOT course preoperatively to avoid delays/cancellation of adjuvant therapy (if patients don’t recover PS after surgery). Curious if a full neoadj Durva-FLOT with adjuvant durva is reasonable? @TumorBoardTues wwyd
Vitamin B12 for prophylaxis of capecitabine-associated hand–foot syndrome
💥Oral methylcobalamin reduced capecitabine-related HFS in HER2-negative early BC, with no added safety concerns
💬A simple prophylaxis option to support treatment adherence
https://t.co/khCOH0RDv7
@BrandonLuuMD Fascinating! In the real world how does one implement this across all tumor types in a large oncology practice. Has anyone accomplished this? Should patients demand morning treatments with ICIs. Makes the case stronger for switching to subcu formulations when possible.
@UGrewalMD@GIMedOnc@GIcancerDoc@TumorBoardTues@AmanChauhanMD@IHC_guy NGS showed TP53. Her2 neg(0), pdl1 neg. 🩸 NGS nothing new. high mitoses, ki67 80%. Poor diff. Fits with LCNEC.
Found DLL3 IHC via mayo.Thanks! will reach out to Winship and try for comp use of Tarla in the future if no trial and DLL3+
Good news- LFTs improved s/p c1 C/Etop
Need the GI onc hive opinion:
43 yo M, PS 0, stg IV G3 Large cell-NEC cecum w extensive liver Mets (causing transaminitis) & TLS. Admitted & started C1 Carbo/etop. NGS pending. Leaning 2ward Carbo/Etop/nivo then nivo. Wwyd? @GIMedOnc@GIcancerDoc@TumorBoardTues@AmanChauhanMD
@UGrewalMD@GIMedOnc@GIcancerDoc@TumorBoardTues@AmanChauhanMD Tissue NGS negative. CTNNB1 and MEN1 mutation noted but germline was negative. No APC mutation. Liquid NGS pending. Looking for commercial DLL3 testing now. Looks like Winship has a Trial (NCT04429087) that I found online. do you do pre-trial DLL3 testing for eligibility?