A surprising but heartening finding. Importantly, trust has dropped amongst specific groups - as scientists and physicians, it is our responsibility that we not give up on those groups but continue to consistently build trust and relationships that support the health of all.
Well-timed with the explosion of AI in biomedicine. Developing new methods with truly diverse datasets ensures findings apply to patients everywhere.
But as always, one database will not be the ultimate solution: positive AND negative ethical implications abound!
Breaking News: A research program at the National Institutes of Health released the world’s largest database of human genomes, officials said, paving the way for a new era of study in personalized medicine.
https://t.co/N29D0YhJVp
“This is a structural problem that reinforces dependency on high resource settings and limits autonomy for researchers in lower income settings. This creates a cycle in which capability is never fully built and global research remains unevenly distributed.”
“Power, authorship, and recognition concentrate around those who control the data… rather than the researchers who collect and best understand the context of the data…
[but] researchers closest to the data are best placed to ask meaningful, contextually grounded questions.”
Progress around data sharing has improved access, but not equity.
Data sharing must evolve towards data sovereignty, writes Trudie Lang
https://t.co/SPpKPEWfcT
Chatbots are machines optimized for our pleasure, not our improvement. A trained therapist knows when to support and when to push back for growth; a chatbot is trained to make you come back no matter what.
People are increasingly turning to AI for mental health support—but its design is “antithetical” to mental health care, experts say
https://t.co/BLpWmrWuCB
The intentional anthropomorphization of AI is dangerous. For better or worse, a day may come when AI is capable of replacing human interaction - but we aren't there yet. Sycophantic models trick users into thinking we are, substituting humanity for (inaccurate) simulated empathy.
When my doctor offered genetic testing based on my family's cancer history, I was on the patient side of the predictive genomics I study. I faced the dilemma of uncertainty: as a future physician, I know the best support I can offer is a clear breakdown of the risks and benefits.
Nancy Wexler's work is a beautiful example of how involving patients early in a scientific journey ensures the questions we ask produce answers they actually want to know. In doing so, her science generated autonomy for patients who felt they had none. https://t.co/bNCBlu457E
Katerina's anorexia hospitalized her over & over. Even still, eventually, she found a way thru.
Then, insurance cut her off.
Ppl w/severe mental illness are frequently denied life-saving care. That's dangerous. It also may be illegal.
Via @rollingstone
https://t.co/Pu6kX8xtQX
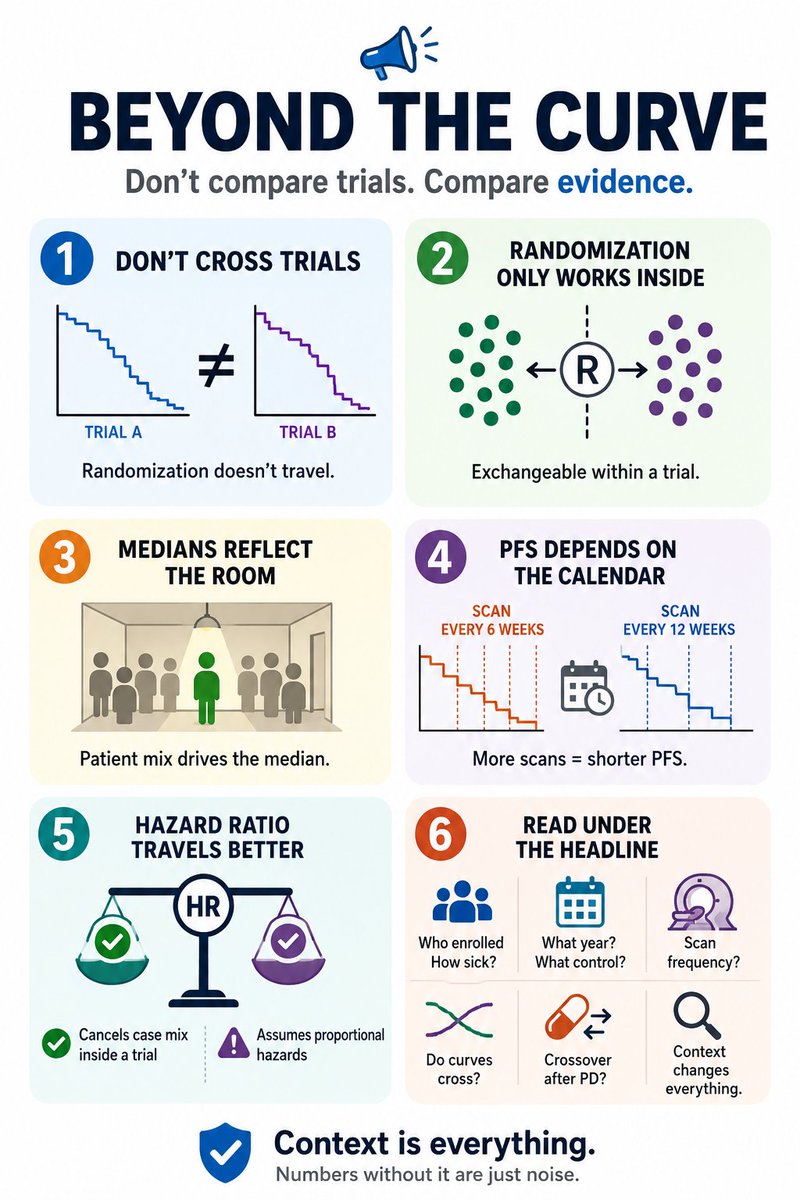
1/ #ASCO26 starts tomorrow. By Friday your feed will be full of survival curves, and the temptation will be everywhere: cross-trial/study comparison.
Before you do so, A few caveats worth keeping in mind
"The erosion of creative thinking means young people will struggle to navigate uncertainty." AI can only iterate on what it has seen before- but "our species’ ability to come up with unexpected and original ideas is something to protect and nurture." https://t.co/6AUb9MECNR
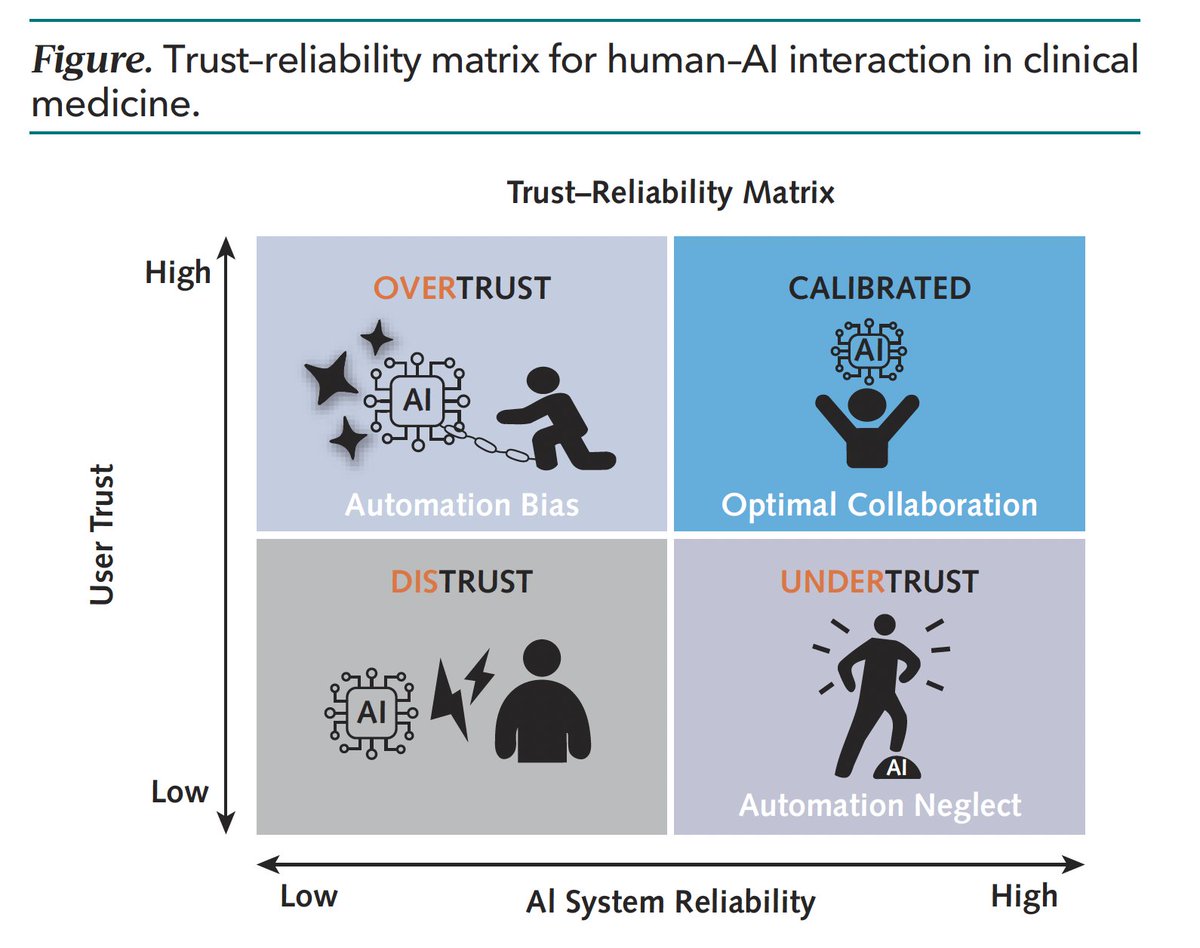
Ignoring AI in medicine would be naïve; implicit trust in all its decisions would be arrogant. As with most clinical practice, balance and healthy skepticism is critical. Future physicians need to be taught not just how to use AI but how and when to question it.
New @AnnalsofIM
"The Human Factor in Clinical AI: Why Technology Alone is Not Enough"
Gets into the trust issue and concludes: 'The most important question in medical AI may not be “how accurate is the algorithm?” but rather “how do we calibrate the relationship between clinician and machine?'
https://t.co/n4ijxrm7o9
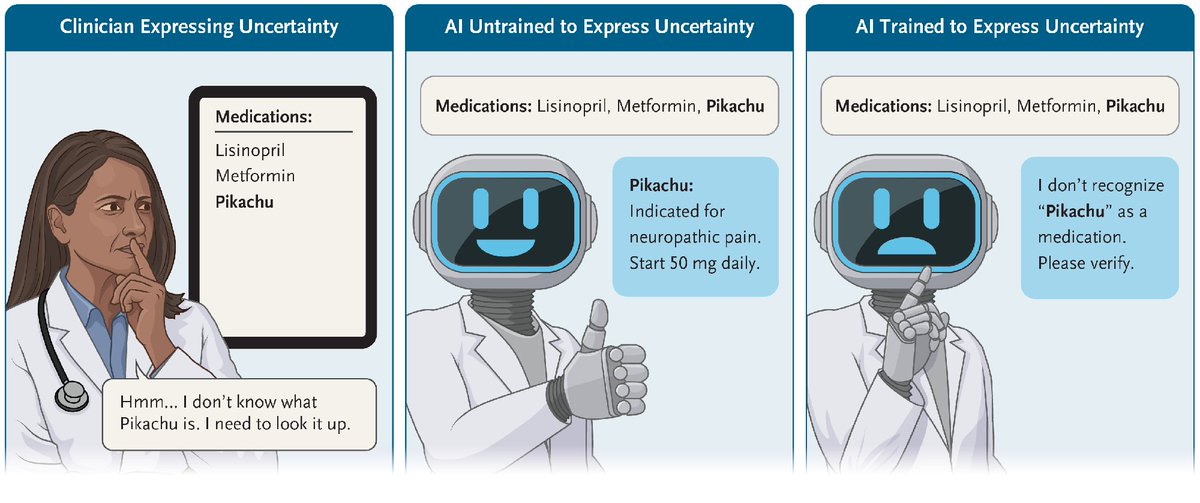
From my perspective there are (at least) two critical things missing from AI that hinder its ability to do clinical medicine: humility and doubt. Ironically, those are the two skills I seem to be constantly reinforcing in medical school…
The authors of a new Perspective argue that clinicians are rightly expected to disclose their gaps in knowledge or their inability to forecast an outcome. Yet emerging AI tools often cannot, or will not, do the same.
Read the Perspective by @AndreaSikora, PharmD, MSCR, Leo A. Celi, MD, MPH, and Raja-Elie E. Abdulnour, MD (@BageLeMage): https://t.co/4l8tHUmkOx
"My mental health struggles have forced me to check in with myself, respect my limits, and make space for emotion in an environment that treats it as a liability." #MentalHealthAwarenessMonth https://t.co/Da1Gdnm9eP
I learned so much during my time in the @FulbrightPrgrm in Heidelberg, Germany with @embl. Excited to be a co-first author on this manuscript coming out in print soon!
Integrative spatial and multi-omic profiling in bladder cancer links L1 retrotransposition to extrachromosomal DNA, genomic ... https://t.co/2VaS1aoP0N #biorxiv_cancer
Experts reach consensus to rename polycystic ovary syndrome (PCOS), better reflecting the condition’s full health impacts.
Find out more 👉 https://t.co/Azue7YDFcn @ESEndocrinology#ECE2026