Malcolm Gladwell revealed why you shouldn't go to Harvard:
1. America does not have a shortage of students who want science and math degrees. It has a shortage of students who finish them. Half of all high school seniors who intend to study STEM drop out by the end of their second year. The problem is not interest. It is persistence.
2. The obvious assumption is that smarter students persist longer. So Gladwell tested it. At Hartwick College, a small liberal arts school in New York, the top third of math SAT scorers took the majority of STEM degrees. The bottom third dropped out in large numbers. The data seemed to confirm it. Smarter kids stick around longer.
3. Then he looked at Harvard. The bottom third of Harvard's math SAT scores are equal to the top third at Hartwick. By the logic above, everyone at Harvard should graduate with a STEM degree. They are all brilliant. Nobody should be dropping out.
4. Harvard showed the exact same pattern as Hartwick. Top students graduated. Bottom students dropped out like flies. Even though the bottom Harvard students were objectively brilliant by any global standard. Something else entirely was driving the dropout rate.
5. That something is called relative deprivation theory. Human beings do not measure themselves against the world. They measure themselves against the people immediately around them. A Harvard student in the bottom third does not think I am in the top one percent of all students globally. They think that kid next to me keeps getting everything right and I keep getting it wrong. So they quit.
6. The research from UCLA puts a specific number on it. Your odds of graduating with a STEM degree fall by two percentage points for every ten point increase in the average SAT score of your peers. Choose Harvard over the University of Maryland and your chance of finishing a STEM degree drops by thirty percent. Thirty percent. Just to put a brand name on your resume.
7. Relative position matters more than absolute position when it comes to confidence, motivation, and self belief. The eightieth percentile student at Harvard looks up at the people above them and feels like they cannot compete. The number one student at a state school feels like they can conquer the world. That feeling drives everything.
8. The practical hiring implication is radical. Class rank matters more than institution name. Gladwell argues companies should have a don't ask don't tell policy for where someone went to college. Hiring only from top schools means missing the top students from every other school. That is not smart hiring. That is brand worship.
9. When choosing a college, never go to the best school you get into. Go to the school where you are guaranteed to be near the top of your class. Being a big fish in a smaller pond does not just feel better. It statistically produces better outcomes than being a small fish in the most prestigious pond available.
10. So why do we keep choosing Harvard over Maryland? Because we are flattered. Because the acceptance letter feels like validation. Because we make an irrational decision in a moment of enormous flattery and call it ambition. Gladwell's conclusion is simple and brutal. When we have the chance to join an elite institution we do things that are genuinely against our own interest and we feel great about it the whole time.
I'm a cardiologist. I've held dying hearts in my hands in the cath lab at 3 AM. And I need to tell you something that changes everything about how we prevent heart attacks.
For decades, the entire field was built on one target: lower LDL cholesterol. Statins save lives — that's settled science. But too many of my patients did everything right — took their statins, hit their numbers, lived clean — and still ended up on my table with a ruptured artery.
We were treating the smoke while the fire kept burning.
The fire is inflammation. And the evidence is now overwhelming.
The CANTOS trial proved it first — lowering inflammation independent of cholesterol reduced cardiac events. But the newer data is what keeps me up at night.
AI-enhanced CT angiography can now detect inflamed arteries by measuring changes in the fat surrounding your coronary vessels — the perivascular fat attenuation index. Higher inflammation in the fat around even one artery independently predicts cardiac death. When multiple arteries show inflammation, the risk multiplies dramatically — even in patients whose cholesterol looks perfect.
This isn't theoretical. This is measurable. Right now. On a scan you can get this month.
Low-dose colchicine — a drug that's been around for centuries for gout — is now FDA-approved specifically for reducing cardiovascular events. It works by quieting the inflammatory cascade that destabilizes the plaque sitting in your arteries. A pill that costs pennies is saving lives the statins couldn't reach.
And the next wave is already in Phase 3 trials. Ziltivekimab — an IL-6 inhibitor — targets the central inflammatory pathway driving atherosclerosis. Phase 2 data showed a 90% reduction in hsCRP. The ZEUS cardiovascular outcomes trial is enrolling now, with results expected late 2026 into 2027. If positive, anti-inflammatory therapy will become standard in managing heart disease alongside lipid-lowering. The era of inflammation-targeted cardiology is arriving.
But it goes deeper than drugs. AI is now predicting heart failure and cardiac events 5+ years before symptoms — integrating CT imaging, electronic health records, and genetic data with accuracy that jumps far beyond traditional risk calculators.
And polygenic risk scores — a simple genetic test that flags inherited cardiovascular risk — are now formally recognized as a risk-enhancing factor in the 2026 ACC/AHA guidelines. A single blood draw can reveal risk that's been silently building since birth. Decades before the first chest pain.
Here's what this means for you right now — today:
Ask your doctor for a high-sensitivity CRP test. It's cheap, routine, and measures the systemic inflammation that standard cholesterol panels completely miss. You can have perfect LDL and inflamed arteries that are quietly preparing to rupture.
If your hsCRP is elevated, discuss low-dose colchicine with your physician. It's FDA-approved for exactly this.
Push for a coronary CT angiography with AI plaque and inflammation analysis if you have risk factors. This isn't the stress test your parents got. This is 3D visualization of your actual arteries — with AI quantifying not just how much plaque you have, but what kind it is and whether the surrounding tissue is inflamed.
Consider polygenic risk score testing — especially with a family history of early heart disease. It's now guideline-supported.
And the foundation that never changes: move daily, eat real food, sleep 7-9 hours, manage stress, and know your numbers — ApoB, Lp(a), hsCRP, fasting insulin.
I left Iran as a child with nothing. I rebuilt everything in a country that gave me the freedom to become a physician. I've spent twenty years watching patients get second chances.
The ones who haunt me aren't the ones who died on my table. They're the ones who survived but never acted on what the science was telling them — years before the event that didn't have to happen.
You can have perfect cholesterol and still have a heart attack. Inflammation plus genetics can drive plaque rupture in arteries that look "fine" on a standard panel.
The myth that normal cholesterol means you're safe has cost more lives than I can count.
We now have the tools to detect the fire — not just the smoke. AI to see it. Genetics to predict it. Drugs to quiet it. And the ancient basics — movement, real food, sleep, purpose — to prevent it from starting.
Prevention is the new cure. And the science to make it real is no longer coming.
It's here.
The current physical activity guidelines are too low.
I've been saying this for a while. And a new study confirms it.
Meeting the standard 150 minutes/week was associated with only a modest ~8–9% lower cardiovascular risk.
The biggest protection occurred at roughly 560–610 minutes/week, about 3–4× higher, where cardiovascular risk was 30% lower.
We need to distinguish between the minimal activity volume required for basic protection, and the substantially higher volumes required for optimal resilience.
There are many non-pharmaceutical options for helping ADHD/behavioral symptoms.
It's cool to see Nick is having success by combining a few low-risk supplements.
@hbomax 🚨 Your Cycling Events this morning, the Giro d’Italia and the Grand Prix du Morbihan, begin with either the WHOOP or Land Rover promos, and then there is just a ‘spinning circle’ that never connects. I’ve tried five times to connect, all unsuccessful.
🚨 Anthropic's own team just showed how to actually use Claude Code properly.
30 minutes. free. the person who created Claude Code.
watch the workshop. bookmark it.
worth more than every $500 course you almost bought.
you've been using Claude without knowing 40 of its commands.
Then read the guide below.
Muscle loss with age is common, but much of that decline is driven by inactivity, not aging alone.
On average, we reach peak muscle mass somewhere between 20 and 30, then lose about 8% per decade after that. By the time many adults reach their 70s and 80s, they may have only 60–80% of the muscle mass they had at 30.
A big reason why is anabolic resistance. As we get older, muscle becomes less responsive to amino acids, one of the key signals for building and maintaining muscle.
This is where resistance training becomes non-negotiable. It's one of the main signals that tells muscle to grow. And just as importantly, it helps re-sensitize muscle to amino acids, so the body responds to protein more like it did when you were younger.
The New Octogenarians
80 year old Rafael Vera decided he'd rather build his body
than just waste away playing bingo in a retirement home.
He has more muscle than most men at any age.
He is part of a new generation of octogenarians reinventing old age.
How do you plan to spend your ninth decade of life?
Receipts are an overlooked source of exposure to endocrine-disrupting compounds
Thermal paper receipts are coated with bisphenol A (BPA), a plastic chemical that can be absorbed through the skin during handling
It might feel trivial, but repeated exposure adds up
Cashiers who handle receipts regularly have very high BPA levels, and hand creams or sanitizers can increase absorption up to 100-fold
If you don't need the paper copy, choose an emailed receipt instead
And if you handle receipts for work, nitrile gloves (not latex) can help reduce exposure
Small, consistent habits like this can reduce your total chemical burden more than you might think
Why won't latex gloves protect you from BPA/BPS in thermal receipts (or EKG paper)?
Latex (natural rubber) is permeable to BPA/BPS. These chemicals dissolve into the latex polymer and slowly migrate through to your skin, especially with repeated handling throughout the day.
Nitrile gloves actually work - their tighter synthetic structure blocks BPA/BPS permeation much better than latex, which is why I recommend it for cashiers, nurses, doctors, and anyone frequently handling thermal paper.
"Peakspan" should be the longevity marker everyone's talking about.
It refers to how long we can maintain 90% or more of our peak capacity in one of several health domains like muscle strength, cognitive function, or fertility.
And it recognizes that these systems peak at different ages and decline at different rates. So we need to strategically target each one as we age to maintain their function as high (and for as long) as possible.
I spoke with @StevenBartlett about "Peakspan" recently on his podcast.
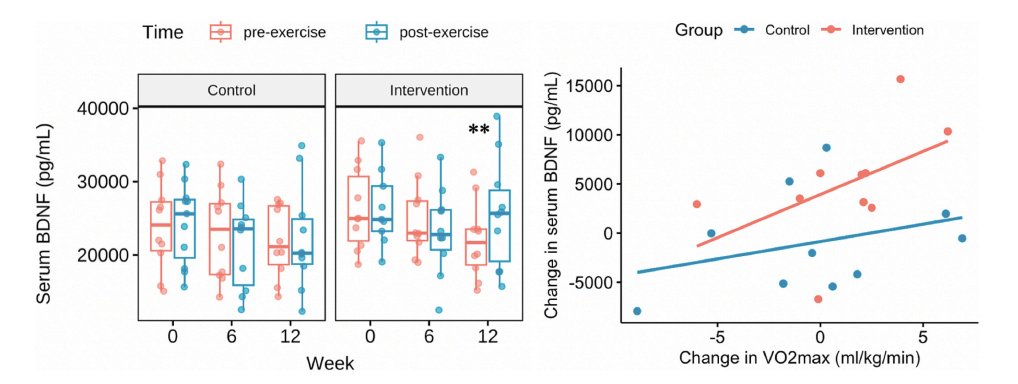
When you get fitter, you release more BDNF after exercise.
Improvements in VO₂ max after 12 weeks of training were associated with greater changes in post-exercise BDNF levels (even though resting BDNF didn't change). And the more VO₂ max improved, the higher BDNF rose after exercise.
Post-exercise BDNF was also associated with changes in prefrontal cortex activity during cognitively demanding tasks.
This illustrates a neat relationship between aerobic fitness, BDNF, and cognitive function!
For 25 years, my team has been told we were wrong, by scientists, big pharma, the media, ethicists, and trolls. It hasn’t been easy
Looking back, it was 100% worth it
Here’s why you should believe in yourself… 🧵
10/
My take-home: this updated ACSM stand shifts the conversation away from rigid rules and toward evidence, flexibility, accessibility, and adherence. People do not need the perfect program. They need to start training, keep training, and make it fit their goals.
@kellyfj1@foundmyfitness Hey Frank, it’s been a few years, but I believe I started buying this based on Rhonda’s recommendation. I like that they are capsules, versus hard tablets/caplets.
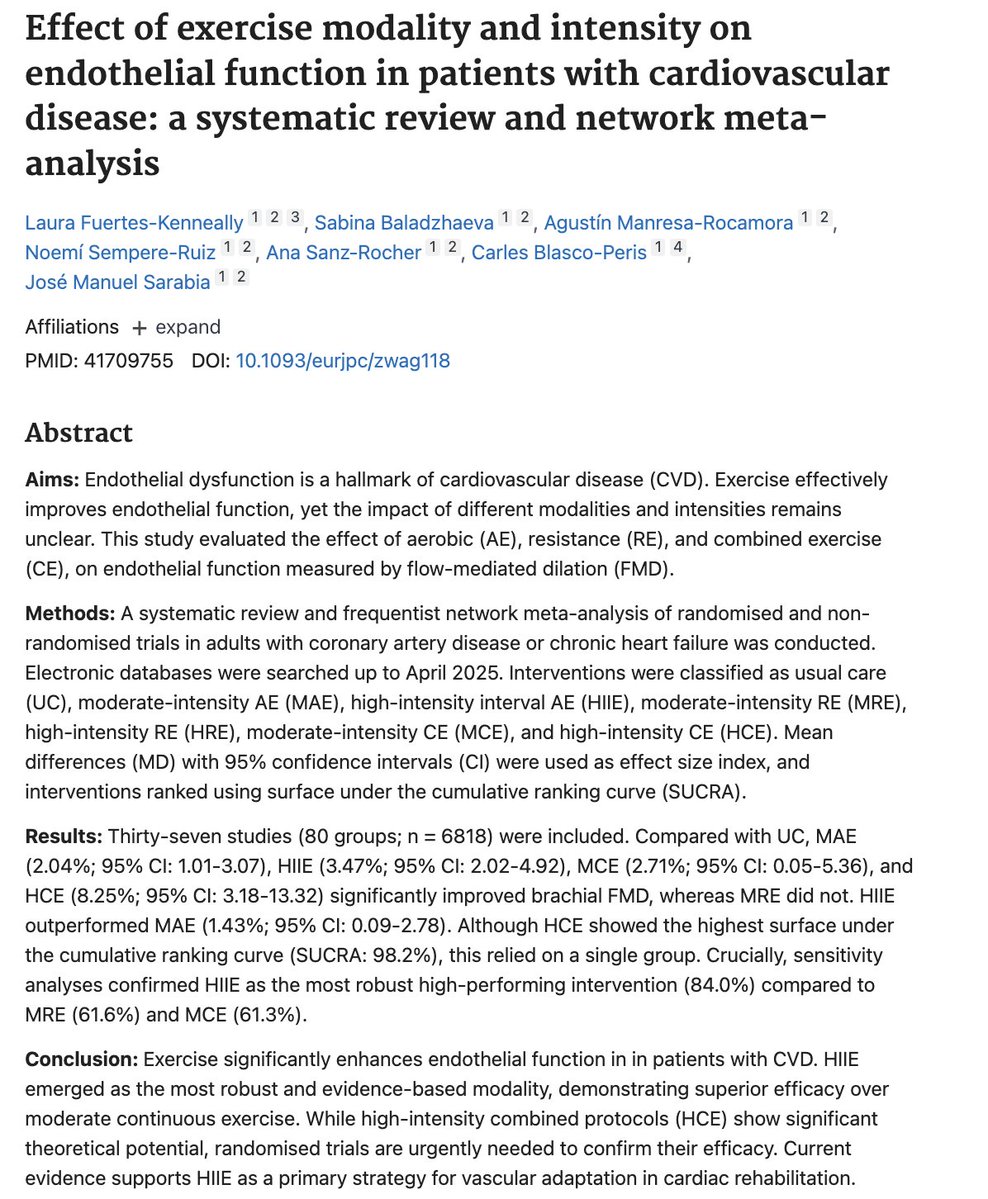
HIIT may be the single most powerful way to improve endothelial function.
A recent meta-analysis found that high-intensity interval training improves flow-mediated dilation (FMD)—a key measure of blood-vessel health and a strong predictor of future cardiovascular risk—by about 4%. That’s meaningfully larger than what’s typically seen with moderate-intensity aerobic training, resistance training, or even combined aerobic + resistance, which tend to improve FMD by 2–3%.
Mechanistically, this comes down to shear stress, the frictional force of blood flow against the vessel wall. HIIT generates a large, pulsatile shear stimulus (often ~2–4× higher than resting), which appears to be a potent signal for beneficial arterial remodeling.
This is one reason vigorous exercise shows such a strong protective effect against cardiovascular disease. It gives a vascular training stimulus that many other modalities simply don’t match.