People who don't follow cancer research often ask me why we haven't cured cancer. That perception masks a wonderful reality: We make amazing, stepwise progress every year, and the result is that many people live much longer today than they would have previously.
Right now we're in the thick of the annual meeting of the American Society of Clinical Oncology, the biggest research meeting on new cancer medicines, and this morning a bunch of really important studies dropped. I'm going to review them here.
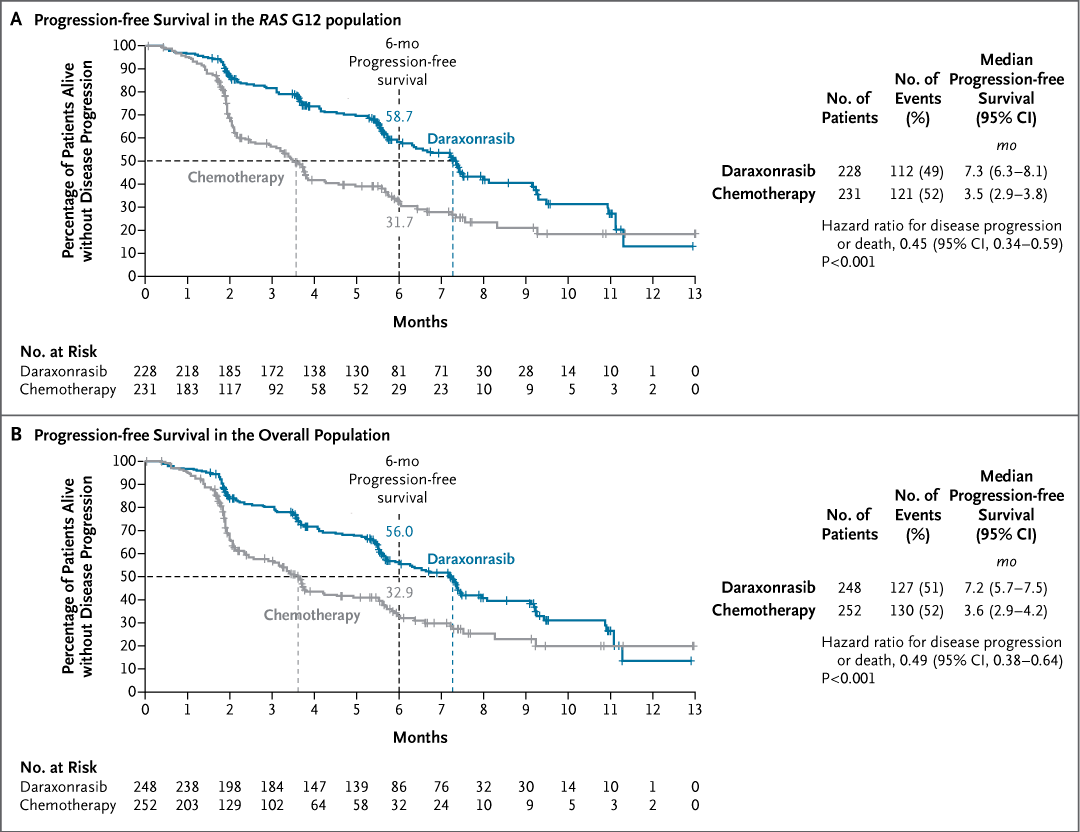
This first image is the result for daraxonrasib, a treatment for pancreatic cancer that is generating consdirable excitement. The green line is the probability of living for patients who got the new drug; the gray one is the chemo control group.
If you follow cancer drugs, a chart like this will make your breath hitch a little. I'm going to review these and some other data here.
Original Article: Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer (phase 3 RASolute 302 trial) https://t.co/y4G27hfORg
#ASCO26 | @ASCO
7yr CROWN update of 1L lorlatinib
55% progression-free at 7 YEARS.
Median PFS STILL not reached.
In metastatic solid tumors, this is essentially unheard of. Let that sink in.
And hopefully, one day, this becomes the standard (or even better) for ALL metastatic cancers.#ASCO26
We show that genetic and non-genetic resistance mechanisms co-exist in KRASi-treated tumors. The early adaptive phase, however, is dominated by cancer cell-intrinsic inflammatory reprogramming. TBK1 inhibition synergizes with KRAS/EGFRi.
Thanks to @theNCI and @BWFUND
Our paper, co-led with @kevanchu in the @dow_lab, is out today in @Cancer_Cell. We analyzed pre-treatment, on-treatment, and post-progression biopsies from 12 CRC patients treated with KRASi + EGFRi.
https://t.co/4KsCQsagil
Our paper, co-led with @kevanchu in the @dow_lab, is out today in @Cancer_Cell. We analyzed pre-treatment, on-treatment, and post-progression biopsies from 12 CRC patients treated with KRASi + EGFRi.
https://t.co/4KsCQsagil
La EMCS del @TecdeMonterrey afirma su liderazgo académico con resultados sobresalientes en el #ENARM.
Nuestras sedes continúan posicionándose sostenidamente entre los primeros lugares de la CDMX y del país en aceptación y conocimientos médicos.
Cancer survival in the U.S. just crossed 70%.
It was 63% in the 1990s.
That gap = 4.8M people alive today.
This one chart captures survival gains across 29 cancer types.
The wins are real.
So is the unfinished work.
▪️CML: 31% → 72%
▪️Multiple myeloma: 32% → 62%
▫️Kidney: 59% → 82%
▫️Metastatic melanoma: 16% → 35%
▫️Childhood ALL: 80% → 92%
But some cancers barely moved.
Cervical cancer outcomes actually worsened.
None of this is abstract progress, though.
These are birthdays, grandkids, and years of life returned.
This is what funded science does.
Next time someone asks if cancer research works, show them this (full) chart.
- - - - -
Source: ACS Cancer Statistics 2026 · SEER · 𝘷𝘪𝘢 @Jori_health
- - - - -
Top 3 universidades de medicina en promedio de calificación del ENARM 2025:
1. Universidad Panamericana
2. Tec de Monterrey campus Jalisco
3. Tec de Monterrey campus Monterrey
¡Muchas felicidades! 🙌
Referencia: https://t.co/6ONxPBOXZI
KRAS mutations drive 25% of *all* cancers.
We just cracked an entire class.
This is a big deal.
For decades, KRAS was called “undruggable.”
It became accepted as fact (it wasn’t).
This week at AACR:
▫️5 KRAS drugs
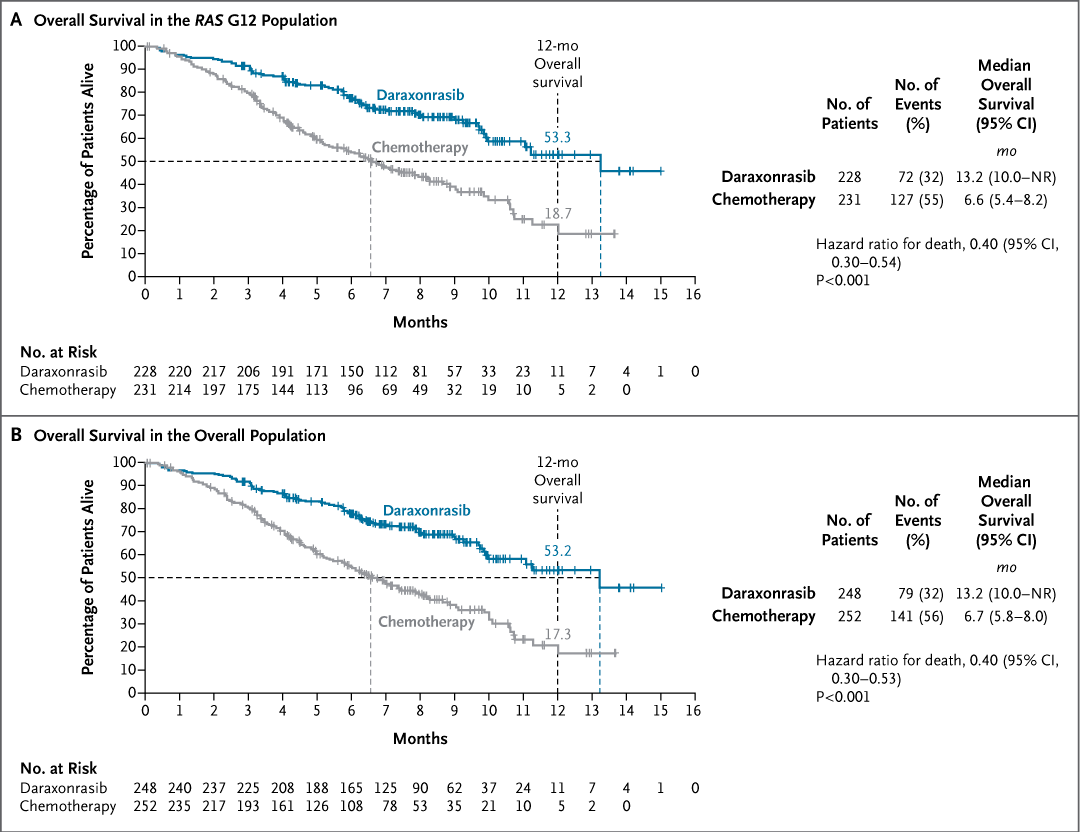
▪️One nearly doubled OS in pancreatic cancer.
▫️13.2 vs 6.7 months (HR 0.40)
This is what happens funded science does.
If you’ve ever been told your target is impossible,
look at this chart.
- - - - -
Source: US Clinical Trials | AACR'26 | RevMed Phase-3 | via @Jori_health
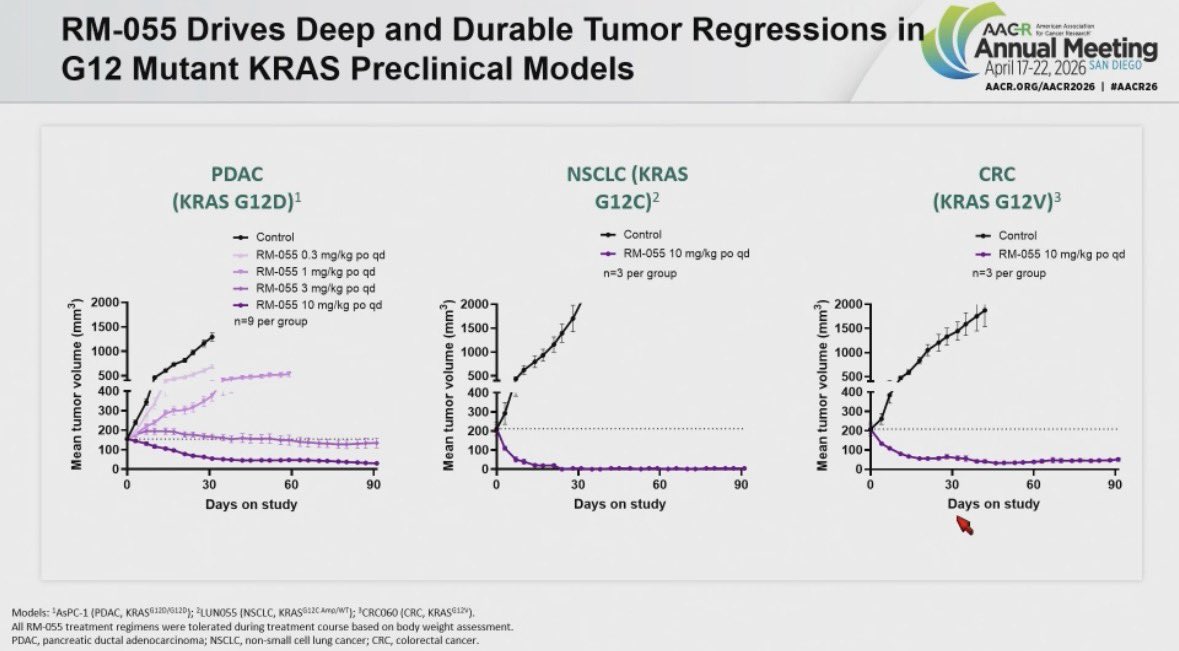
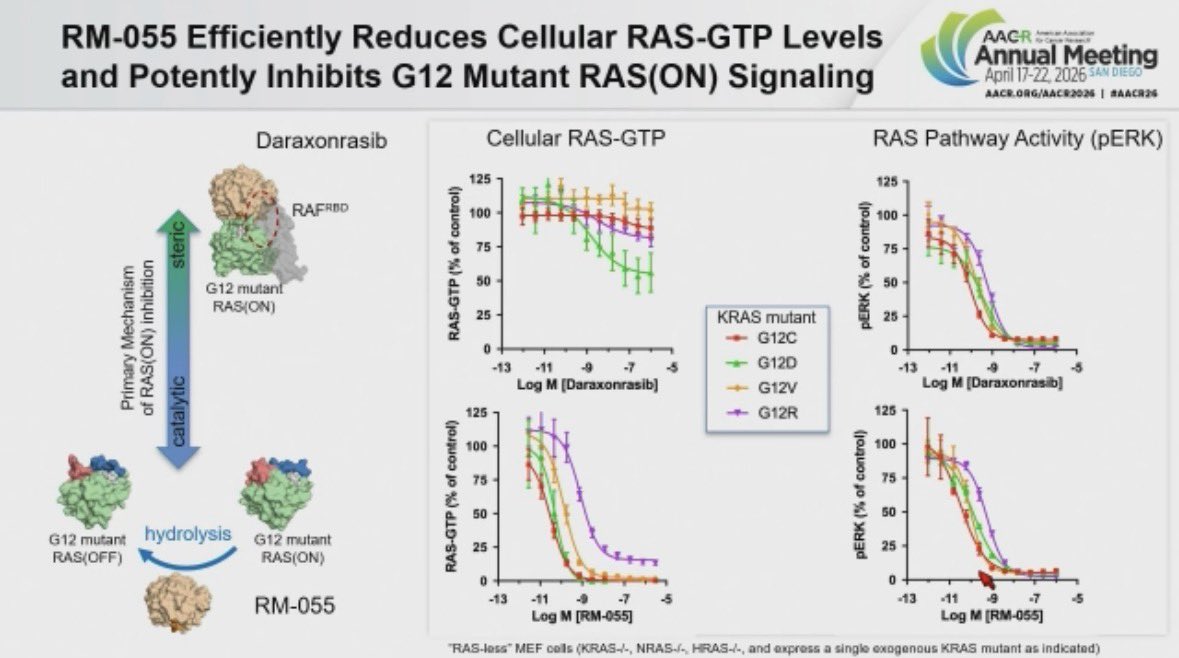
New compound from @RevMedicines RM-055 disclosed at #AACR26
They took a subtle finding 👉🏽Daraxonrasib-CYPA complex modestly increasing RAS GTP hydrolysis 👉🏽 to build a RAS GAP on steroids. RM-055 flattens Daraxonrasib resistant tumors including RAS amplified cases across models.
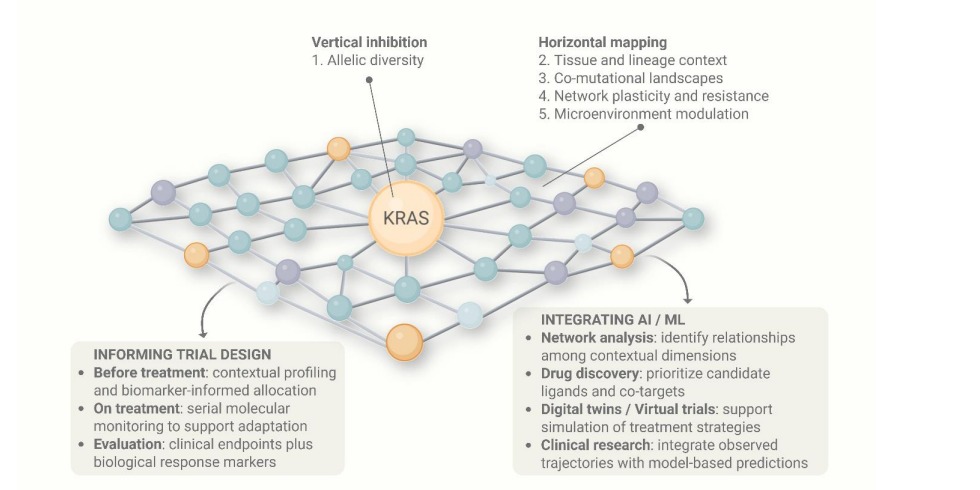
KRAS is no longer “undruggable.”
But that’s not the real question.
Why does targeting KRAS not lead to the same outcome across cancers?
Maybe KRAS is trying to teach us something.
Cancer is not just a mutation.
It’s a system.
How that mutation develops,
the microenvironment it lives in,
the pathways it interacts with,
and how resistance emerges…
This is what we need to understand.
Because we now know:
Targeting a single mutation is not enough.
We need to target the network.
@OncoDaily@OncBrothers@myESMO@JCO_ASCO@ASCOPost@Dr_R_Kurzrock@tompowles1@ilyassahinMD
https://t.co/G8FBoEgQIE
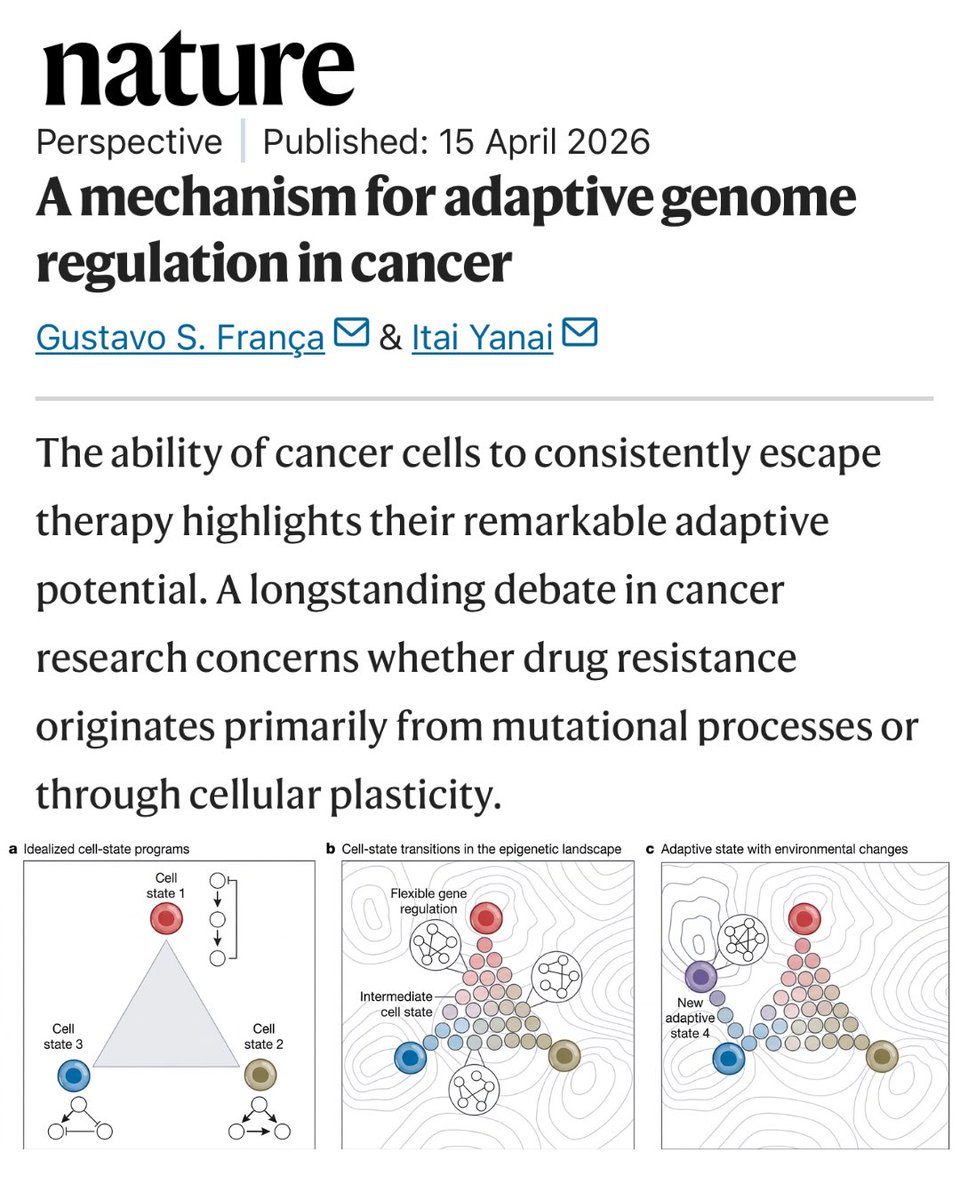
New research in Nature suggests cancer cells can learn to resist therapy, not by mutating, but by reprogramming themselves.
In #lungcancer, resistance to targeted treatments is a significant challenge. Understanding how this happens is an important step in the search for better treatment
🔗 https://t.co/RvSA6FljUj #LCSM
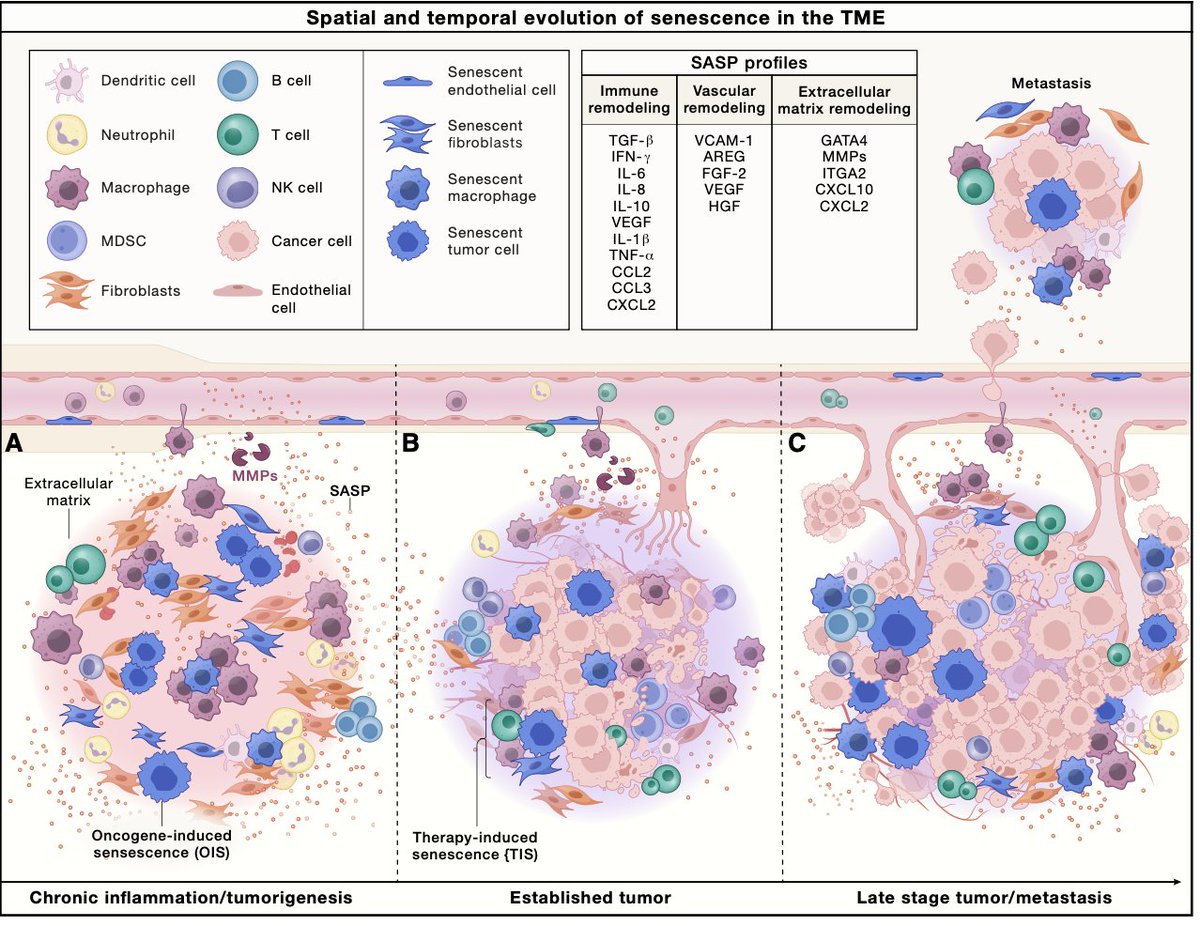
Cell senescence and how it predisposes to cancer, no less how we may be able to modulate it. An outstanding @CellCellPress review
https://t.co/bmAXOS1Ybz
Filled with joy to share that I will be joining @BrighamMedRes@HarvardMed for internal medicine residency.
I am deeply grateful to my mentors, school, family, and friends for their support throughout this journey.
#Match2026#IMGs@UPMexico@DanaFarber
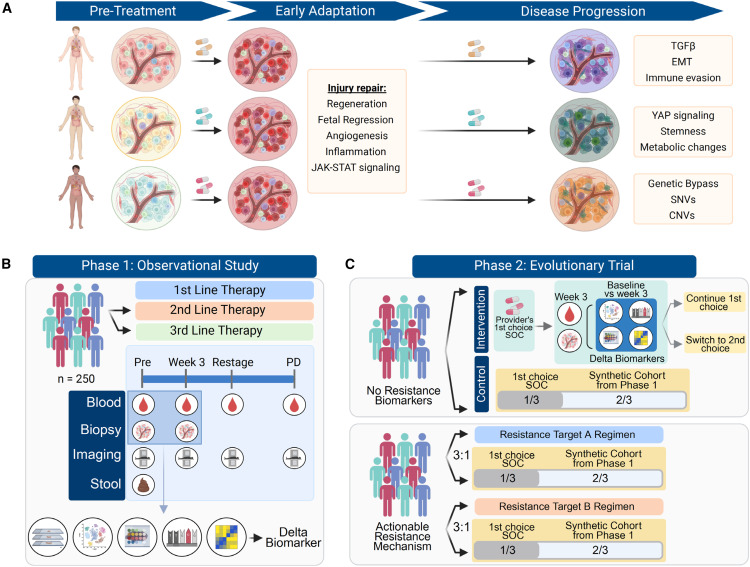
Check out this Cancer Cell commentary by my PI, Dr. Alonso et al!!!
ASCEND-CRC tracks tumor evolution over time to identify early adaptive changes and intercept resistance in metastatic CRC.
🫡🫡👏🏻
Happy to share our commentary in @Cancer_Cell describing ASCEND-CRC, an adaptive clinical trial designed to track tumor evolution in real time and adjust therapy before resistance takes hold
https://t.co/TWvB2ffbVL