@sib313 This⬆️. if pt journey cannot be observed as a whole, in real-time, that ‘later in flow’, you mention, particularly from backdoor onward, remains invisible.
Most promising avenue for research in this area would see time as the fundamental unit of currency in healthcare systems. Talking about how time is spent (is a much better starting point for engaging op. management and clinicians in a 'productive' conversation about productivity.
Reminds of India and some countries in Africa jumping straight from analogue to mobile tech. Nothing like starting (effectively) from scratch to speed tech adoption (v little custom and practice to overcome)
@rcsloggett here is another one.
Just had confirmation from an ICS that they will not give CGM to those with #T2Diabetes in 2026- irrespective of what NICE said 3 years ago.
Evidence-free interventions are a big bugbear of mine. Especially for complex interventions rolled out across the NHS.
I have skeptical of SDEC services for some time.
First systematic review here done by a good team.
https://t.co/jNYmqz7WdR
1/
Like so many other ideas, this one reminds me of Hirschman's first law of the social sciences (intended playfully but often true): “Whenever a phenomenon in the social world is fully explained, it ceases to operate.”
The flurry of ~econ policy changes under the current administration has me routinely thinking about this lovely paper. (Also helpful when interpreting stock market news.)
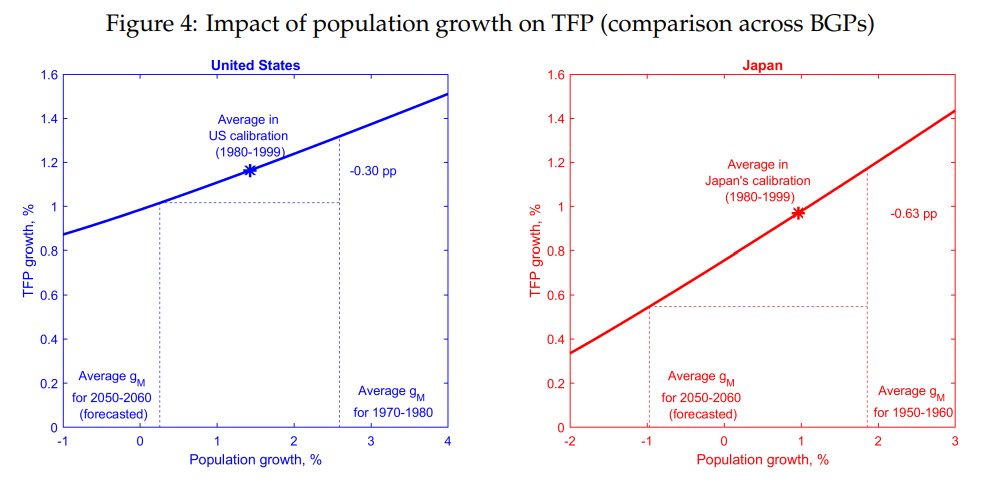
Faster population growth can lead to faster productivity and economic growth because a faster growing populations creates newer, more innovative firms.
There's been lots of work to make sure people who are on hospital waiting lists get the care needed. But @SivaAnandaciva says we should 'thinking more about what happened to the people who never came back for care' & where these missing millions might be. https://t.co/EtfXBAKYf1
@rcsloggett@HMAnderson39 I particularly like
NHS trusts do many different things and serve very different communities. So, just because one trust ranks higher than another doesn’t mean it’s “better.”
In a high intensity system Iike a healthcare system the optimal capacity is 80%
Hotels - that are high turn around etc - the optimal capacity isn’t 100% - if you are doing 100% you are probably leaving money on the table and also not doing your operational duties
I wouldn’t operate a hotel at more than 84-85% occupancy (yearly average) - need to do maintenance, upgrades, get the higher price per room etc etc
Nearly 5 months on and still no progress on the cuts to ICBs (or NHSE) because no funding for the reorg was ever agreed (eg see this from Greater Manchester). ICBs naturally waiting for cover (still not forthcoming) before cutting patient care to fund it
https://t.co/0Vo0JJDDT3
"This paper empirically analyzes the effects of mergers between complementary firms on competition and pricing."
NEW @nberpubs by Zack Cooper, Stuart Craig, Aristotelis Epanomeritakis, Matthew Grennan, Joseph Martinez, Fiona Scott Morton, Ashley Swanson: https://t.co/x7i9e0QaCy
We found that patients with multiple long-term conditions were more likely to experience fragmented outpatient care. This reinforces the need for these patients to have greater continuity of care in general practice to ensure better coordination of care. https://t.co/KIpB8rMjSB
Workforce substitution is NOT a solution.
It makes services more fragile. Harms patients. Costs more money in the long run.
Hospitals and services need to do the RIGHT things in the first instance.
Fin
https://t.co/dKxqRyRq8D
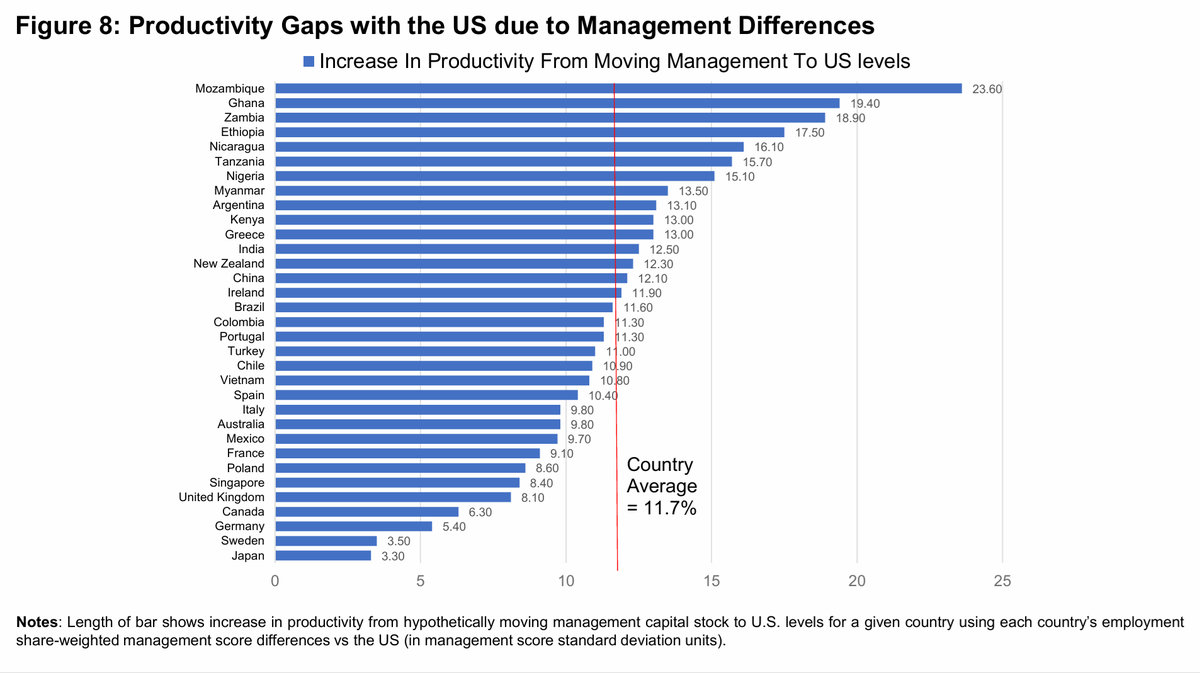
How much can the management quality of firms explain why countries are rich and poor? Our new NBER working paper ("Management and Firm Dynamism") attempts to tackle this question arguing that the management quality of firms matters considerably for economic growth
🚨 We're hiring! 🚨
Join us at the Health Foundation and be part of the NHS Productivity Commission.
We have 2 roles open:
🔹 Senior Economist
🔹 Senior Policy and Engagement Lead
Great opportunity. Find out more and apply here: https://t.co/hmugvvYW5h