TKAD resmî akademi dergisi yayın hayatına başladı🎉🎉The oficial academical journal of TASL has released first volume 🎉🎉 Volume: 1 Issue: 1 Year: 2020 (Hepatology Forum) https://t.co/hcAMsLZCJG
Kurban Bayramımız Kutlu Olsun
Paylaşmanın, dayanışmanın ve iyiliğin ön plana çıktığı Kurban Bayramı’nın; toplumumuza sağlık, huzur, mutluluk ve bereket getirmesini diliyoruz.
Bayramın tüm üyelerimize ve ülkemize huzur ve mutluluk getirmesini temenni ederiz.
Hepatolojide Bu Hafta’nın 296. Sayısı Yayında 📊
Prof. Dr. Onur Keskin tarafından hazırlanan yeni sayımızda, hepatoloji alanındaki güncel gelişmeleri ve dikkat çeken bilimsel verileri sizlerle buluşturuyoruz.
🇺🇸🇹🇷
As TASL, we warmly congratulate our distinguished colleagues elected to the 2027 AASLD leadership.
🇹🇷🇺🇸
TKAD olarak, 2027 AASLD yönetimine seçilen değerli meslektaşlarımızı içtenlikle tebrik ederiz.
🇹🇷 19 Mayıs Atatürk’ü Anma, Gençlik ve Spor Bayramımız Kutlu Olsun.
Bu anlamlı günde, başta Gazi Mustafa Kemal Atatürk olmak üzere Milli Mücadele’nin tüm kahramanlarını saygı, rahmet ve minnetle anıyoruz.
17. Ulusal Hepatoloji Kongresi başarıyla tamamlandı. Bilime ve yeniliklere doyduğumuz bu kongrede meslektaşlarımızla bir arada olmak harikaydı.
TKAD yönetim kurulu ve düzenleme kurulu adına katkılarından dolayı tüm katılımcılara ve paydaşlarımıza teşekkür ederiz.
17. Ulusal Hepatoloji Kongresi’nde 2. Gün Tüm Heyecanıyla Devam Ediyor! 🩺✨
Hepatoloji alanındaki en güncel gelişmeleri ve geleceğin hekimliğini şekillendirecek başlıkları uzmanlarından dinliyoruz.
17. Ulusal Hepatoloji Kongresi’nin açılışı, Kongre Başkanımız Prof. Dr. Dinç Dinçer, TKAD Başkanı Bülent Değertekin ve TGD Başkanı Prof. Dr. Ayhan Hilmi Çekin’in değerli konuşmalarıyla gerçekleştirildi.
The evolving landscape of obesity pharmacotherapy
Nature Reviews Drug Discovery, 2026
1️⃣ Obesity pharmacotherapy has moved from “weight loss drugs” to cardiometabolic disease-modifying therapy
Obesity is now framed as a chronic, relapsing, neuroendocrine-metabolic disease, not simply a lifestyle failure. The major therapeutic shift is from modest appetite suppression to hormone-based, receptor-targeted treatment acting on GLP-1, GIP, glucagon and amylin pathways. The review states that modern incretin and multi-receptor peptide therapies can produce average weight loss exceeding 20% in humans, with improvement in several obesity-related comorbidities.
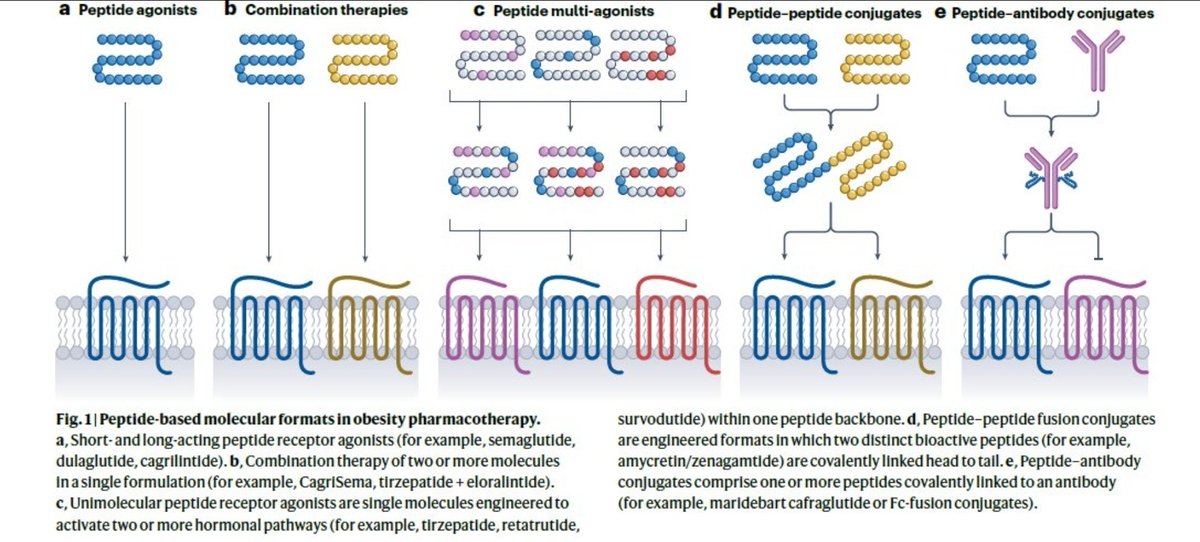
2️⃣ The figure shows the “molecular evolution” of obesity drugs
a. Peptide agonists
Single peptide receptor agonists such as semaglutide, dulaglutide and cagrilintide mainly target one hormonal pathway.
b. Combination therapies
Two molecules are co-formulated to produce additive or complementary effects, for example CagriSema or tirzepatide plus amylin-based therapy.
c. Peptide multi-agonists
One engineered molecule activates two or three receptors. Examples include tirzepatide, retatrutide and survodutide.
d. Peptide–peptide conjugates
Two bioactive peptides are covalently linked into one molecule, such as amycretin/zenagamtide-type formats.
e. Peptide–antibody conjugates
Peptides are linked to antibody or Fc-based structures to prolong half-life, improve tissue targeting or alter pharmacokinetics.
Clinical message: the field is moving from “one hormone–one receptor” to multi-pathway pharmacology.
3️⃣ GLP-1 receptor agonists opened the door, but multi-agonists are the next wave
Semaglutide 2.4 mg established that pharmacological weight loss could approach bariatric-level effects in some patients. Tirzepatide expanded the concept by combining GIP and GLP-1 receptor agonism, while retatrutide adds glucagon receptor agonism as a third axis. The review highlights this progression from GLP-1 agonists toward next-generation multi-receptor agonists.
4️⃣ Amylin is becoming a major partner pathway
Amylin-based drugs such as cagrilintide and newer amylin receptor agonists are clinically important because amylin complements GLP-1 biology. It promotes satiety, slows gastric emptying and may improve tolerability when combined intelligently with incretin therapy. The review specifically includes amylin receptor targeting among the expanded obesity pharmacotherapy pathways.
5️⃣ “Weight-loss quality” is the new clinical frontier
Future obesity therapy will not be judged only by kilograms lost. The key question will be: what type of weight is lost?
Clinicians must increasingly consider preservation of lean mass, muscle strength, bone health, nutrition quality, physical function and long-term metabolic durability.
CME INDIA Pearl:
A 20% weight loss with sarcopenia is not equivalent to 20% weight loss with preserved muscle and improved cardiometabolic fitness.
6️⃣ Obesity drugs are expanding beyond BMI reduction
The therapeutic scope is moving toward comorbidity modification: type 2 diabetes prevention, glycaemic control, cardiovascular risk reduction, heart failure with preserved ejection fraction, obstructive sleep apnoea, chronic kidney disease and MASH/metabolic liver disease. The Nature review cites the expansion of obesity pharmacotherapy into obesity-related comorbidities rather than weight loss alone.
7️⃣ Oral formulations may decide scalability
Injectables have transformed efficacy, but global scalability—especially in countries like India—will depend on cost, access, adherence, cold-chain issues, oral formulations and long-term affordability. The review identifies oral formulations as one of the major future strategies in obesity drug development.
Next....✈️
https://t.co/B9ogSeGlz0
La metformina no deja de sorprendernos. 🔬
Nuevo estudio: su diana no es el hígado. Es el intestino.
Lo convierte en una esponja que capta el exceso de glucosa.
70 años después, seguimos aprendiendo. Larga vida a nuestra reina 👸🏻 metformina
@NatMetabolism
🔗 https://t.co/0VMhOGDJYB
Lifespan extension from fasting depends not on sustained activation of lipid catabolism, but on its silencing upon nutrient replenishment. @NatureComms
Drug-induced fatty liver disease is evolving.
Over two decades, drug class patterns and trends have shifted—highlighting changing risks and the need for updated monitoring strategies.
👉 https://t.co/IPDQZJEuVr
#FattyLiver#Pharmacology#Metabolism
The number on your scale is not what your brain is responding to.
A new study followed 533 adults for up to 16 years with repeated abdominal and brain MRI. Participants came from four prior dietary intervention trials at Ben-Gurion University. Researchers measured cumulative visceral fat exposure and tracked brain volume, gray matter, hippocampus structure, and cognitive scores across the entire follow-up.
People with lower cumulative visceral fat had more preserved brain volume, larger gray matter, better hippocampus structure, and higher cognitive scores in late midlife.
What did not predict brain preservation: subcutaneous fat, BMI, total weight, lipid panels, inflammatory markers. The fat just under your skin showed no association. Body weight showed no association. LDL and CRP showed no association.
One blood signal mediated the relationship between visceral fat and brain aging. Glucose control. Fasting glucose and HbA1c. Not cholesterol. Not inflammation.
The most provocative finding involves time. Visceral fat reductions during the original 18-month dietary intervention predicted better brain structure 5 to 10 years later. Even when participants regained their weight. The body composition memory outlasted the diet itself.
A few caveats. The cohort was 86% men, so generalizability to women is limited. The follow-up after randomization was observational, not interventional. MoCA is a cognitive screen, not a full neuropsychological battery.
The practical takeaway is uncomfortable for the GLP-1 era. Weight loss alone is not the brain-preserving move. Where the fat sits, and what your fasting glucose looks like over years, matter more than what the scale says on any given morning.
-
Pachter D, et al. Sustained visceral fat loss is associated with attenuated brain atrophy and improved cognitive function in late midlife. Nature Communications, 2026.
What are the benefits and harms of GLP-1s in older adults? 🤔
It's challenging to answer this question because most randomized controlled trials did not include large numbers of older adults.
📊 In a meta-analysis of older adults from 11 RCTs with 85,373 individuals who either received GLP-1 or no GLP-1:
⬇️ GLP-1 RA with 15% reduction in MACE (CV death, stroke, MI) 🫀
⬇️ 22% reduction in kidney composite outcome