Why can Hepatocellular Carcinoma (HCC) often be diagnosed without a biopsy, while most other cancers cannot?
The answer lies in its unique vascular transformation.
As HCC develops, it switches from portal venous to arterial blood supply, producing the classic imaging pattern:
🩸 Arterial Phase Hyperenhancement (APHE) → 🌑 Portal/Delayed Washout ± Capsule.
In a patient with cirrhosis or chronic HBV, this pattern is so specific that LI-RADS LR-5 allows a confident diagnosis without tissue confirmation in many cases.
Most other solid tumors lack such a unique imaging signature, making histopathology and molecular profiling essential before treatment.
A fundamental concept every oncology trainee should master.
#HCC #HepatocellularCarcinoma #LiverCancer #Oncology #MedicalOncology #Radiology #LIRADS #CancerEducation #FOAMed #MedEd #DrNB #DMOncology #CancerConceptsExplained #OncoTwitter #MedTwitter
Systemic therapy, gastrectomy, cytoreductive surgery, and hyperthermic intraperitoneal chemotherapy versus systemic therapy alone for gastric cancer with limited peritoneal metastases (PERISCOPE II): final results of a multicentre RCT phase III https://t.co/V8f6madiNj
If they’re all called Tyrosine Kinase Inhibitors (TKIs)… why can’t we use the same drug for every cancer? 🤔
Because TKI is a mechanism—not a target.
🔑 Every cancer is driven by a different molecular “lock,” and every TKI is designed as a specific “key.”
• Imatinib → BCR::ABL1 in CML
• Osimertinib → EGFR in NSCLC
• Sunitinib → VEGFR/PDGFR in RCC
Precision oncology isn’t about where the cancer started—it’s about what’s driving it.
Treat the mutation, not just the organ. 🎯
Which TKI do you think has transformed cancer care the most? 👇
#MedicalOncology #PrecisionOncology #TargetedTherapy #TKI #TyrosineKinaseInhibitors #CancerBiology #PrecisionMedicine #CML #LungCancer #NSCLC #RenalCellCarcinoma #Oncology #FOAMed #MedTwitter #CancerEducation
Online now: Systemic therapy, gastrectomy, cytoreductive surgery, and HIPEC versus systemic therapy alone for #gastriccancer with limited peritoneal metastases (PERISCOPE II): results of a phase 3 trial after an unplanned commissioned interim analysis
https://t.co/QGMzC2Rp8x
HIPEC vs PIPAC in Ovarian Cancer: High-Yield Comparison Every Resident Needs ✅
Strongest evidence for HIPEC is in interval debulking surgery after NACT (OVHIPEC-1 trial) — improved RFS & OS without increasing major complications.
Not routine in primary upfront CRS or most recurrent cases.
PIPAC remains investigational — useful in selected platinum-resistant/unresectable peritoneal disease (laparoscopic, repeatable, lower systemic toxicity).
Key practical points: • Achieve CC-0/CC-1 cytoreduction
• Cisplatin 100 mg/m² @ 40–43°C for 90 min (HIPEC)
• PIPAC: Low-dose cisplatin ± doxorubicin, every 6–8 weeks
Full infographic with indications, patient selection, contraindications, complications, flowcharts & guideline position 👇
Save for your notes & exam prep!
What’s your institutional practice with HIPEC in interval debulking? Drop your thoughts below 👇
#OvarianCancer #HIPEC #PIPAC #GynecologicOncology #MedicalOncology #OncologyEducation #DrNB #ExamPrep
MMR or MSI? One of the most common areas of confusion in oncology and pathology.
A simple way to remember it:
🧬 MMR = Machinery (IHC)
🔬 MSI = Mistakes (PCR/NGS)
✅ IHC checks whether the DNA mismatch repair proteins (MLH1, PMS2, MSH2, MSH6) are present.
✅ PCR/NGS measures the genomic consequence—microsatellite instability.
High-yield takeaway:
• dMMR ≈ MSI-H
• pMMR ≈ MSS
• MSI-L is uncommon and is generally managed similarly to MSS for most clinical decisions, including immunotherapy selection in colorectal cancer.
Save this visual for exam revision and daily oncology practice.
#MedTwitter #Oncology #Pathology #MolecularPathology #ColorectalCancer #Immunotherapy #MMR #MSI #PrecisionOncology #CancerEducation #FOAMed #MedEd #MedicalOncology #DrNB #CancerConceptsExplained
🔥off the press🔥
Durvalumab with gemcitabine-based CTx in advanced BTC: primary results from the phase IIIb TOURMALINE study
https://t.co/GGqyAGNB2s
@JHepatology
👉Consistent efficacy & safety across 7 different chemo regimes
@myESMO@EASLnews@ILCAnews@curecc
Not every premenopausal woman with early-stage HR-positive breast cancer requires ovarian function suppression (OFS).
The greatest benefit is seen in patients at higher risk of recurrence—particularly women aged <35 years, those with node-positive disease, those who remain premenopausal after chemotherapy, and those with other high-risk clinicopathologic features.
For high-risk patients, OFS + exemestane provides the greatest reduction in recurrence based on the SOFT and TEXT trials, while tamoxifen alone remains appropriate for many low-risk patients.
Choosing the right endocrine strategy means balancing recurrence risk with treatment-related toxicity and patient preferences.
#BreastCancer #MedicalOncology #BreastOncology #EndocrineTherapy #OvarianFunctionSuppression #OFS #Tamoxifen #Exemestane #SOFTTrial #TEXTTrial #Oncology #OncologyEducation #MedEd #FOAMed #CancerEducation #DrNB #DMMedicalOncology
How to interpret an NGS report 🧬
Finding a mutation is only one part of reading an NGS report. The real skill is knowing what to check, what it means, and how it changes patient management.
In this infographic, I share a practical 18-step framework that I use to systematically review every NGS report—from sample adequacy and quality metrics to driver mutations, gene fusions, biomarkers, resistance mechanisms, actionability, and final clinical integration.
A simple mnemonic—SAMPLE–GENES—can help ensure that no clinically actionable finding is overlooked.
Whether you’re a Medical Oncologist, Pathologist, Molecular Biologist, DM/DrNB resident, or preparing for tumor boards, I hope this serves as a practical bedside checklist.
💬 Which part of an NGS report do you find most challenging to interpret?
#NGS #PrecisionOncology #MolecularOncology #CancerGenomics #MedicalOncology #TargetedTherapy #LiquidBiopsy #GenomicTesting #Biomarkers #TumorBoard #OncologyEducation #MedEd #FOAMed #DrNB #MedicalEducation #CancerConceptsExplained
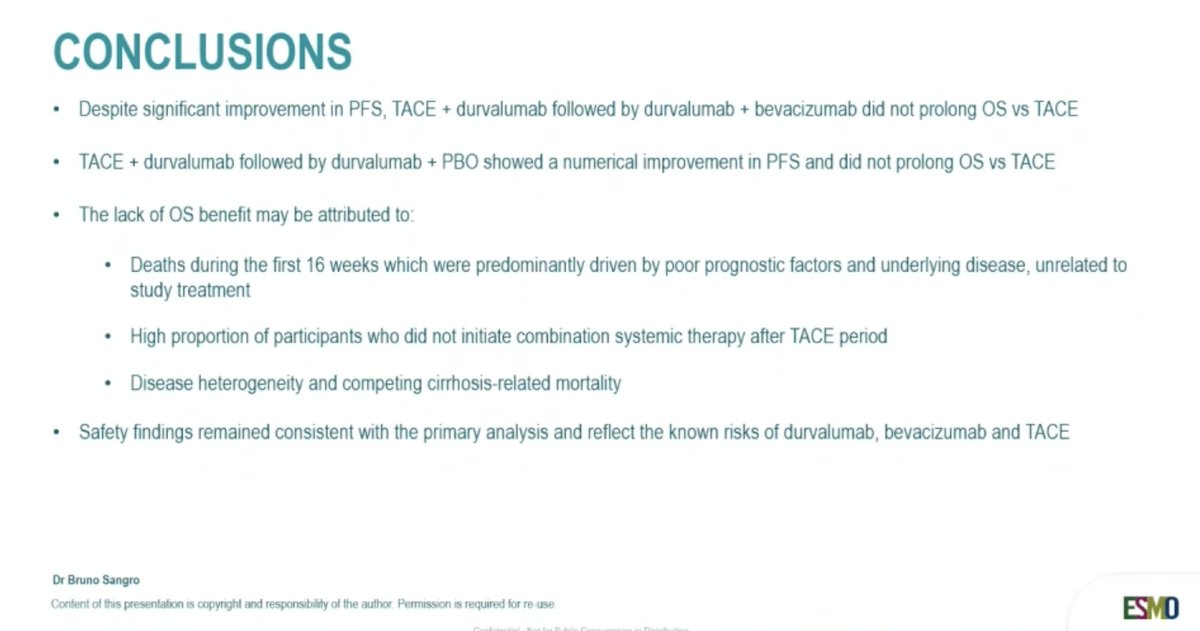
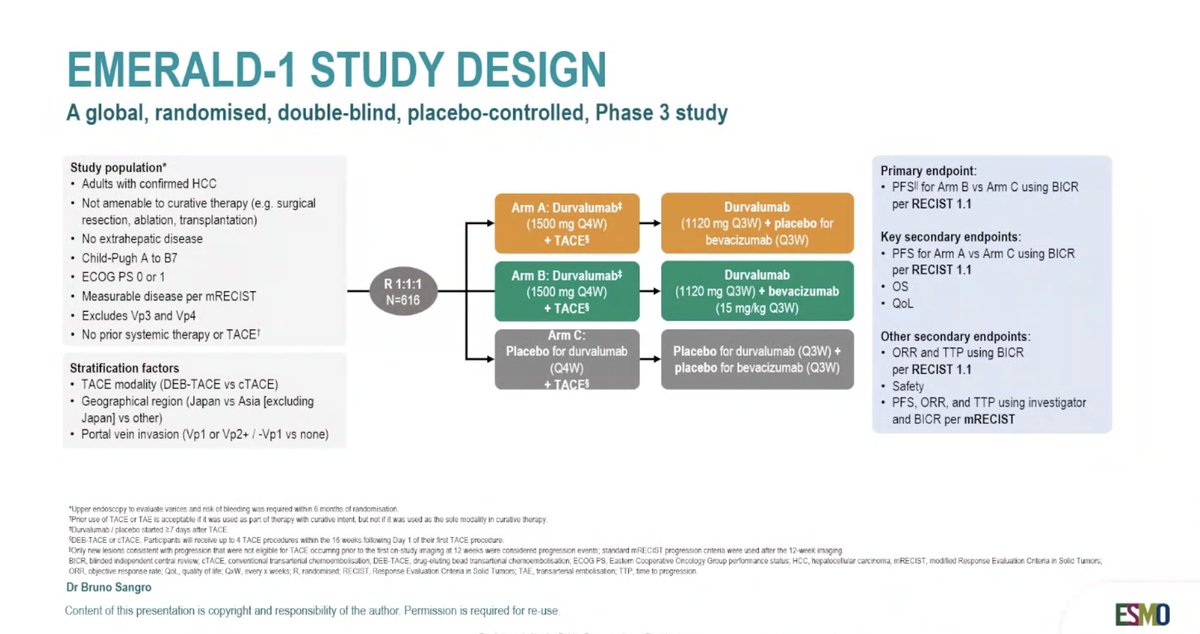
OS in EMERALD-1: A phase III study of durvalumab ± beva and TACE in unresectable embolisation-eligible HCC
👉OR & PFS improved
👉no OS benefit
🧐No safety concerns, but also not strongly supporting the combination
@myESMO@EASLedu@ILCAnews
Zolbetuximab plus gemcitabine and nab-paclitaxel in CLDN18.2+ metastatic PDAC: phase II GLEAM study
@ESMO-GI
👉Primary endpoint not met, no OS & PFS benefit
👉Toxicity manageable
🧐Not the right drug, but maybe the right target
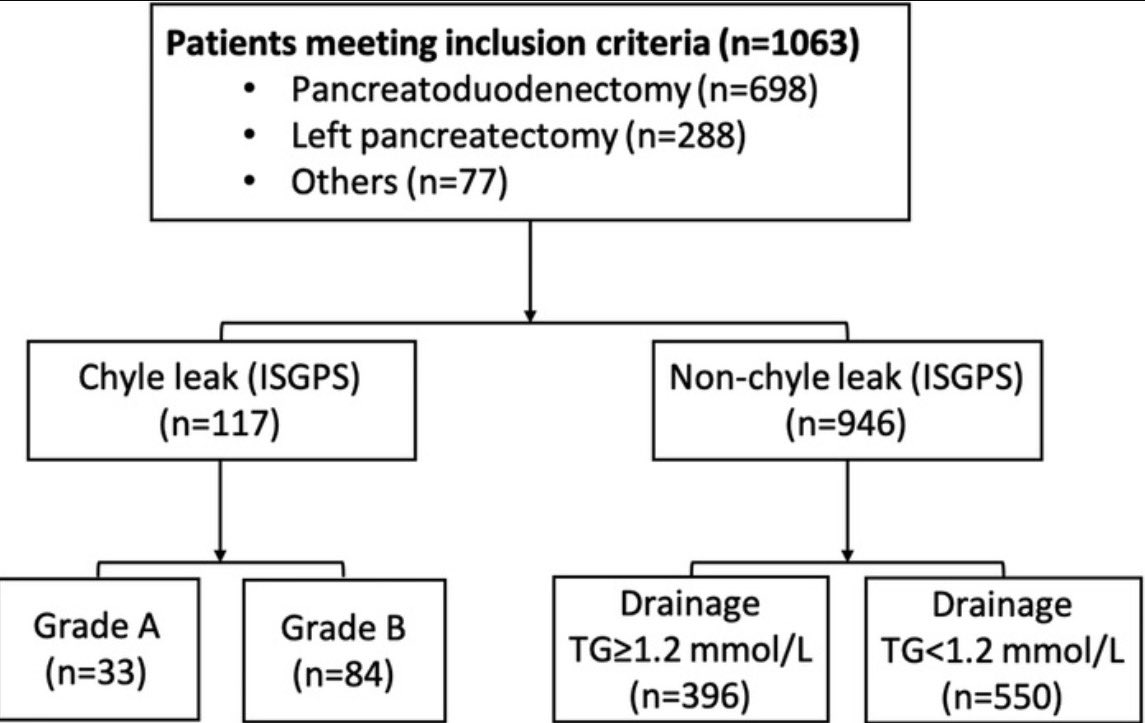
Chyle leak 🍼 after pancreas surgery is never fatal but increases in vascular dissections …
🔴 1k cases > 11% chyle leak (most grade B as per @ISGPS_news)
❌🥛 Minimally invasive approach + drain volume risk factors / Not milky appearance!
https://t.co/5t0kaAnM3z
⚡️ Histological subtypes of urothelial carcinoma — micropapillary, plasmacytoid, sarcomatoid, squamous — don't fit the one-size-fits-all treatment paradigm.
Each carries distinct biology, is often understaged on TURBT, and shows variable response to standard systemic therapy.
https://t.co/NnF32TmzJn
#BladderCancer
🆕 Drain management risk-stratified dynamic algorithm after Whipple 🆕
💦 Drain fluid amylase still key but pathways different based on intraop risk assessment
🚨 800 PD included / 32% high risk
Check out the thread 👉 practice changing algorithm
https://t.co/aqskbzXT8Y
Developing more effective therapies is critical. But just as important is to identify which pts may be cured with less chemo, an effort often only made possible thanks to philanthropy. Thanks to BCRF for supporting DAPHNe and for highlighting its results. https://t.co/nZ9GZb9Hq9