@DrPlantel@AmDiabetesAssn " These attendees were escorted out by our onsite event security because they demonstrated behavior not consistent with this code of conduct." @AmDiabetesAssn can you explain why handing out flyers is against the code of conduct?
Blandine Laferrère with an excellent review of different methods of diagnosing obesity, including the limits of BMI and a review of @TheLancetEndo guidelines in which she participated.
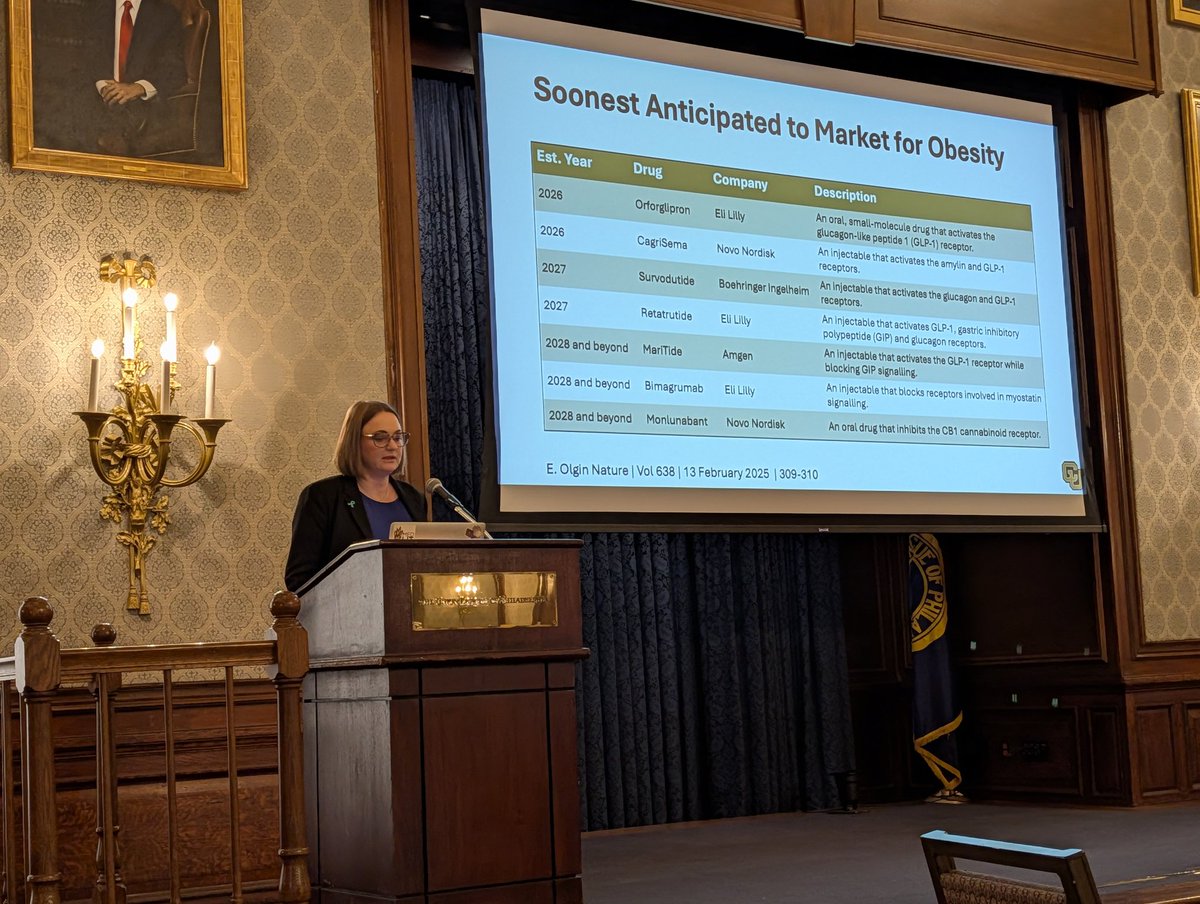
@LoewenthalMd One of the weaker agents in the class, too! Will be so interesting to see how widespread GLP-1 receptor effects may be outside of what we initially thought.
@thecurbsiders Great episode! For diagnostics, I'll add that many hospitals are using newer higher-sensitivity cortisol assays and the cutoffs for 'normal' cosyntopin stims are changing: https://t.co/Qll5TGIjis
@Dr_Oubre There's a concept in golf that you fix two divot marks on the putting green - one you made when your ball landed and another someone else never fixed.
The same logic applies to the problem list - clean up your diagnoses that are no longer relevant and that others left behind!
I'm just a physician, again asking a major television show @succession@HBO to please just properly depict good CPR technique. Proper depth of compressions and switching off every 2 minutes are so important - don't mislead the audience otherwise!
I understand it's not the most realistic show in the world but the CPR scene in @obxnetflix is so unfortunate. It's easy for the public to misunderstand the basics when they see such poor compressions on TV. 2" deep while humming "Stayin' Alive," everyone!
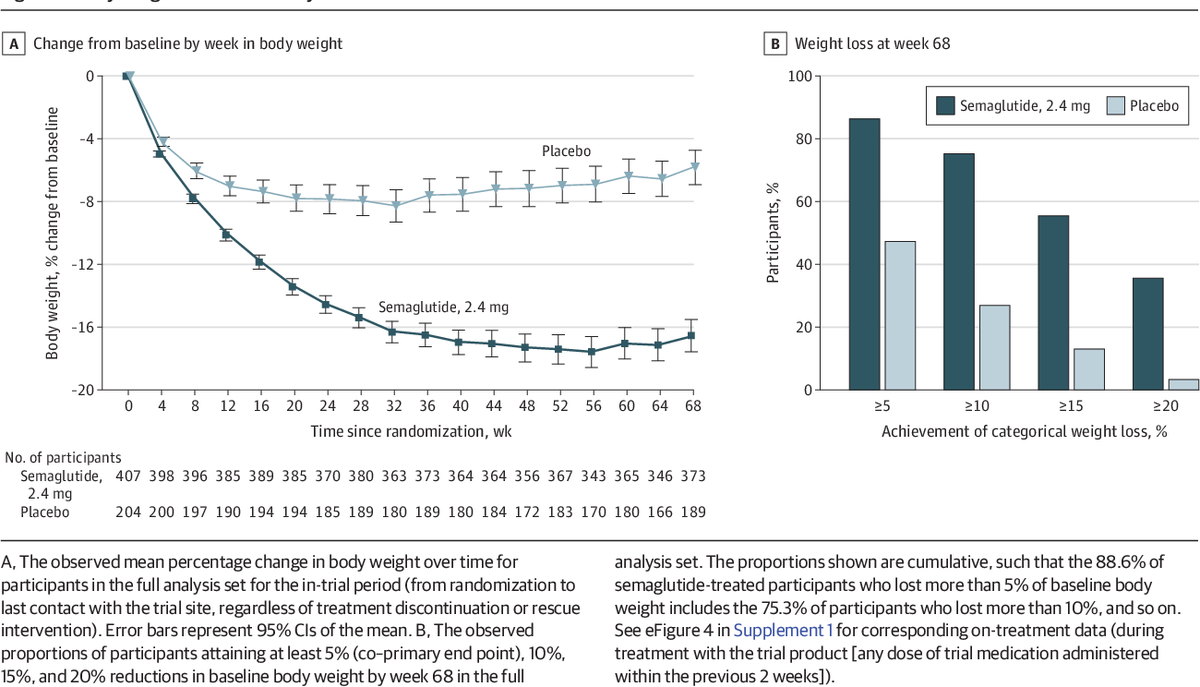
@DanielJDrucker Excellent graph. This is what I review with all patients newly starting therapy. Aside from medico-legal fears, is there then any reason to avoid offering GLP-1A therapy to patients with a history of chronic pancreatitis?
@DudzLightLime@BevTchangMD@Bianco_Lab He is certainly a proponent for the increased utilization of T3 in primary hypothyroidism but these labs are not consistent with hypothyroidism. He wouldn't use your regimen for this patient.
@BevTchangMD Yeah... Definitely did the math wrong there 😉 I see new TSH suppression frequently but always assumed it was the weight loss. Good to know it may occur independent of that!
@HadleyFreeman Look at these results. The placebo group received weekly counseling related to weight loss. But you think it's 'surreal' and 'myopic' to recommend a therapy that was so much more effective?
@HadleyFreeman I'm sorry you struggled with anorexia and I'm glad you are better. But to say the root cause of obesity is 'emotional' ignores the extensive data showing aberrations in hunger signaling for many patients. To deem the use of GLP-1As like semaglutide as 'self-harm' is ridiculous.
@BrownJHM@InternAtWork Nice overview. Patients should aim for moderate calcium intake (800-1000 mg elemental) and enough vitamin D supplementation to maintain normal (>30) levels - low Ca intake + 25-OH insufficiency can both worsen PTH secretion!
@WilliamAird4 Do you think similarly for the opposite problem of erythrocytosis/polycythemia? Endocrine Society guidelines emphasize monitoring Hct, not Hgb, in testosterone replacement - are there any drawbacks to this approach?
@tmodarressi@AnandVaidya17 The main concept I'm struggling with is why the discordance between plasma and urine aldo levels can be so vast. Eg, a patient with PRA <1 and aldo in high teens had a UrAldo of ~4-5 despite low UrNa on collection. Seems too large a discrepancy?
@tmodarressi@AnandVaidya17 I'm seeing the same issue in workups. I think the Umakoshi paper used captopril challenge as gold standard for diagnosis, so maybe their flaw was assuming 100% sensitivity for this test? I'm not sure how PRA <1 and aldo >20 could really be anything but hyperaldosteronism.