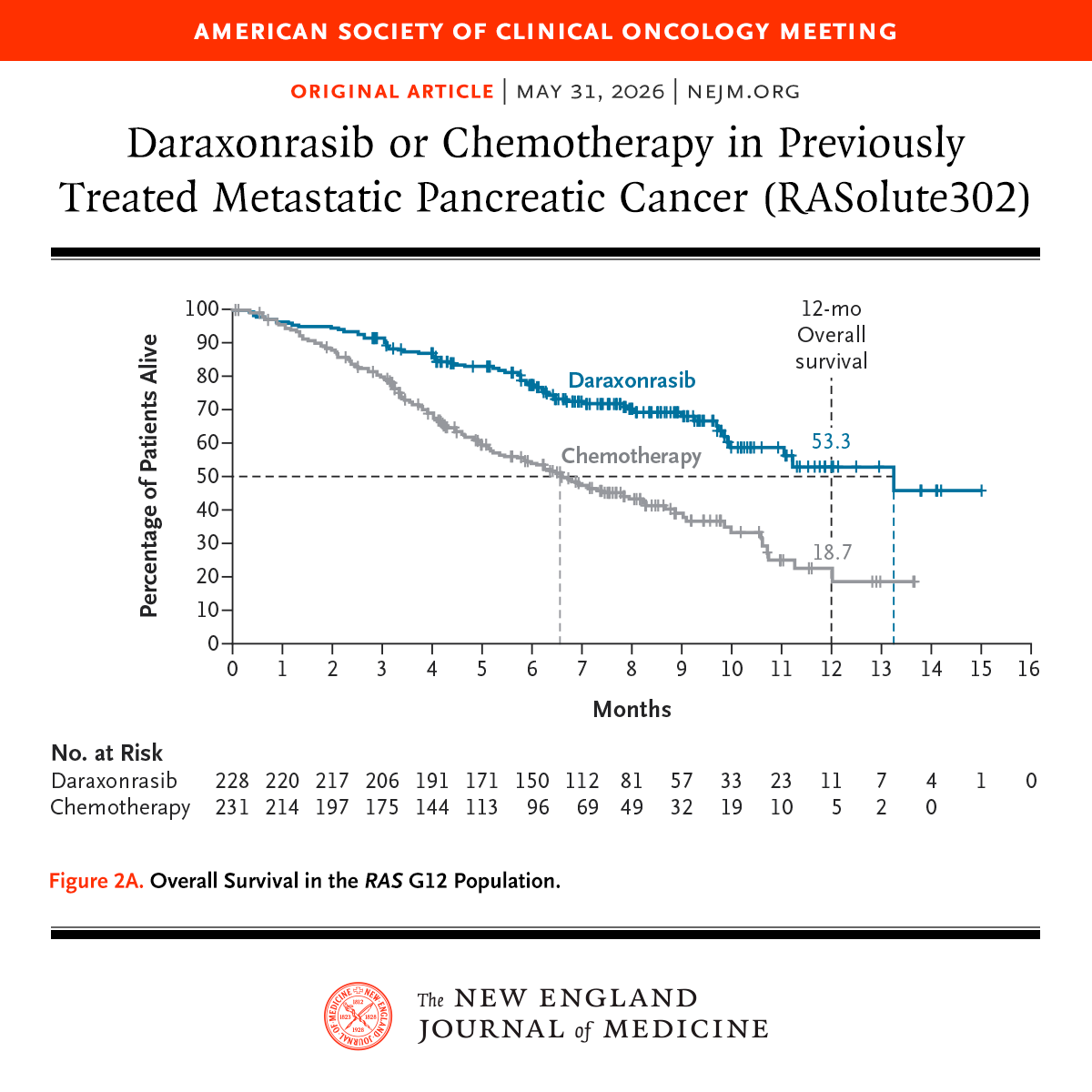
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
🔴 Balancing the benefits and risks of GLP-1 receptor agonists: aclinical guide for shared decision-making - Review (Lancet, 2026)
https://t.co/6o6CZwDLdc
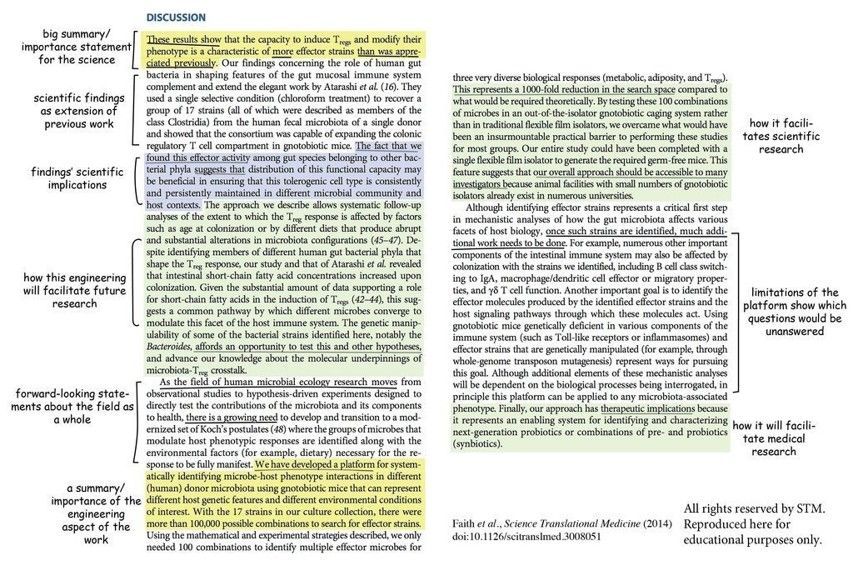
PhD Students - Here is an example of a good discussion section.
A good discussion section should answer 6 questions.
1. What is different in your findings compared to previous research?
2. What is similar in your findings compared to previous research?
3. How different sections of your results section correlate?
4. What are the implications of your findings for practitioners?
5. What are the implications of your findings for researchers?
6. What are the limitations or threats to the validity of your findings?
Anything you'd like to add?
The ramp up of cancer immunotherapy is remarkable. Now we're seeing vaccines achieve some cures or remissions in the most refractory cancers: pancreatic, melanoma, glioblastoma, renal, triple-negative breast cancer.
✓ out the new Ground Truths (link in profile)
Not every microcytic anemia is iron deficiency.
The Mentzer Index remains a useful bedside screening tool:
📌 >13 → IDA
📌 <13 → Thalassemia Trait
Clinical medicine still starts with understanding basics.
#ClinicalMedicine#Hematology#MedicalKnowledge#FOAMed
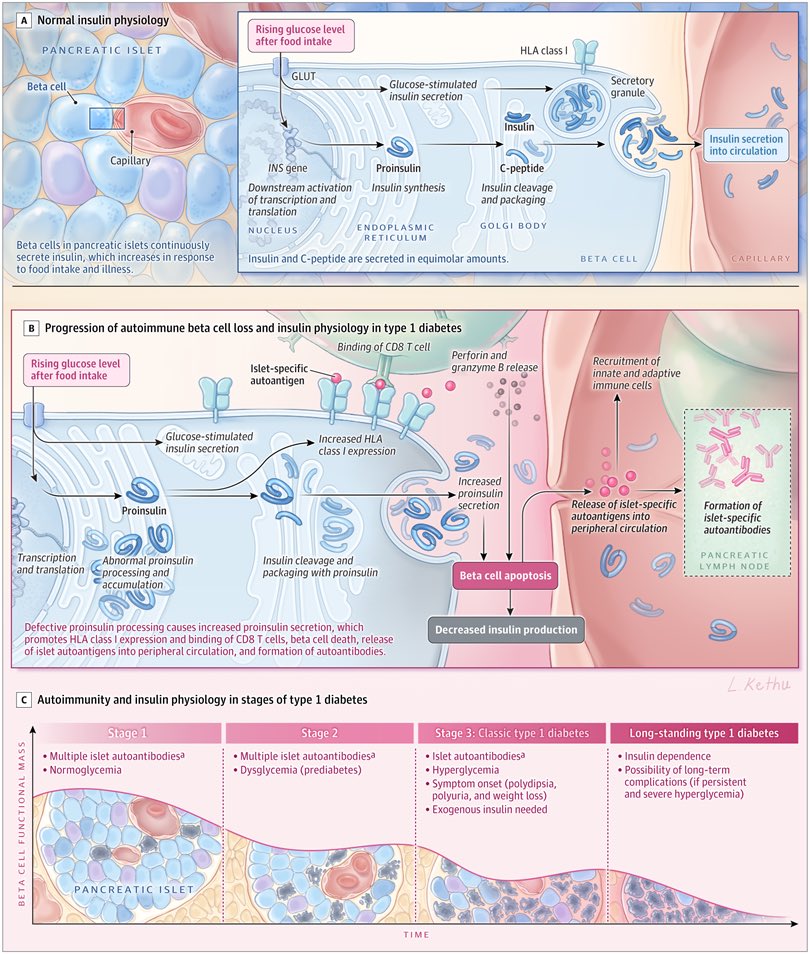
🧬 Las células delta del islote pancreático — apenas el 8% de su composición — resultan ser las que más influyen en la secreción de insulina. Y su proporción se asocia con el riesgo genético de DM2.
Un estudio en @NatureComms con 299 donantes sin diabetes sugiere que parte de nuestra predisposición genética a la DM2 podría actuar a través de estas células. La composición del islote además varía según sexo y genética. Otra pieza del puzzle de por qué la diabetes no es igual en todas las personas 🧩 🔬
📎 https://t.co/AAJqYhA4zN
¿Cuándo elegir semaglutida y cuándo tirzepatida?
La EASO acaba de actualizar su algoritmo con evidencia hasta noviembre 2025 📊 @EASOobesity
Spoiler: depende del objetivo clínico. No es solo pérdida de peso.
🔗 @NatureMedicine
https://t.co/RKkccNGYTq
#ECO2026
🩺 Obesity-related hypertension — it’s not just about weight.
In 77 patients with obesity-related HTN, dynamic hormonal phenotyping (saline suppression, ACTH stimulation, dexamethasone testing) revealed:
🔴 51.9% — Primary aldosteronism phenotype
🔵 23.4% — Renin-dependent aldosteronism
🟡 24.7% — Low-renin phenotype
⚪ 9.2% — ACTH-independent hypercortisolism
The striking finding? Over 80% had overlapping pathologic phenotypes of aldosteronism and/or hypercortisolism.
➡️ Obesity-related hypertension is far more hormonally complex than we think — and static phenotyping alone misses a large part of the picture.
Could targeted hormonal workup change how we treat these patients? 🧵
Parisien-La Salle S. et al. — JACC Basic Transl Sci. 2026;11(4):101526
#Hypertension #Obesity #Aldosteronism #Endocrinology #Cardiology #MedTwitter #CardioTwitter #JACC #Hypercortisolism #Hormones
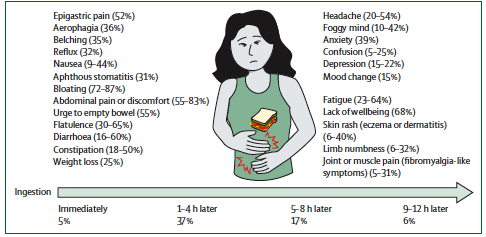
İnsanlar gerçekten glutenden dolayı mı hassasiyet yaşıyor?
Lancet dergisinde geçen sene sonu harika bir derleme makale yayınlandı bu konuda. Toplumda insanların yaklaşık %10’u “glutene hassasım” diyor ama kontrollü çalışmalarda gerçekten glutene spesifik reaksiyon verenler toplumun sadece %1,6–3,0 yani büyük çoğunluk aslında glutene değil başka şeylere tepki veriyor.
Sorun büyük ihtimalle gluten değil, FODMAP’ler (bağırsakta zor emilen ama fermente olabilen şekerler), bağırsak–beyin etkileşimi ve en önemlisi nocebo etkisi (Olumsuz beklenti nedeniyle gerçekleşen semptom).
İnsanlar gluten yediğini düşündüğü için semptom yaşıyor. Hatta bazı deneylerde insanlar gluten içermeyen yiyecekleri glutenli sanıp aynı semptomları gösteriyor.
Buna rağmen gluten-free pazarı milyarlarca dolara koşuyor ve bu algı bilimsel gerçekliğin önüne geçiyor. Ortada net bir biyobelirteç yok, mekanizma belirsiz, tanı dışlama ile konuyor ama herkes emin! Sorun glutenden kaynaklanıyor
Gerçek şu, semptomlar gerçek, ama suçlanan çoğu zaman yanlış hedef. Gluten tartışması bilimden çok algı, pazar ve psikolojinin birleşimi haline gelmiş durumda.
Meraklısı için makale:
https://t.co/TzsSOpoud8
Antibiotics to Avoid with Cheese
The Core Mechanism: Calcium Chelation
Cheese and dairy are rich in calcium (Ca²⁺), a divalent cation. Certain antibiotics form insoluble chelation complexes with Ca²⁺ and other divalent/trivalent cations like Mg²⁺, Al³⁺, and Fe²⁺/³⁺. This drastically reduces oral bioavailability and can lead to treatment failure.
1. Tetracyclines — The Classic Example
This is the most well-known and heavily tested interaction. Calcium in dairy chelates the tetracycline molecule, forming an insoluble complex that is poorly absorbed from the GI tract.
Tetracycline itself is the most severely affected, with bioavailability dropping by up to 50–80% when taken with dairy. Doxycycline is less affected (around 20–30% reduction) and is sometimes taken with food to reduce GI upset — but cheese and milk should still be avoided. Minocycline is the least affected member of the class due to its higher lipophilicity and alternative absorption pathways.
The clinical rule is straightforward: tetracyclines should be taken 1 hour before or 2 hours after any dairy product.
2. Fluoroquinolones — Second Most Important
Fluoroquinolones have a 4-oxo and carboxyl group in their structure that readily chelates divalent cations, including the calcium in cheese and dairy.
Ciprofloxacin sees a bioavailability reduction of roughly 30–36% with dairy. Norfloxacin is significantly affected as well. Levofloxacin is moderately affected. Moxifloxacin is the least impacted due to its superior baseline oral bioavailability.
The recommendation is to take fluoroquinolones 2 hours before or 6 hours after calcium-rich foods, antacids, or supplements.
3. Linezolid + Aged Cheese — A Completely Different and More Dangerous Interaction
This is not a chelation problem. This is a pharmacodynamic interaction and it can be life-threatening.
Linezolid is an oxazolidinone antibiotic that acts as a weak, reversible MAO inhibitor (MAOI). Aged cheeses — including cheddar, brie, camembert, parmesan, gruyère, stilton, and blue cheese — are rich in tyramine, a vasoactive amine produced by bacterial fermentation of tyrosine.
Under normal circumstances, MAO-A in the gut and liver rapidly breaks down dietary tyramine before it reaches systemic circulation. When MAO is inhibited by linezolid, tyramine accumulates and triggers a massive release of norepinephrine from sympathetic nerve terminals.
The result is the classic "cheese reaction" or hypertensive crisis, characterized by severe hypertension, a pounding occipital headache, diaphoresis, flushing, palpitations, and in the worst cases, intracranial hemorrhage or stroke.
This is the same reaction seen with classic psychiatric MAOIs like phenelzine and tranylcypromine. The key distinction is that with linezolid, most clinicians prescribing it for infections don't always think to warn patients about dietary tyramine — which makes this interaction especially dangerous in practice.
The highest-tyramine cheeses to specifically warn patients about are aged cheddar, stilton, gruyère, camembert, brie, and roquefort. Fresh cheeses like ricotta, cottage cheese, and cream cheese are generally low in tyramine and considered safer.
Antibiotics That Are Safe with Cheese
For completeness, beta-lactams (penicillins, cephalosporins, carbapenems), macrolides (azithromycin, clarithromycin), metronidazole, clindamycin, and trimethoprim-sulfamethoxazole have no clinically significant interaction with dairy or cheese. They can be taken with food freely.
The Core Memory Framework
There are two completely distinct mechanisms to remember here:
Chelation group → Tetracyclines and Fluoroquinolones. Calcium in cheese binds the drug and prevents absorption. The consequence is treatment failure, not toxicity.
MAOI-tyramine group → Linezolid (and classic MAOIs). Cheese doesn't reduce the drug's effect — it triggers a dangerous surge in blood pressure. The consequence here is a hypertensive crisis, not treatment failure.
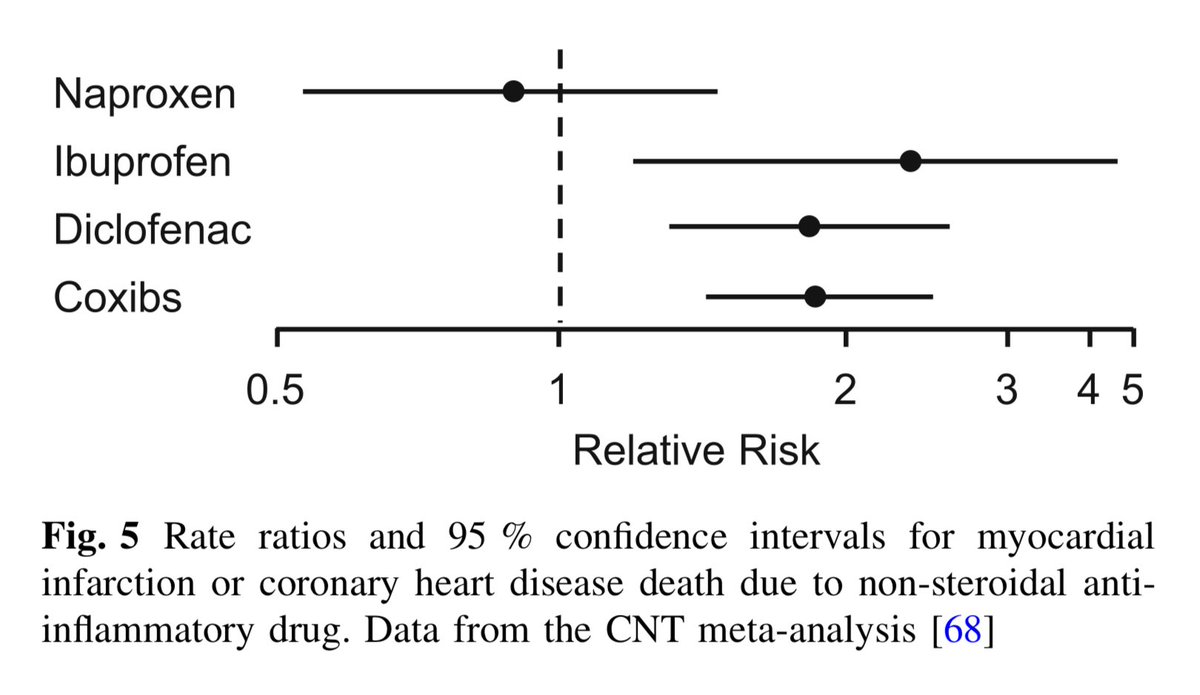
𝗡𝗮𝗽𝗿𝗼𝘅𝗲𝗻
◦ Naproxen has been consistently observed to possess a "neutral" or significantly lower risk of causing heart attacks and strokes compared to other NSAIDs such as diclofenac or ibuprofen at high doses.
◦ Several meta-analyses, including that of the CNT Collaboration (Coxib and traditional NSAID Trialists), the largest conducted to date, have concluded that naproxen does not significantly increase the risk of major vascular events or vascular death compared to placebo.
◦ While drugs such as diclofenac or coxibs (e.g., celecoxib) raise the risk of myocardial infarction by approximately 30–40%, naproxen is often associated with a relative risk close to 1.0 (placebo).
◦ Furthermore, risk may be mitigated through lower doses or shorter duration of use, such as that with over-the-counter OTC) use of naproxen.
◦ In addition to its low COX-2 selectivity (instead
demonstrating greater selectivity for COX-1
inhibition), naproxen’s greater safety is believed to be due to its long half-life and its ability to produce a sustained inhibition of platelet aggregation, similar to the effect of aspirin, when used at full doses (500 mg every 12h).