@AlbertoEspay@movedisorder Great facts. Like facts.
Is it the load, or level of misfolded proteins associated with neurological disease
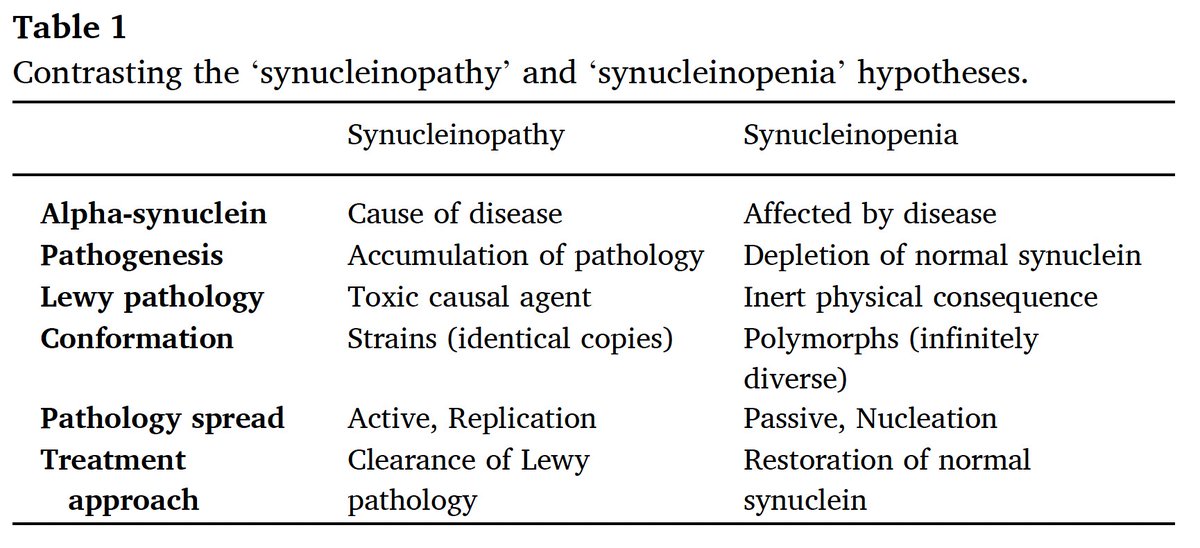
Or is it the level of remaining protein?
@ScienceofPD@PDandHDLab AUC in the low 80s seems to need some work to be predictive when 50 is flip a coin. Pretty interesting cohort at baseline with a nasty mean updrs score and old enough to have 20-25 percent die due to old age.
@ParkinsonsEU The word, smart therapy has a perceptual problem as well in that by default. Other therapies are not smart. there are plenty of good choices without starting a new problem when trying to fix another
Barely a day goes by without me seeing someone with an abnormal movement disorder in the street or on the Tube.Only a minority would ever be seen in a neurology clinic.
More will be seen by mental health services, drug rehabilitation clinics and day centres for the elderly.
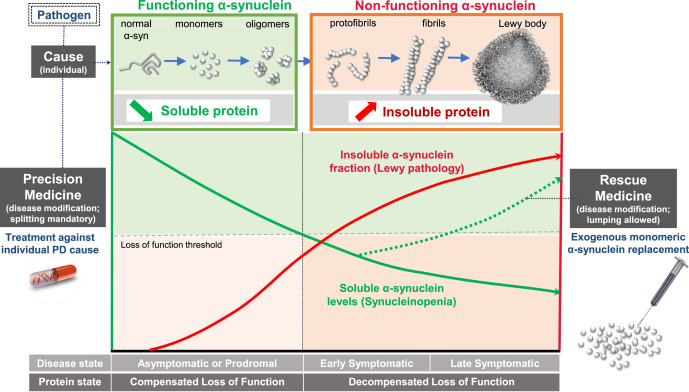
There is lots we don’t know and much yet to learn in PD. Classification systems can help zero in closer on groups of patients to figure out if synuclein is friend, foe or innocent bystander @AlbertoEspay@ajlees@MichaelOkun@basbloem @RayDorseyNeuro @BrundinPatrik@KBI_UHN
Check out the commentary by Hugh Johnston (former patient advisory board chair) about the new biologically based model for classifying PD, called "SynNeurGe", by Dr. Tony Lang & team!
Article: https://t.co/UlC6S4UGSi
Full issue of Connect: https://t.co/UlC6S4UGSi
The Synucleinopenia Hypothesis: Lewy pathology is made of what once were normal α-synuclein monomers. Entrapped, they can no longer function. Losing enough α-synuclein brings out #Parkinsons. Lewy pathology alone doesn't. @ajlees@ParkinsonismD
https://t.co/u8PLSYoSC7
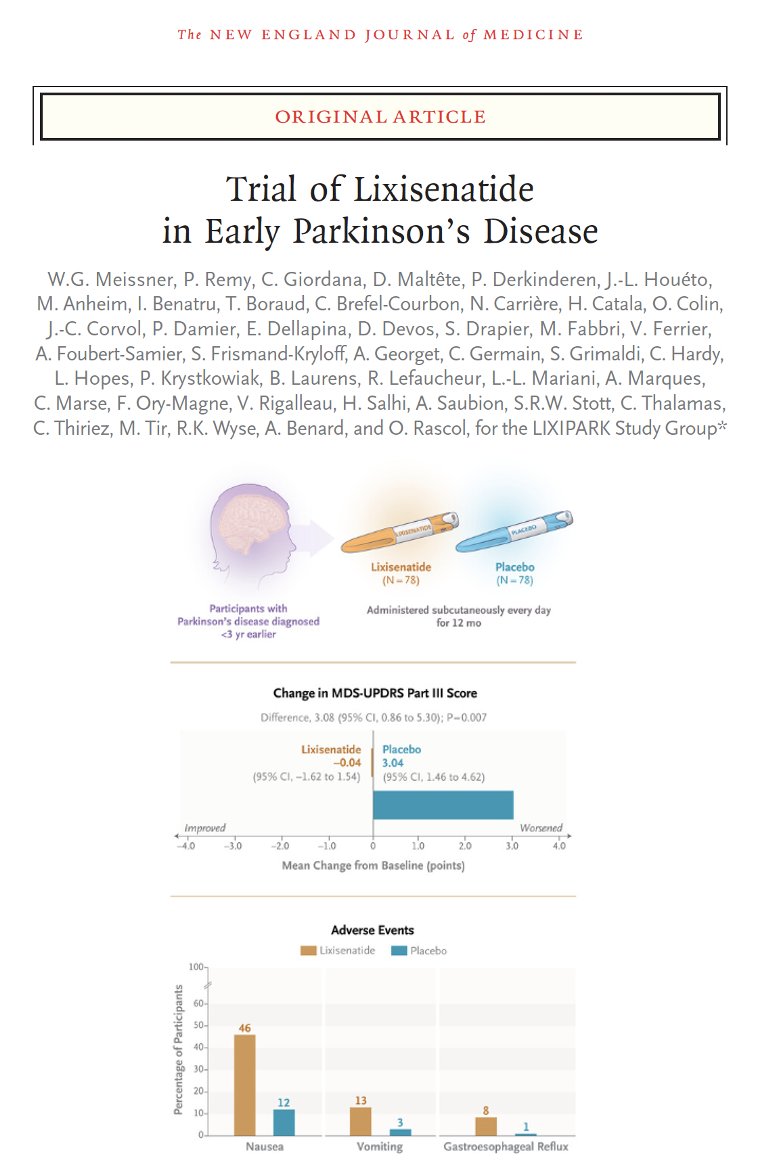
Big news with positive result announced for a randomized study of a GLP-1 agonist for Parkinson's just released @NEJM. A new era for Parkinson's or alternatively, more questions than answers raised by Meissner and colleagues.
Key Points:
- This multi-center French trial studied Lixisenatide which is a glucagon-like peptide-1 receptor agonist used for in diabetes.
- The trial was a phase 2 double-blind randomized and placebo-controlled.
- The authors wanted to know whether this drug would affect the progression of motor disability.
- Who did they study? Parkinson's treated and with symptoms less than 3 years.
- If you enrolled, you received daily subcutaneous lixisenatide or a placebo.
- The primary outcome was a change in the motor PD scale called the MDS UPDRS when on dopamine medication after one year.
- There were 78 people in each group.
- The motor scores slightly improved in lixisenatide and worsened by 3 points in the placebo group.
- There was a very short 2 month washout period where those getting the active drug stopped it and the benefit persisted.
- Nausea was the most common side effect and occurred in about 1/2.
My take: We have continued our multiple year love affair with various diabetes drugs and their potential links to Parkinson's disease, however the current study results are the most promising. Interpret with caution: there is a number called the 'clinically meaningful threshold' and those reading this study should appreciate that the results 'fell short' of this important metric. There will certainly be many arguments among experts as to whether this study met a minimum threshold for neuroprotection, and my personal opinion is that it did not. Here is an important message: In my view do not rush to prescribe this drug or try to creatively acquire it. We have been down this road many times including leukemia drugs, cough syrups and lithium. The data is not yet there to proceed to prescribing. More importantly, the weight loss associated with GLP-1’s is not desirable in the majority of cases of Parkinson’s disease and the nausea and vomiting will not be a welcome symptom. We must ask the important questions as to why the non-motor outcomes did not change, and why the other GLP-1 studies have been negative? Is there a blind spot here we are missing? Please appreciate this was trialed in only very early Parkinson's disease and thus there may be 'generalizablility' concerns. I do not want to diminish a great paper with a randomized design and encouraging data, however let's not rush to the drug store counter. Perhaps we should consider ad augusta per angusta – to glory through narrow spaces by continuing to follow the data with diabetes drugs and see where it leads and what it teaches us.
https://t.co/Gna336Awip #Parkinsons #OZEMPIC #diabetes #GLP1
A classification system for PD that recognizes 1) we need to understand if synuclein is friend foe or innocent bystander, 2j there are many types of PD some which don’t involve synuclein and 3) a positive SAA without clinical PD is not a disease https://t.co/NOJgSss8NE
I’m very proud of @GGilmourMD's fantastic new review on diagnosing #FMD. There are many excellent reviews on this already, and here’s what we add that’s different (tweet summary).
Moving Beyond Movement: Diagnosing Functional Movement Disorder https://t.co/GiFVVUGw16
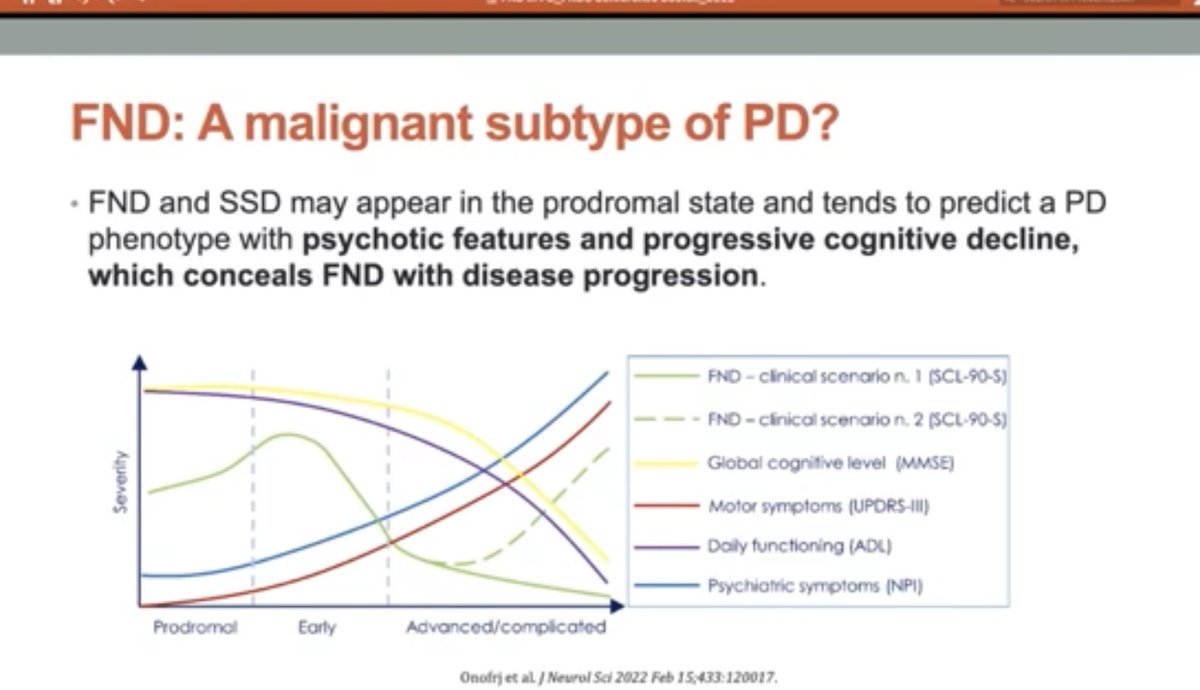
@DrTFromKC@ajlees@jonstoneneuro@AlanCarson15@AlbertoEspay Good question. Apologies for the curt tweet. Am suggesting there is a significant overlap and that prevalence is fairly common that patients with PD will have a basket of FND that ensues. Also am suggesting that incidence of malignant phenotype amongst them is low.