Targeting vaccine fusion proteins to APCs increases immunogenicity of adenoviral and mRNA-LNP vaccines https://t.co/gUhCwajWTc #genetherapy#celltherapy
Since the 1960s, the genetic code has been used to predict protein sequences from DNA and mRNA sequences. Our @Nature article demonstrates that these predictions miss thousands of protein sequences present in human tissues.
Across >1,000 human samples, we identified numerous abundant proteins whose amino acid sequences differ from those predicted by the genetic code.
These proteins are not rare translation byproducts. They accumulate to thousands of copies per cell. Some are more abundant than the proteins predicted by the genetic code from the same transcripts.
Their abundance reflects a combination of alternate RNA decoding mechanisms — including codon-anticodon mismatches, tRNA abundance, and RNA modifications — and selective stabilization of the resulting proteins. The last factor – protein stability – emerges as a major determinant of protein abundance across proteins, proteoforms and cell types: https://t.co/IzOfAZKnxT
Alternate RNA decoding is pervasive across functional groups of proteins, healthy and diseased tissues. It affects proteins playing key roles in neurodegeneration, and some alternately decoded proteins show strong enrichment in tumors compared to their surrounding tissues.
This discovery has been a long and exhilarating journey with Shira Tsour and the @slavovLab team. It started in 2019 and proceeded through many challenges and thrilling highs. A journey that has opened new perspectives that we long to explore!
1/
A new Science #Immunology study shows that PD-L1 blockade can inhibit MHC-I presentation on tumor cells, enabling immune evasion and #metastasis in mouse models of #pancreatic cancer. @IngunnStromnes https://t.co/CGeW2vgG1K
In Brief: The most advanced clinical trial for an in vivo gene editor, @intelliatx's lonvoguran ziclumeran (lonvo-z), reported positive phase 3 results in hereditary angioedema https://t.co/T49Hx59Eaz
Today we all lost our jobs.....
Three Nature papers showing that scientists in the conventional sense are obsolete
At least read the first one.... the AI replaced all things that the scientist does ....
https://t.co/zMsRLaaRDU
Cancer survival in the U.S. just crossed 70%.
It was 63% in the 1990s.
That gap = 4.8M people alive today.
This one chart captures survival gains across 29 cancer types.
The wins are real.
So is the unfinished work.
▪️CML: 31% → 72%
▪️Multiple myeloma: 32% → 62%
▫️Kidney: 59% → 82%
▫️Metastatic melanoma: 16% → 35%
▫️Childhood ALL: 80% → 92%
But some cancers barely moved.
Cervical cancer outcomes actually worsened.
None of this is abstract progress, though.
These are birthdays, grandkids, and years of life returned.
This is what funded science does.
Next time someone asks if cancer research works, show them this (full) chart.
- - - - -
Source: ACS Cancer Statistics 2026 · SEER · 𝘷𝘪𝘢 @Jori_health
- - - - -
Across recent evidence, GLP-1 receptor agonists look like multi-organ metabolic therapies—not just glucose drugs—with real benefits and real safety and durability trade-offs. 🧵 1/7
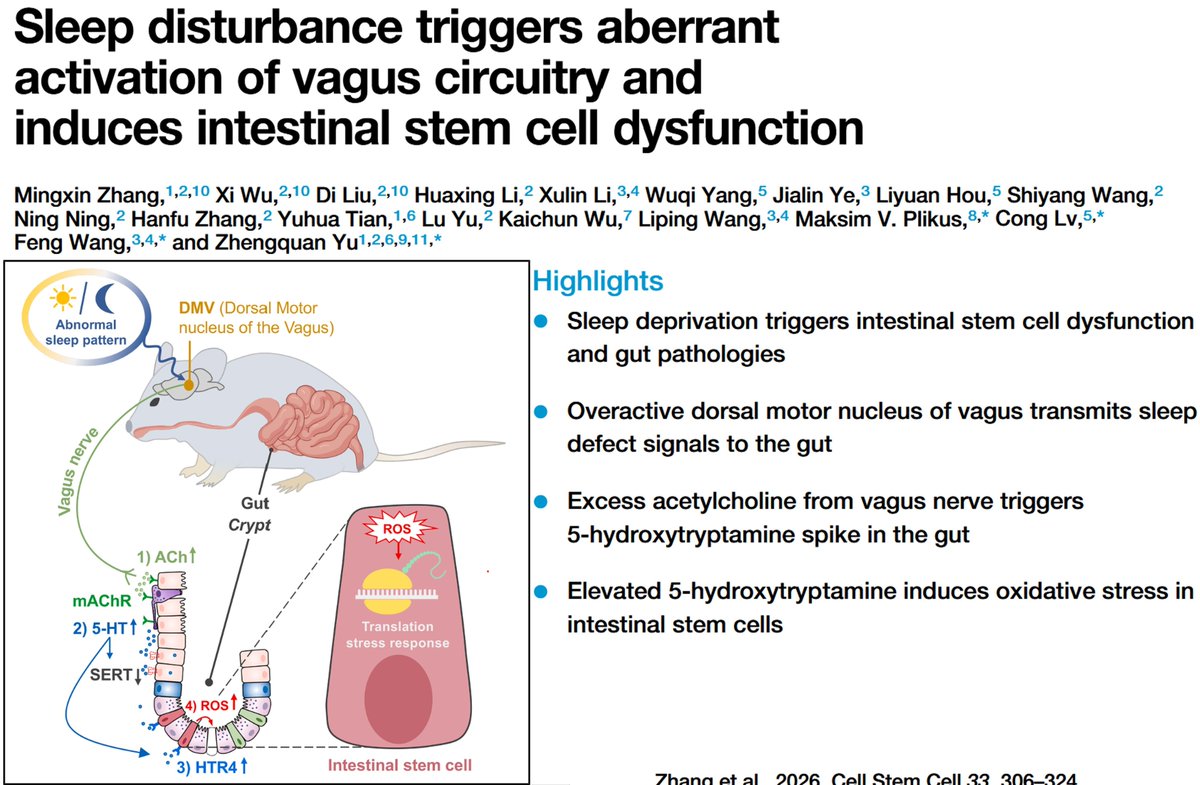
Sleep loss doesn’t just affect the brain—it disrupts the gut 🧠➡️🦠
Overactive vagus signaling boosts acetylcholine & serotonin in the intestine, driving oxidative stress and impairing stem cell function. Another reason sleep is critical for whole-body health. #SleepScience #GutHealth
https://t.co/gcqACD9LWM
Short sleep ages you. Long sleep usually means something is already aging you.
A new paper in Nature this week mapped sleep duration against biological aging across 9 organ systems in half a million UK Biobank adults aged 37 to 84. Junhao Wen's lab at Columbia used 23 different aging clocks built from MRI scans, plasma proteins, and metabolites. The relationship is U-shaped. The slowest measured aging sat between 6.4 and 7.8 hours per night. Outside that window in either direction, organs looked older than chronological age would predict.
The two arms of the U are not the same biology.
On the short-sleep side, the causal story is well established. Sleeping under 6 hours raises systemic inflammation, impairs next-morning glucose tolerance, suppresses NK cell activity, and tracks with markers of poorer overnight brain waste clearance. Mendelian randomization in this paper supports a direct causal effect of short sleep on aging biology. Short sleep drives the wear and tear.
On the long-sleep side, the picture flips. Consistently sleeping over 8 or 9 hours is a well-documented marker of underlying disease, not a damaging behavior in itself. It tracks with major depression, undiagnosed sleep apnea, hypothyroidism, chronic inflammation, and neurodegenerative disease. The authors note that Mendelian randomization could not strongly support reverse causality, but they explicitly could not exclude it either. Decades of sleep medicine argue that for most long sleepers, the long sleep is the body compensating for something already wrong.
This matters because the practical advice for the two groups is opposite.
If you sleep under 6 hours, the levers are direct. Total sleep opportunity. Consistent timing. Morning light. Caffeine cutoff after lunch. Alcohol stopped at least three hours before bed. Sleep extension trials adding 45 to 90 minutes a night have shown measurable improvements in metabolic and cardiovascular markers.
If you consistently sleep 9 or more hours and still wake unrefreshed, the right move is to investigate what your body is recovering from. Home sleep study to rule out apnea. TSH, free T4, ferritin, CRP, vitamin D, B12. Depression and anxiety screening. A review of medications that increase sleep need.
One scenario gets lumped in with long sleepers that shouldn't be. Athletes in heavy training blocks, adolescents, people recovering from infection, and people in their first trimester genuinely need 9 to 10 hours. The paper looked at habitual sleep in adults aged 37 to 84, not acute recovery states. The curve does not apply to them the same way.
The cleaner way to state the finding: there is a window in the middle where the body looks youngest on every clock the authors built. Both sides of that window correlate with faster organ aging. The reasons differ. Short sleep does the damage. Long sleep usually shows the damage is already underway.
Four trials at AACR 2026. Four approaches. One question: what if you treated cancer before it fully forms?
NEOPRISM-CRC gave 32 colorectal cancer patients 9 weeks of immunotherapy before surgery. 59% had no cancer left. At 33 months, zero relapses.
CAR-PRISM gave 20 patients with smoldering myeloma (a precancer, no symptoms yet) CAR-T cells. 100% went MRD-negative. Zero progressions at 15 months.
A BMS team injected checkpoint inhibitors directly into precancerous lesions. 82% cancer-free at 12 months.
A late-breaking study eliminated KRAS-driven precancerous pancreatic cells before they formed a tumor.
Four groups. Immunotherapy, cell therapy, direct injection, molecular targeting. All pointed upstream of the tumor itself.
Oncology has spent decades perfecting what to do after diagnosis. These trials ask: what if diagnosis is too late to intervene?
Small trials (20-32 patients), short follow-up (15-33 months). But zero relapses and zero progressions across two independent studies is not noise.
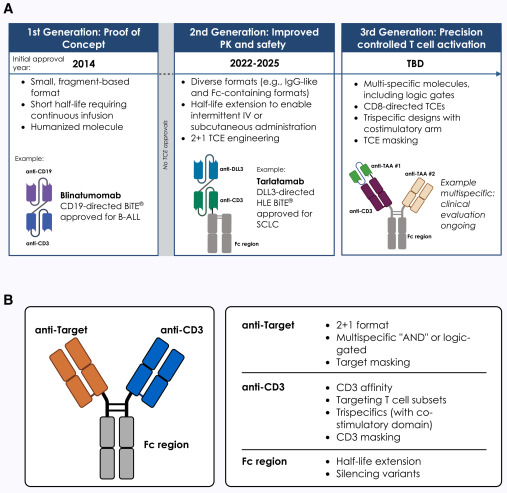
ADCs may already be changing oncology more than we realize.
Navigating the clinical progress of ADCs in @CellPressNews
The biggest shift 🚀
High antigen expression may no longer be necessary for benefit.
HER2-low changed the field
TROP2 may change it again
https://t.co/jMXeQ7i712
A single injection just replaced a $1 million procedure.
Traditional CAR-T therapy costs over $1 million and takes weeks. Doctors extract your T-cells, re-engineer them in a lab to recognize cancer, then reinfuse them.
Researchers are now doing the same thing with a single injection.
It's called in vivo CAR-T. Lipid nanoparticles carry genetic instructions directly into your bloodstream.
They find your T-cells, fuse with them, and deliver the gene for a cancer-targeting receptor.
The T-cells build the receptor themselves. No extraction. No bioreactor. No weeks of waiting.
The platform is already in clinical trials targeting blood cancers including B-cell lymphoma and leukemia.
The same lipid nanoparticle technology that delivered COVID mRNA vaccines is now being used to reprogram your immune system to hunt cancer.
Engineered cellular immunotherapy shows great potential for treating autoimmune diseases. Payne and colleagues review emerging clinical data of the most recently developed technologies https://t.co/GmoJGW5d8j
https://t.co/g53ng3bwCZ
Today we announced that the first participants in the U.S. and UK have been dosed in a Phase 3 study of our investigational mRNA-based H5 pandemic influenza vaccine candidate, mRNA-1018. In December 2025, @CEPIvaccines and Moderna announced that CEPI will invest up to $54.3 million to help advance mRNA-1018 to licensure.
Read more: https://t.co/5PP4YTYaIf
The 2026 "Cancer Hallmarks" update shows that tumor metabolism is the central node connecting the whole body. From brain signals to gut bacteria, metabolic reprogramming drives how tumors grow and resist treatment
https://t.co/KbbhCCk11R
via @imedverse