Very pleased to share the results of the eternal question on the usefulness of Pelvic RT in High Risk Prostate cancer. Hope the debate will settle now. Thanks for the great support. https://t.co/UhvlZHJHtK
@TataMemorial@ACTREC_TMC@docpriyamvada#JCO@ASCO_pubs@APCCC_Lugano
Survey results on #ProstateCancer management treatment preferences in South Asia. @VedangMurthy@TataMemorial joins @neerajaiims@huntsmancancer describing the Indian approach to prostate cancer care. He outlines four practical principles guiding treatment decisions in resource-constrained settings. #WatchNow > https://t.co/9sFpLHXWKs
RCC pT4NoMo 1 yr post op evaluated for a persisting loin pain with a CT scan.your diagnosis #medtwitter
Are traditionally used practices sidelined by modern day dominance of immunotherapy .In low resource setting can adj Sunitinib or post-op RT still be used.
@VedangMurthy
@DrAndrewLoblaw@Soum_Roy_RadOnc Dog’s dinner!
MDTs going to be fun!
I am genuinely fascinated by all this, though. So many issues & factors involved, especially when Urologists are the gatekeepers
Standard of care if you are going to operate is surgery then salvage if needed. This was not included in the trial so hard to say this is a postive trial for neoadjuvant therapy where this has not been tested and all previous trials negative.
MFS by conventional imaging identical between ENZARAD and PROTEUS at 5 y and both trials negative for addition of ARPI. This was the initial primary in PROTEUS and hard to see why should be viewed as positive. PET imaging triggered by PSA >0.2 hence PROTEUS MFS = PSA PFS
Trials in localized prostate cancer are incredibly difficult to pull off, especially given the rapidly changing imaging and therapeutic landscape, so major congrats to the investigators.
For me, top line results: small MFS benefit when MFS is defined by either conventional imaging or PSMA PET. No MFS benefit by conventional imaging.
Critically, there were significant differences in PSMA PET utilization. Post hoc analysis showed that 686 patients (64.9%) in the apalutamide group and 755 patients (71.8%) in the placebo group underwent PSMA PET at least once.
That difference is greater than the absolute MFS benefit (when MFS is defined by either conventional or PSMA imaging) and may mean that the MFS benefit is confounded by the differential use of PSMA PET at biochemical recurrence. The extent of that confounding will depend on the comparative probability of detecting Mets at BCR using PET vs conventional imaging in the trial cohort. Would be interested in that data.
Does PROTEUS change practice? Given the above, I'm not sure the argument is there to go from RP alone (the current standard) to RP+ADT+ARPI. Will be interested in the substudy results.
#ASCO26 #radonc #medtwitter #pcsm
https://t.co/k8p6w2Lsh7
PUNCH and now PROTEUS...congratulate the investigators in a high-risk patient population with an important question, but I do not think this will be controversial if discussed with the patient.
The story of benefit of peri-operative systemic therapy for high-risk prostate cancer remains largely unchanged IMO: if electing for RP -> RP followed by selective secondary therapy when needed.
6/n #ASCO26
This is the crux of the problem, MFS by PET closely mirrors EFS, and will certainly have a STE below 0.5.
Conventional imaging:
~50% of BCR events with conventional imaging result in positive scans.
- RTOG 9202 with 15+ yr fu: RT+LT-ADT: 45% had BCR at 15yr, but only 17% had DM.
PET imaging:
>95% of BCR events with PET result in positive scans.
-POP-RT w/ 5yr fu: WPRT+LT-ADT: Every BCR correlated to a +PET finding with 6 of the 7 BCR events having corresponding DM events. You can see the KM curves are nearly identical for BCR-free survival and MFS.
@VedangMurthy@DrHowardSandler@DrMHofman@jmmrad
A really thought-provoking study at #ASCO26 (Abstr 4512, Clinical Science Symposium): decision regret after adjuvant pembrolizumab in RCC.
🔹 The question
Do patients regret receiving adjuvant pembro — and if so, is it driven by long-term toxicity that CTCAE grading doesn't adequately reflect? They built a patient co-designed tool focused on long-term toxicity.
🔹 The study
104 RCC pts post-adjuvant pembro across 3 London centres, median f/u 30 mo. Pts completed the Ottawa Decision Regret Scale alongside their own rating of irAEs as life-changing, significant, or non-significant.
🔹 What they found
28% rated their toxicity as significant and 11% as life-changing — but these ratings did NOT correlate with CTCAE grade (a third of G1–2 events were rated significant), and regret was identical for G1–2 vs G3–4 irAEs. Regret was driven by patient-perceived long-term toxicity, especially permanent endocrine and MSK irAEs — and not by disease recurrence (only 1/14 who relapsed expressed regret). Lower baseline expectations of toxicity → more regret.
🔹 My take
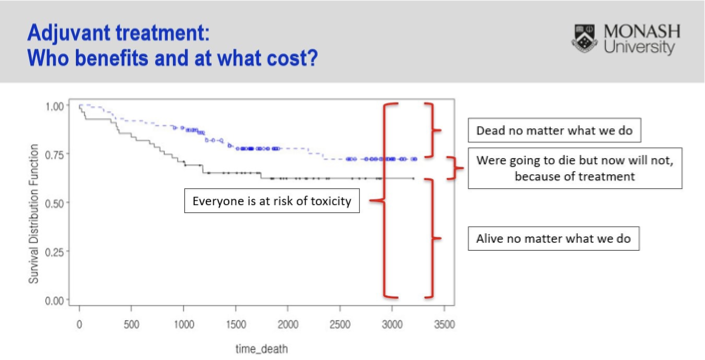
Striking that >1 in 4 reported significant and >1 in 10 life-changing toxicity. What concerns me most isn't that CTCAE missed these events — it's that the grade didn't correlate with how significant patients found them, nor with regret at all. That deviates from the very purpose of grading. The hard part: a regret analysis is tough to contextualize when the alternative, no treatment, risks recurrence — arguably worse than a long-term toxicity. Adjuvant therapy is challenging by nature: most patients are either cured already or destined to recur regardless — we expose everyone to toxicity to benefit a minority. We urgently need biomarkers to find the few who truly benefit. This slide from @Prof_IanD says it all 👇
Looking forward to seeing the presentation!
🔗 https://t.co/laVM7xBbxr
#kcsm #ASCO26
@BethN01@tompowles1
Congrats @VedangMurthy and @RadOncTMC on the publication of the BART trial, presented last Fall at @ASTRO_org AM 2025
(I can’t find a Bart Simpson emoji 🥲)
A Phase III study in high-risk bladder cancer showed that advanced IMRT based radiotherapy improved disease control and recurrence free outcomes with low severe toxicity.
#Radiotherapy#IMRT
For patients with high-risk features after cystectomy + perioperative chemotherapy: add pelvic IMRT to your armamentarium.
Locoregional control matters. It avoids painful LRRs, reduces need for (inefficient) salvage , and offers a pragmatic, safe & accessible option globally.
This trial represents a decade of work—hypothesis → design → accrual → follow-up → data lock → Presented at @ASTRO_org 2025 plenary →publication in @JCO_ASCO
https://t.co/nPBHKp9VPN
🙏 To the patients, families, clinicians, and my team: A BIG thank you.
A personal story published today in the @TataMemorial Newsletter
Radiation after Cystectomy in Bladder Cancer (the BART trial): A Timeless Problem, A Timely Solution
Read Here:
https://t.co/bchheXlCU2