🧵 Long-term outcomes after #ECMO are lacking in the literature.
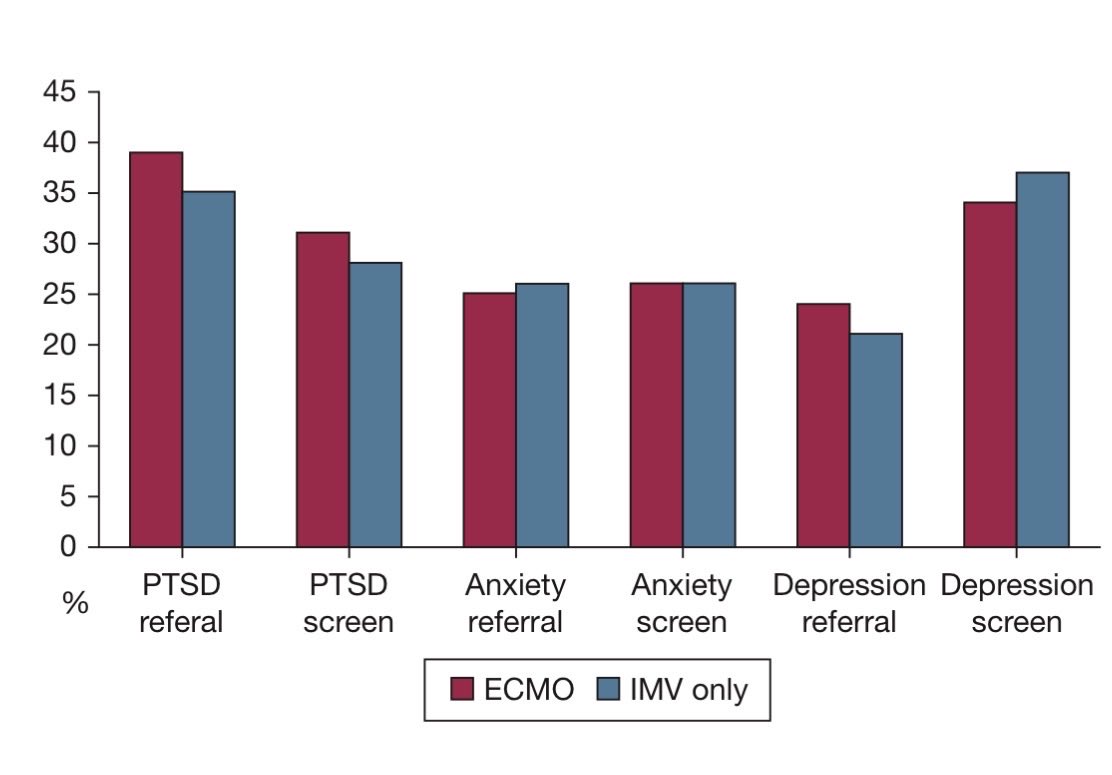
A brief thread on our new paper in @JAMA_current, looking at mental health outcomes in survivors after ECMO (OPEN ACCESS).
Thrilled to have presented the results live @ESICM#LIVES2022
https://t.co/xaqKxCky67
💙 Methylene blue in septic shock: miracle, myth… or misunderstood tool?
We all know the scenario:
👉 Refractory vasoplegic shock
👉 Escalating norepinephrine
👉 Vasopressin, steroids… still hypotensive
At some point, the question comes:
Should we use methylene blue?
⚡ Mechanism
Septic shock = NO-driven vasoplegia
Methylene blue acts by:
❌ Inhibiting nitric oxide synthase (NOS)
❌ Blocking soluble guanylate cyclase
⬇️ Reducing cGMP
➡️ Restoring vascular tone
👉 A true catecholamine-sparing strategy
📊 What does the evidence say?
Reality check:
Use in practice is rare (~0.5% of septic shock patients)
Often used as late salvage therapy
Dosing strategies = highly variable
But RCT signals are interesting:
↓ Vasopressor duration
↓ ICU / hospital length of stay
Possible ↓ mortality (low certainty)
👉 Evidence is promising… but still weak
🚨 The clinical dilemma
Timing is everything:
Early use → potential physiologic benefit
Late use → often too late to change trajectory
👉 Current practice is probably backwards
⚠️ What about safety?
Potential concerns:
Serotonin syndrome (with SSRIs)
Pulmonary vasoconstriction
G6PD-related hemolysis
Interference with pulse oximetry
👉 Most serious effects seen with high doses
🧠 Take-home message
> Methylene blue is not a “magic drug”
but it may be a physiology-driven adjunct in vasoplegic shock
❓The real questions are:
Who benefits?
When to give it?
At what dose?
🚀 Where we’re heading
Ongoing trials (e.g., BLUSH trial) will clarify:
✔️ Early vs late use
✔️ Optimal dosing strategy
✔️ True impact on mortality
👉 This could redefine vasoplegic shock management
💡 Clinical reflection
Next time you face refractory shock, ask:
👉 Is this still “fluid + catecholamine problem”…
👉 or already a NO-mediated vasoplegia problem?
📚 Reference
Fernando, S. https://t.co/ncF980VW9A al. Journal of Critical Care, 92, 155353.
https://t.co/df2IPfq0QS
⚙️ Curious re the long term outcomes of ECMO & iMV? 🫁
👀 Check out N Jawa & @shanfernands’s new 🌟editorial🌟 on L Rose et al’s study in #journal_CHESTCritCare:
Ed: https://t.co/Qs4iCouIcI
Art: https://t.co/yZWc5OKwrL
We're expanding our group! If you want to work with an amazing team in a terrific city, please consider applying! Please share widely.
https://t.co/jJ17fmRglw
It is so painful to share the news of @FralickMike sudden and unexpected passing 💔
Mike was an amazing, inspiring and generous person who touched the lives of many.
As we mourn, please share and consider supporting his wife and 2-year-old daughter. https://t.co/uErWWCFPde
Another output from superstar fellow @JungRichardG - Prognostic factors associated with mortality in septic shock: a systematic review and meta-analysis - out in @LancetRespirMed
Downloadable: https://t.co/JJ3Yzm3Sqc
Kudos to @SameerKadri12 for the accompanying editorial.
In fields like cardiogenic (https://t.co/Qm5v2D2ucM) and septic shock we generate large amounts of prognostic data that live individually in studies published across time, journals etc. These findings have important implications for clinical and research applications but it can be difficult to understand these factors comparatively.
In our publication, we boiled the data down to 95 eligible studies that included 4.8 million eligible patients. We divided the analysis into patient, presentation factors and biochemical markers as they related to in-hospital or 30-d mortality.
Significant patient factors included black race, history of cirrhosis or malignancy.
Significant presentation risk factors included respiratory source, AKD or elevated risk score (SOFA>APACHE>SAPSII)
Significant treatment/biochemical risk factors included need for NE or mechanical ventilation.
The identification of these prognostic factors could aid in clinical risk application, goals of care discussions, and identifying the subset of patients at highest and lowest risk of early mortality for patients with septic shock.
Kudos to co-authors and collaborators @shanfernands@rebeccamathewmd@Bram_Rochwerg@PietroDiSantoMD@PietroDiSantoMD@GProsperiPorta@cameron_stotts
#SEPSIS #SpesisAwareness #StopSepsis #critcare #criticalcare #ICU #CICU @MayoClinicCV@mayoclinicCCM@MayoPCCM@MayoCCJC@UOHI
Kudos to the author team including lead author @shanfernands from our @LakeridgeHealth@queensccm Critical Care faculty! Looking forward to the eventual results of the BLUSH trial underway to provide the randomized evidence needed to evaluate methylene blue in septic shock.
🔍 Methylene blue (MB) use is uncommon in septic shock, with substantial variability across time, patient populations, and hospitals. Randomized evidence is required to evaluate the efficacy and safety of MB.
📖 Read more in CCM: https://t.co/H7OCGpcgKg
#CritCareMed#SCCM@SCCM
Proud that @LakeridgeHealth has recruited its first patient into the @AlterAKItrial! An RCT designed to test the efficacy of albumin infusion during dialysis in critically ill adults.
We are excited to contribute to this important RCT!
@edclark75@CCCTG_@cmcpher@drrandywax
We just published in @ResusJournal a meta-analysis of MCS after ROSC
While only 1 RCT addressed this topic only in CA pts, most RCTs of MCS in AMI-CS enrolled a high proportion of post-CA pts
We pooled data from RCTs with available CA subgroups.
https://t.co/YdSwfbcknz
1/
🚨📣 A long-awaited study from my #BantingCanada fellowship examining predictors of recurrent #VTE and anticoagulant-related🩸 #bleeding in patients with cancer was published in #EHJ today to coincide with my live presentation at #ISTH2025‼️
https://t.co/QZnSMisHwU