We've released a #new State-of-the-Art Review, "The Effect of General Anesthesia and Mechanical Ventilation on the Echocardiographic Evaluation of Cardiac Function!"
Read it now: https://t.co/cbmJ46fd5C
🫀NEW GUIDELINE🫀
Read our new #ASEGuideline, "Guidelines for the Intraprocedural Imaging for Mitral Valve Transcatheter Edge-to-Edge Repair!" https://t.co/mPEUDziCfD
🚨 Nuevos grados de severidad en el corazón derecho según la ASE.
Cambia la evaluación del VD, la AD y la arteria pulmonar:
❌ menos “normal/anormal”
✅ más grados de severidad
✅ más valor pronóstico
Si quieres estar al día en Eco, este hilo es para ti 👇🏼 🧵#CardioNova#Eco
📄 Can we finally measure RV volume accurately with simple echocardiography?
🔗 DOI: https://t.co/cHII0FgTLH
🫀 The right ventricle (RV) remains one of the most challenging chambers to assess—especially in congenital heart disease (CHD).
👉 Gold standard? Cardiac MRI
❗ But: expensive, time-consuming, and often requires sedation
✨ This study proposes a simple, fast, and accurate 2D echo-based method for RV volumetry—bringing us closer to true bedside quantification.
✨ The key idea:
👉 Model the RV using a cone-based geometric approach
➡️ Using only 2 standard echo views:
Apical 4-chamber (A4CH)
Parasternal short-axis (SAX)
📐 With just a few parameters:
✔ Cross-sectional areas (A4CH, ASAX)
✔ Tricuspid valve diameter
📊 Performance vs MRI:
🔥 Excellent agreement:
Systolic volume → ICC 0.98
Diastolic volume → ICC 0.96
📉 Minimal bias:
Δ systolic volume ≈ 0.1 mL
Δ diastolic volume ≈ 5.2 mL
➡️ Clearly outperforms traditional 2D models
💡 Why this matters clinically:
👉 Enables:
✔ Rapid bedside RV assessment
✔ Reduced need for repeated MRI
✔ Easier follow-up in paediatric & CHD patients
👉 Particularly valuable in:
Post-operative monitoring
Serial evaluations
Resource-limited settings
🚀 Key innovation:
👉 A mathematically robust yet practical model
➡️ Balancing accuracy + simplicity
➡️ Adaptable to different RV shapes
🚨 Bottom line:
2D echocardiography—when combined with smart modelling—can approach MRI-level accuracy for RV volumetry.
#Cardiology #Echocardiography #RightVentricle #CongenitalHeartDisease #CardiacImaging #CMR #Innovation #MedTech #PediatricCardiology 🫀📊
Coronary Anatomy in d-TGA — Yacoub Classification📚
👉Type A: LCA from sinus 1 and RCA from sinus 2 — the usual and most common pattern.
👉Type B: Single coronary ostium, from either sinus 1 or sinus 2, with early branching between the great arteries.
👉Type C: Two separate but closely adjacent ostia, usually near the posterior commissure; often managed like a high-risk transfer pattern.
👉Type D: LAD from sinus 1 and RCA + LCx from sinus 2 — LCx courses posteriorly around the pulmonary root.
👉Type E: RCA + LAD from sinus 1 and LCx from sinus 2, often with side-by-side great arteries and complex looping.
Anomalous Aortic Origin of a Coronary Artery (AAOCA) #2: Surgical Concept of Unroofing
👉Unroofing opens the shared aortic–coronary wall of an intramural segment, converting a tunneled coronary course into a wide, non-compressed neo-ostium.
👉It is best suited when the intramural course runs above the aortic valve; if the course is below the AoV, unroofing may be unsafe or inappropriate.
👉If dynamic compression persists in the Ao–PA corridor after unroofing, coronary reimplantation may be required to fully relieve ischemic risk.
Surgeons at CHOP say the birth day of the week is associated with surgical timing and postoperative brain injury in neonates with #congenital heart disease. Read more in #JTCVS Open: https://t.co/BlsufFd9qV
@JLynchMDPhD
🫀 Are we underestimating sudden cardiac death risk in HCM?
📊 For years, risk stratification in hypertrophic cardiomyopathy (HCM) has relied on clinical scores…
But are these models too simplistic for such a complex disease?
🔍 A recent editorial challenges the paradigm:
👉 Moving from risk scores → precision cardiology
⚠️ The problem with current models:
✔️ Based on static variables
✔️ Limited integration of imaging & genetics
✔️ “Low-risk” patients can still experience events
💡 Example:
A 5-year SCD risk of 4–6% translates to only ~0.8–1.2% per year…
👉 Small differences, big clinical uncertainty
🧠 New insight: the atrium matters
Traditionally, we focus on the LV… but:
➡️ The left atrium reflects chronic diastolic burden
➡️ Dysfunction may precede structural changes
📈 In “low-risk” HCM patients:
👉 Impaired LA strain (LA-GLS) predicted adverse outcomes
👉 Even when conventional scores were reassuring
🔬 Where are we heading?
The future of SCD prediction in HCM is multidimensional:
✔️ Advanced imaging (CMR, strain, LGE)
✔️ Genetics (variants, polygenic risk)
✔️ AI-driven ECG analysis
➡️ Not one tool… but integration of all
🚀 Take-home message:
We need to move beyond rigid risk categories and embrace a dynamic, patient-specific approach.
👉 Precision cardiology is no longer a concept—it’s becoming a necessity.
#Cardiology #HCM #SuddenCardiacDeath #CardioImaging #CMR #StrainImaging #CardioGenetics #PrecisionMedicine #AIinMedicine #CardiologyResearch #PhDLife 🧬✨
Damus–Kaye–Stansel Procedure #2: Side-to-End DKS Anastomosis
👉The side-to-end DKS technique connects the transected MPA to the lateral AAo, establishing an enlarged systemic outflow pathway.
👉Flap or patch augmentation may be required to optimize the anastomotic geometry, especially in side-by-side great artery relationships or size mismatch.
👉The key technical consideration is preservation of pulmonary root geometry and semilunar valve integrity to minimize late valve dysfunction.
PAPVR (RUPV–SVC): Anatomy, Hemodynamics, and Surgical Repair
👉PAPVR of the RUPV to the SVC/RA creates a significant L→R shunt, especially when the right pulmonary veins are involved.
👉Repair requires redirecting anomalous pulmonary venous flow to the LA while preserving unobstructed SVC drainage.
👉The double-patch technique and Warden procedure are two key strategies to balance pulmonary venous pathway, systemic venous pathway, and sinus node safety.
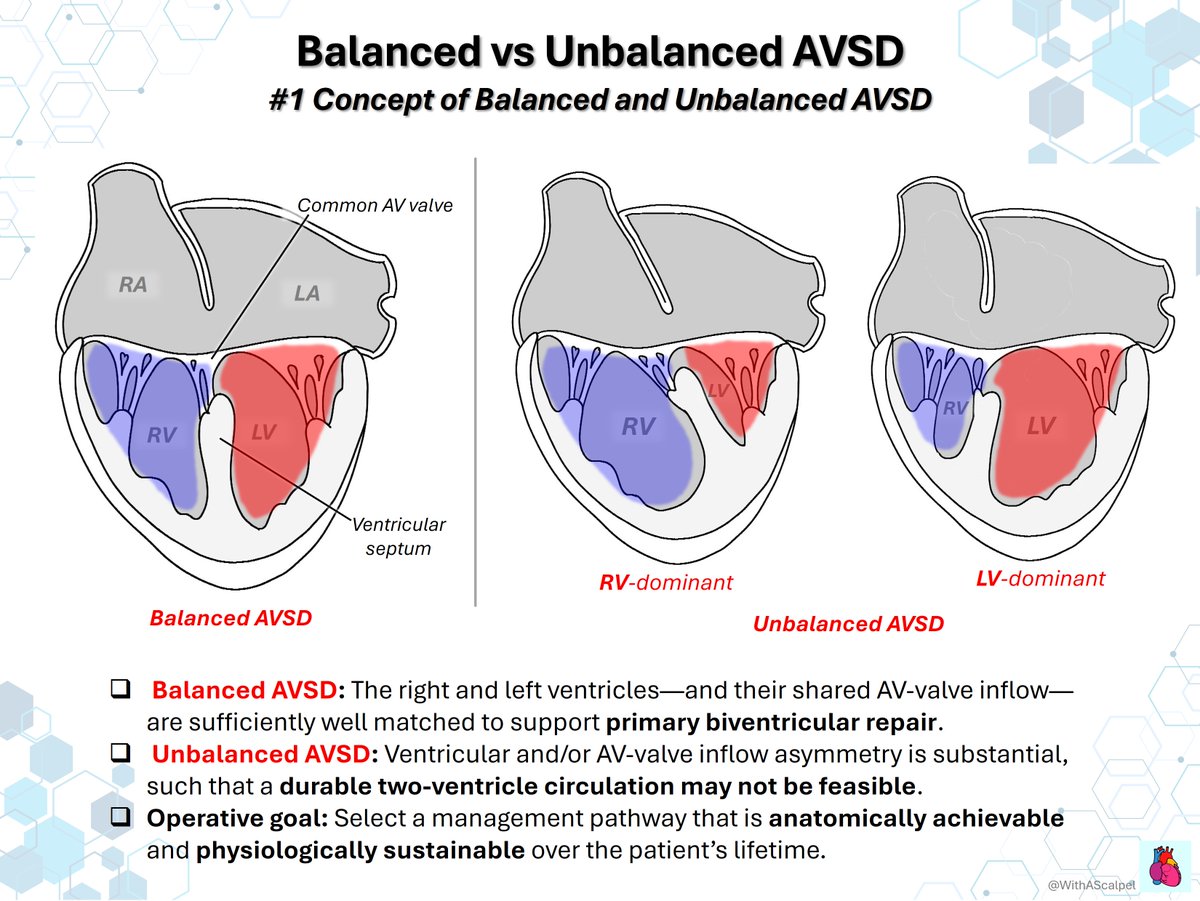
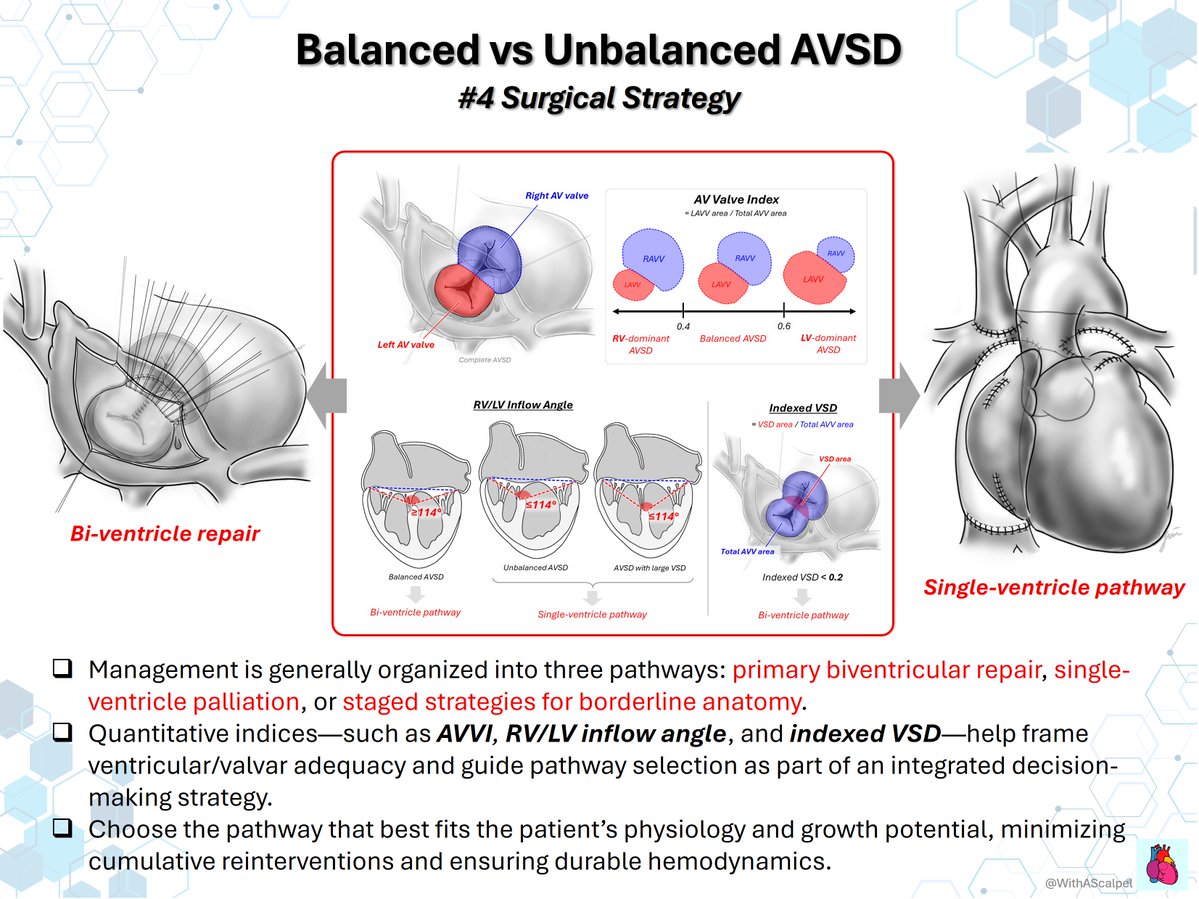
Balanced vs Unbalanced AVSD — From Anatomy to Strategy
👉Balanced AVSD supports a primary biventricular repair when ventricular size and AV-valve inflow are well matched.
👉Unbalanced AVSD requires careful assessment of AVVI, RV/LV inflow angle, indexed VSD, valve regurgitation, and ventricular function.
👉The goal is to choose the most durable pathway—biventricular repair, staged strategy, or single-ventricle palliation—based on anatomy and physiology.
Rules of #echofirst engagement
B4 showing & sharing knowledge on big stage be aware that attendees will take your images as example to follow so don’t show bad settings
👉 Color Doppler box too big
mention always why you have choosen (your goal should be best FPS, so color box not too big!)
👉 Vena contracta measurements need good resolution and gain setting optimization to avoid overestimating
👉 3D VCA must be explained with FPS! IF too low value not real! Show your settings
👉 Showing PISA EROA please make sure you have choosen correct settings with Nyquist and didn’t overestimate the radius! Mention that r > 0,9 is rarely seen
Always point out that Reg. Volume > 60 ml are rarely seen
Always show LV dimensions & Volume!
Always explain that a certain high amount of Regurgitation let’s say > 60 ml is only possible if LV Volume and LVOT SV are making sense
👉🎯 please Never Show That you have stopped using only one parameter
👉 IF you use 3D Volume Show your settings (FPS) and point not only EF but also LV / RV Volumes out.
Volumes matter more than EF
🎓 SCMR Webinar | The Congenital Heart Disease You May Be Missing
Could congenital heart disease be overlooked despite standard imaging protocols? Learn key clues that may help identify missed diagnoses.
👉 Register now: https://t.co/BpFsVpjNNb
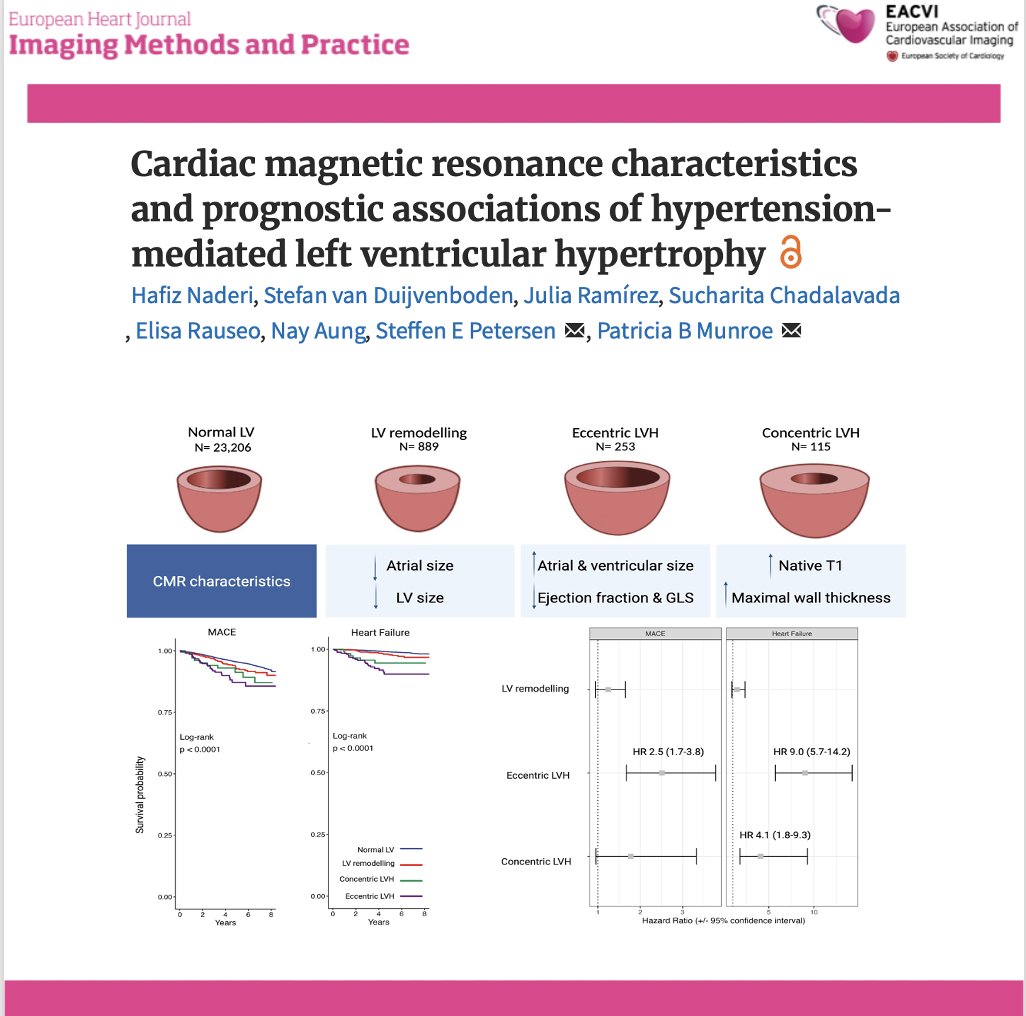
📄 Hypertension-related LVH: not all phenotypes carry the same risk
🔗 DOI: https://t.co/W1SFC0ZCz6
🫀 Hypertension is the most common cause of LV hypertrophy—but its cardiac expression is far from uniform.
This large UK Biobank CMR study (n >24,000) provides a comprehensive look at LVH phenotypes and their prognostic impact.
✨ Four CMR-defined phenotypes:
👉 Normal LV
👉 LV remodelling
👉 Eccentric LVH
👉 Concentric LVH
📊 As shown in the graphical abstract (page 2):
➡️ each phenotype has distinct structural and functional signatures
✨ Key findings:
🔹 Eccentric LVH = worst phenotype
➡️ Most impaired LV function (EF + strain)
➡️ Largest chambers
➡️ Highest risk:
MACE → HR 2.5
Heart failure → HR 9.0
🔹 Concentric LVH:
➡️ Highest wall thickness and native T1 (fibrosis)
➡️ ↑ Heart failure risk (HR 4.1)
➡️ No significant MACE association
🔹 LV remodelling:
➡️ Intermediate phenotype
➡️ Smaller chambers, milder changes
📊 Key pathophysiological insight:
👉 LVH is not a binary condition—but a spectrum of myocardial adaptation
➡️ From remodelling → concentric or eccentric hypertrophy
➡️ Driven by pressure load, volume load, and myocardial response
💡 Clinical take-home message:
👉 Not all LVH is equal
✔ Eccentric LVH → high-risk phenotype
✔ Concentric LVH → fibrotic, HF-prone phenotype
👉 CMR enables:
precise phenotyping
improved risk stratification
potential tailored treatment strategies
🚨 Bottom line:
In hypertension, LV geometry matters—because different phenotypes carry very different prognoses.
#Cardiology #CMR #Hypertension #LVH #CardiacImaging #HeartFailure #RiskStratification #PrecisionMedicine #UKBiobank 🫀📊