I was skeptical of virtual twin studies but @fdossa convinced me they have a role, especially for our patients with rare cancer. Look forward to seeing what’s next out of this line of research #ASCO26#sarcoma 👇🏻
SARC041: confirms clinical activity of abemaciclib for pts with advanced dediff liposarcoma ✅
👏🏽 to Mark Dickson @MSKSarcoma on this work and Paolo Casali @casali_pg@IstTumori for an excellent discussion
Open❔role in resectable disease
#ASCO26
This is a great read on watch & wait in rectal cancer.
B/c patients with local regrowth after WW have higher rates of distant mets, there has been an intuitive fear that regrowth is causal (i.e delaying TME permits metastatic seeding hence WW risky).
The authors here argue (and I agree) that regrowth/metastases are manifestations of intrinsic aggressive tumor biology because:
1) no difference in time to surgery in patients w pCR/regrowth who developed mets vs. those who didn't (if delay were causal, would expect longer delay in patients who developed M1).
2) in OPRA secondary analysis, patients with cCR underwent least surgery/longest observation while those with incomplete response had surgery most frequently/immediately. But outcomes still tracked with response phenotype not timing of surgery (i.e. cCR did best).
3) tumor response itself is prognostic (i.e. even when all pts undergo TME, more regression after neoadjuvant therapy --> better DFS/DM).
4) modern tumor evolution data suggest metastatic spread mostly happens early.
5) chemo/radioresistance appears to be linked to metastatic potential (i.e. regrowth is a marker of aggressive biology not the mechanism itself).
IMO a persuasive argument against hypothesis that regrowth seeds metastasis, but rather biology=dominant driver. @OncoAlert
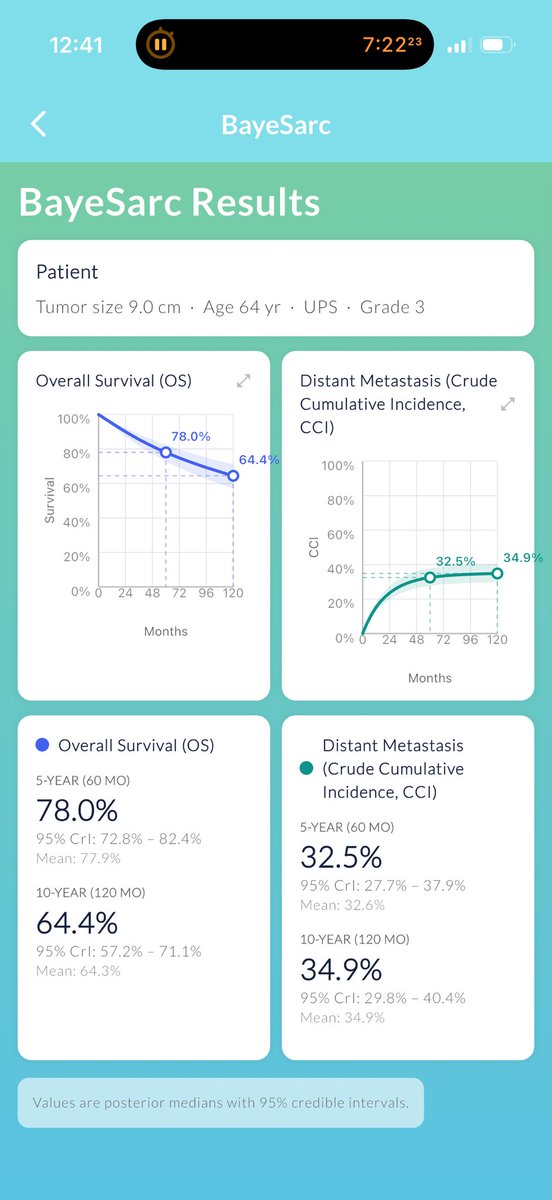
Thrilled to finally see this out - 🚨#Sarculator bayesian update for more refined risk estimates in extremity soft tissue sarcoma
App📱update and @LancetOncology pub: https://t.co/MU01O5h5ca
Phenomenal work @DCalleMD, Gabriele Tine, et al. ! 👏🏽👏🏽
The #Sarculator app update is now live!
This comes together with our @TheLancetOncol paper introducing #BayeSarc, a Bayesian sequential learning approach to refine prognostication in extremity soft tissue #sarcoma.
Paper: https://t.co/gQuFERjCqu App: https://t.co/4mLSfv7zE3
With ⤴️use of W&W for rectal cancer, how can we safely 🫸the limits? Is there a role for W&W in pts with *near* complete response or does this risk distant disease?
More on the📊 and our recommendations for safe W&W practices: https://t.co/SrxoUVZFcQ
@JCO_ASCO @DrGarciaAguilar
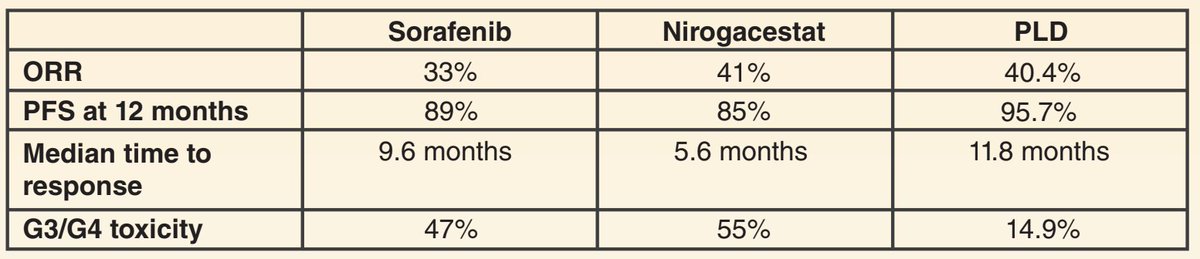
@HannahRAbrams Thanks for highlighting! This is probably clearer in the paper but we purposely framed all outcomes such that further from center = better (eg tolerability rather than toxicity)
So niro had ⬆️toxicity (incl ovarian suppression) but most rapid effect💨(?differences in study pops)
New RCT data 📈 supporting the efficacy of Doxil for progressing desmoid tumors. Now 3 options supported by level 1 data - but how to choose? 🧐
👀 editorial in @CCR_AACR with @SilviaStacchia and @alegronchi
https://t.co/pDLiZK0fX7
Celebrating @seacm on receiving the AHPBA Research Development Grant. This is the impact we strive for: advancing science, elevating care and leading the way.
https://t.co/ZPkzAodCsP
ctDNA🩸: game-changer or expensive crystal ball?🔮
💡What surgeons should do with ctDNA in CRC, gastric & cholangiocarcinoma at #SSO2026 with @ColinCourtMD@fdossa@FlavioRochaMD & wrap-up by @rachnatshroff
Join us in Phoenix👉🏻 https://t.co/i6a9aJgivX