The biggest cancer meeting of the year just ended. The headline most people missed: some of the strongest results cost almost nothing.
4 wins from ASCO 2026, cheapest first:
1️⃣ Exercise, basically free. A structured program after colon cancer cut the risk of death 37%. Survival at 8 years: 90% vs 83% for usual care. The health economists ran the numbers and called it “dominant,” meaning it cost the system less AND people lived longer. They almost never get to use that word.
2️⃣ Low-dose immunotherapy, about $230 a month. A Mumbai hospital gave one tenth the usual dose of a checkpoint drug plus three generic pills. In head and neck cancer it beat standard chemo: 10.3 months of survival vs 6.2. Same class of drug that costs tens of thousands elsewhere.
3️⃣ The gentler prostate pill, same price as the harsh one. Two standard drugs control the cancer about equally. One (darolutamide) caused half the brain fog of the other (enzalutamide). Costs the same. The cheaper “win” here is just knowing to ask.
4️⃣The expensive one, when it’s worth it. A targeted combo for BRAF-mutant colon cancer doubled survival (30 months vs 15). It’s not cheap. But this is the case where the price buys you something real, the contrast that makes the first three land.
The pattern of the year: the next gains in cancer aren’t all locked behind a bigger price tag. Some are a referral, a dose, or a question you didn’t know to ask.
Which of these would you want your doctor to bring up first?
#REVIEW 🚨
How does #exercise reduce cancer risk? Zhuang et al. propose that physiological adaptation to aerobic activity reshapes adult stem cell behaviour, limiting transformation and tumour initiation
📖⬇️
https://t.co/aZ2RxF0eZ2
Durante años, la narrativa dominante sostuvo que la adicción podía entenderse casi exclusivamente a través de la dopamina. Este artículo propone una visión mucho más compleja, y probablemente más cercana a la realidad biológica: la conducta adictiva emerge de la interacción dinámica entre múltiples sistemas neuronales, gliales, metabólicos y neuroendocrinos.
La recompensa y la aversión no serían procesos separados, sino dimensiones de un mismo sistema de “valencia” que integra señales dopaminérgicas, orexinérgicas, histaminérgicas, endocannabinoides y relacionadas con el estrés. Incluso regiones poco exploradas del tallo cerebral, como el núcleo tegmental subventricular (SVTg), podrían desempeñar un papel central en la regulación de la motivación y la compulsión.
Quizá una de las ideas más interesantes es que la adicción deja de verse como un “defecto químico” aislado y comienza a entenderse como una propiedad emergente de redes cerebrales distribuidas, moldeadas por evolución, plasticidad y ambiente. En neurociencia, las explicaciones lineales suelen ser insuficientes frente a sistemas complejos.
https://t.co/nrDwhgUQs3
An exercise hormone derived from muscle—irisin— is neuroprotective, preventing brain cell loss, as seen in the experimental model of multiple sclerosis
@NatMetabolism
https://t.co/CC4KDOJTn1
https://t.co/9bbcLpW4g6
Nuevo artículo🔍🧬: Systematic Review of Monocyte Transcriptomic Profiles as Diagnostic and Prognostic Biomarkers in Colorectal Cancer https://t.co/usjmz5liLj #mdpiijms vía @IJMS_MDPI
🧬 #ScienceSaturday
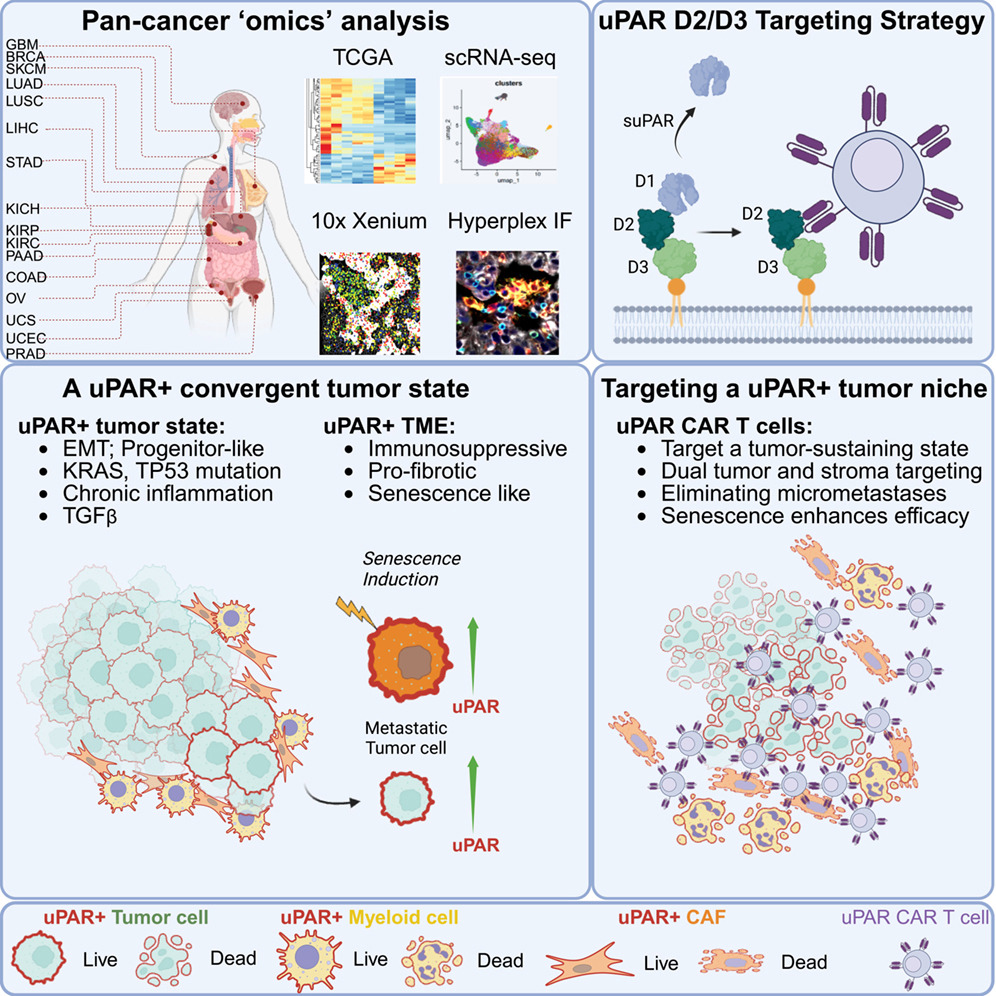
❓ What if cancer treatment could target not only tumor cells, but also the tumor’s stromal support: non-malignant, non-cancerous cells within the tumor microenvironment, that actively help cancer grow, spread, and resist treatment?
➡️ In a new study published in @CellCellPress, researchers identified uPAR, a cell-surface protein linked to aggressive tumor behavior, as a marker found on both solid tumor cells and the fibrotic, immune-suppressive environment that helps sustain them.
➡️ The team developed uPAR-targeted CAR T cells that attacked both tumor cells and their supportive stroma, leading to durable tumor regression across multiple cancer models, including metastatic disease.
➡️ They also found that senescence-inducing therapies, like chemotherapy, increased uPAR expression and made tumors even more vulnerable to CAR T cell treatment.
🌟 This dual-targeting strategy could help overcome some of the biggest barriers to CAR T therapy in solid tumors, including immune suppression and treatment resistance.
🔗 Read the study: https://t.co/dvHrEzUZ7F
@ZedaZhang@Aveline_Filliol@LoweLabMSKCC
1/ Thrilled to share our new paper, out today in @Nature: "Non-invasive profiling of the tumour microenvironment with spatial ecotypes".
Paper (open access): https://t.co/EujZFqU7wi
⭐️Don't miss this Review published @NatureCancer
as part of our Series on Tumor Heterogeneity and Plasticity
'Heterogeneity and plasticity of cancer-associated fibroblasts'
✒️By Ruth Scherz-Shouval, Mara Sherman and co-authors
🔗https://t.co/Qo6oplbnVx
#AdiposeTissue (AT) is a dynamic metabolic organ that shapes #obesity & cardiometabolic disease. New review discusses adipocyte & lipid turnover, inflammation & AT spatial organisation in human health & disease. #Metabolism#DiabetesResearch https://t.co/i0GxsxcSEo 🔓
Sucralose and the Gut–Immune Axis: Emerging Evidence Linking Dysbiosis, Barrier Alterations, and Implications for Colitis and Colorectal Cancer Immunotherapy
▶️ Emerging evidence suggests that chronic exposure to sucralose may alter gut microbial composition, epithelial barrier function, mucosal inflammation, & immune responses.
▶️ This review examines current experimental and clinical evidence on the effects of sucralose on the gut–immune axis, w/particular attention to its potential implications for colitis & colorectal cancer.
https://t.co/86SLTYxURj @HealthyFellow
Proposed mechanisms by which sucralose exposure may disrupt intestinal homeostasis, based primarily on preclinical studies.
— Sucralose exposure may impair epithelial barrier integrity & alter tight junction protein expression, potentially increasing intestinal permeability & microbial translocation into the lamina propria. — This process may trigger immune activation and promote a pro-inflammatory environment.
— In parallel, sucralose-induced dysbiosis may favor the expansion of taxa such as Bacteroidetes, Fusobacterium, & Enterobacteriaceae, further amplifying inflammation through increased production of cytokines (e.g., IFN-γ, TNF-α, IL-1β) & oxidative stress.
—Additionally, altered microbial metabolism may reduce levels of protective metabolites, and short-chain fatty acids (SCFAs), which normally support barrier integrity and immune regulation. Together, these alterations compromise intestinal homeostasis and may increase susceptibility to inflammatory bowel disease (IBD) and colorectal cancer (CRC).
New ESPEN Practical Guidelines on Ethical Aspects of Medical Nutrition Therapy
ESPEN has published a new practical guidelines on the ethical aspects of medical nutrition therapy (MNT), offering practical support for complex decision-making in clinical nutrition, including palliative care and end-of-life situations.
We warmly congratulate and thank the authors for their excellent work.
Read more here:
https://t.co/coigQ4X50o
Vitamin B12 is absorbed through two pathways. The first is intrinsic factor, a protein produced by parietal cells in the stomach. IF binds B12 in the small intestine and carries it across the gut wall via a receptor called cubilin in the distal ileum. This pathway is efficient but has a hard ceiling: it saturates at roughly 1.5 µg per dose. No matter how much B12 you swallow beyond that, IF cannot carry any more.
The second pathway is passive diffusion. About 1 to 2% of any oral dose diffuses across the intestinal lining without IF, and this occurs along the entire length of the gut. At dietary doses, this pathway is negligible. At supplement doses, it becomes the primary route of absorption.
Adams et al. (1971, Scand J Gastroenterol) measured whole body retention of radiolabeled cyanocobalamin at different doses. At 1 µg, roughly 50% was retained. At 5 µg, about 20%. At 25 µg, just over 5%. The NIH Office of Dietary Supplements reports approximately 2% absorption at 500 µg and 1.3% at 1,000 µg.
The fraction drops dramatically. But the total amount absorbed keeps rising. At 1 µg you absorb about 0.5 µg. At 1,000 µg you absorb roughly 13 µg total, of which approximately 10 µg comes from passive diffusion alone. The RDA is 2.4 µg. Even the backup pathway, working at 1% efficiency, delivers more than four times your daily requirement from a single pill.
This is the basis for high-dose oral B12 as an alternative to injections in patients who lack intrinsic factor. The NIH notes that high-dose oral supplementation "may be another treatment option" for pernicious anemia, though injections remain standard first-line therapy and the available randomized controlled trials comparing the two approaches are considered limited in quality.
One important nuance: absorbing B12 into your bloodstream is only the first step. After absorption, B12 must bind to a transport protein called transcobalamin to reach your cells. This complex, holotranscobalamin, is the biologically active fraction. It represents only about 20 to 30% of the total B12 circulating in your blood. The remaining 70 to 80% rides on a separate protein called haptocorrin, which does not deliver B12 to most tissues.
This is why serum B12 can be misleading as a status marker. A person can have a "normal" total serum B12 level while their holotranscobalamin, the fraction that actually delivers B12 to cells, is low. Methylmalonic acid is a more sensitive functional marker because it rises when cellular B12 is genuinely insufficient, regardless of what total serum B12 shows.
Absorption determines how much B12 enters your blood. Transport determines how much reaches your cells. Testing only total serum B12 measures neither of these processes accurately.
Adams et al., Scand J Gastroenterol, 1971
NIH Office of Dietary Supplements, 2024
Allen et al., J Nutr, 2018