@bbmdmsk@UrologyMSK@UroOnc@AmerUrological 💯! Similar to teaching TURBT with the loss of high volume TURP experience, more emphasis and intentionality on teaching open skills is needed
Great effort by all. Closely proctored course consists of:
Renal vascular isolation
Partial nephrectomy
RPLND
Pelvic vascular control
IVC and aortic vascular repair
Ureteroenteric anastomosis
Ureteral repair
bowel handling/stapling
Great learning, bonding and social interaction
This was so fun to write. BCG is an old drug but it remains dynamic--I received a draft to review in 2 weeks was already outdated because POTOMAC and ALBAN read out. This was a 💪 lift by Dr Tazegul and as always 🙏 to #MOD for his vast experience and advice. @UIowa_urology
@VigneshPackiam@saumyg We’ve 👀 this before - systemic tx PD-1 therapy in NMIBC (*cough* pembro) that DID NOT move needle. 5% DFS not compelling enough for use in patients given cost/logistics. My guess is poor utilization in real world. Bar for FDA approval needs to be higher. @US_FDA@BCAN_Research
@VigneshPackiam So much of real world NMIBC "treatment failure" is actually a logistics and delivery failure. Adding systemic IO to an already burdensome intravesical treatment schedule not going to improve any real world outcomes...need some disruption in treatment delivery!!
Glad its approved and have another treatment option!
IMO, for 5% improvement in 3y DFS (essentially only recurrence not progression), and associated >15% G3+ systemic AE, this combo does not seem useful to most pts
And we have ever growing # of well tolerated salvage tx
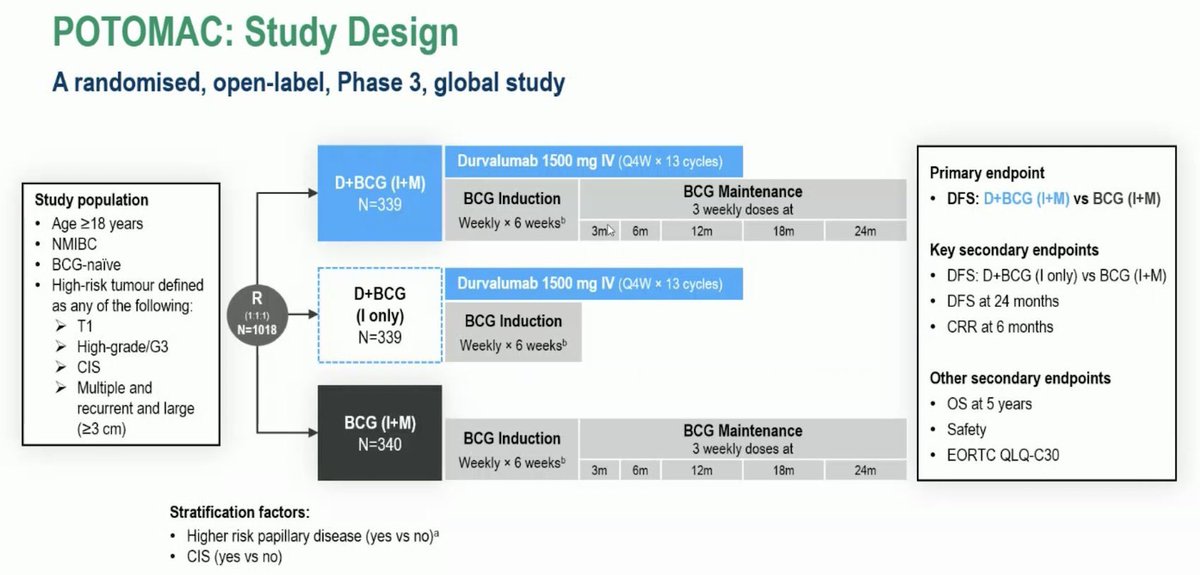
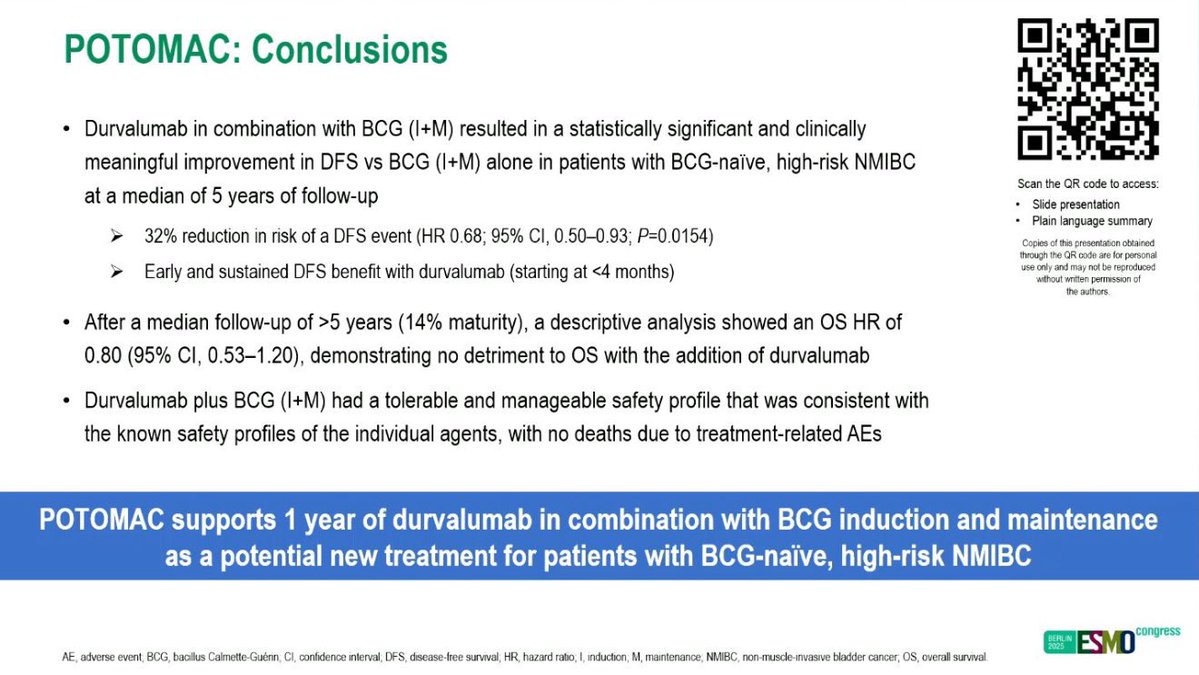
Durvalumab now @US_FDA ✅ for Non-Muscle Invasive Bladder cancer based off #POTOMAC: PhIII, BCG + Durvalumab vs. BCG alone in BCG naive HR-NMIBC:
- DFS waiting maturity (HR: 0.68)
- 3yr mDFS 82% vs 77%
- MedOncs will now see HR-NMIBC
#gusm#OncTwitter
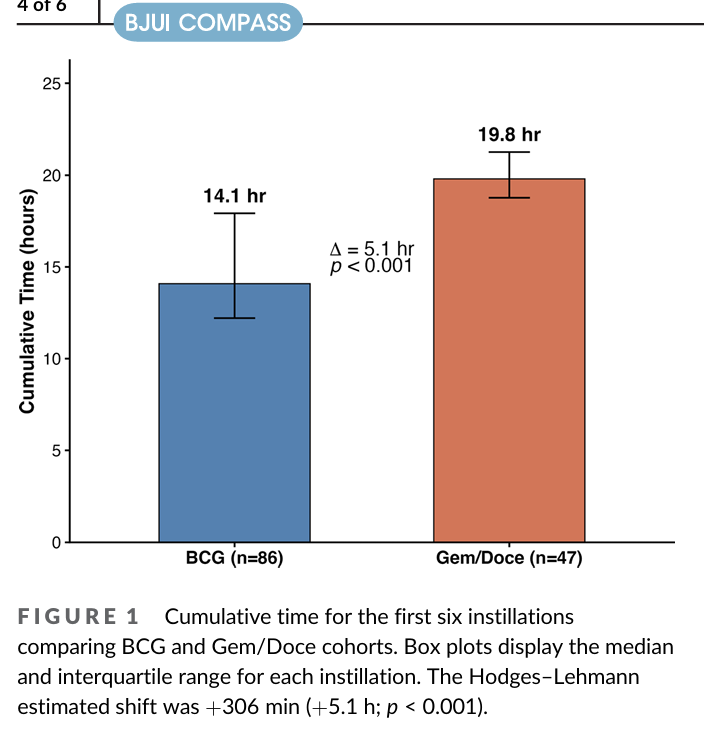
If BRIDGE shows non-inferiority (I think likely)... need to choose treatments in real world. One of main issues if Gem/Doce is logistics, especially in community.
But there is also a time burden on the patient which can impact shared decision making
https://t.co/zyzToUgypq
Really like this Cell paper from Stanford group - TURBT results in molecular clearance in 39% NMIBC. And those patients do really well. Lots of good stuff in the paper... non-molecular responders could get new agent earlier, not just maintenance BCG
https://t.co/xfpYbbZZIX
Time to revisit something I’ve been saying for years: TaHG bladder cancer is not intermediate risk. The clinical outcomes, molecular biology ... all point in the same direction.
Yet some frameworks allow < 3cm TaHG tumors to be downgraded into “intermediate risk” alongside low-grade disease.
That classification has real consequences for patients:
• undertreatment
• less rigorous surveillance
• in some studies, these patients are even placed on observation as a supposedly appropriate “control arm.”
TaHG is high risk. 🧵 @BladderCancerUS@WorldBladderCan@IBCG_BladderCA
Congratulations to @RutgersCancer and @RWJBarnabas Dr. Saum Ghodoussipour @saumyg, one of last year's award recipients of the Annual Non-Muscle Invasive Bladder Cancer (NMIBC) Research Fellowship Award, on presenting his research at the Society of Urologic Oncology @UroOnc 2026 Annual Meeting at the American Urological Association on Dynamic intra-tumor heterogeneity on non-muscle invasive bladder cancer!
https://t.co/wxs06BZOgq
#AUA26 @AmericanUrological
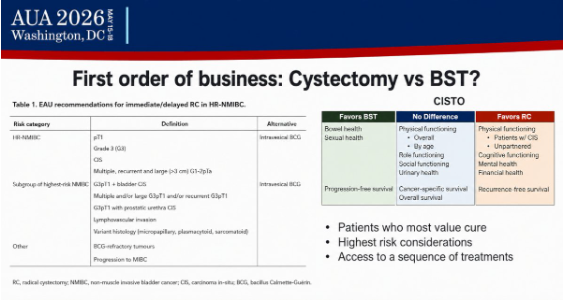
The @IBCG_BladderCA Crossfire Debates may have been some of the most practical sessions of the meeting 🔥
Some clear take-home messages emerged:
1️⃣ In perioperative #MIBC: Follow the protocol. Sandwich systemic therapy remains the SOC
2️⃣ In low-risk intermediate #NMIBC: Active surveillance and office fulguration continue gaining momentum.
3️⃣ MRI for bladder cancer staging: Promising, but still not standard of care for ALL
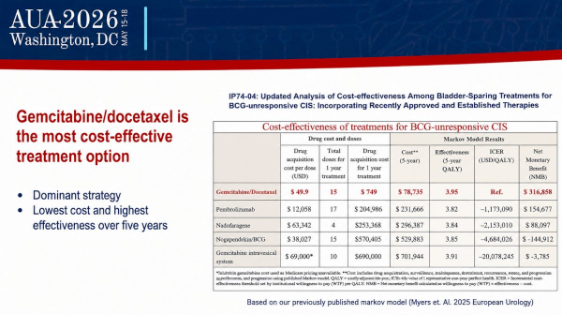
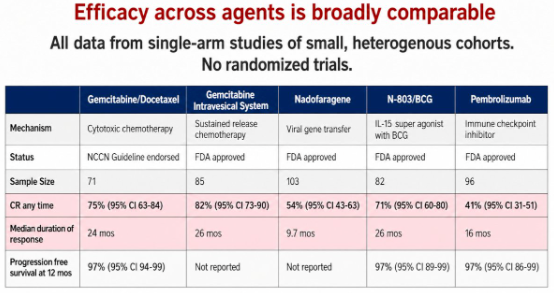
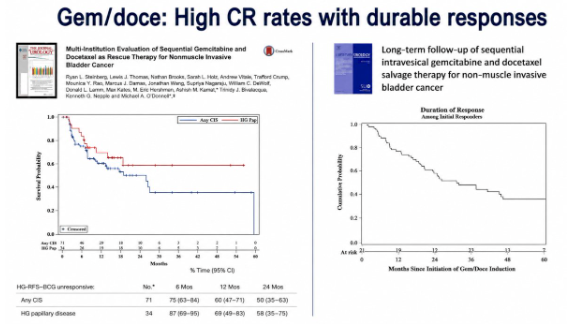
4️⃣ In BCG-unresponsive #NMIBC: GEM/DOCE remains a major benchmark bladder-sparing option.
Excellent debates, outstanding faculty, and highly practical discussions this year.
More coverage at @urotoday
Cool trial. To me these are 2 quite different regimens. Traditional Gem/Doce therapy which our data shows capitalizes on optimized drug penetration. And a dual alternating regimen - immune activation plus an element of chemo field sterilization in between. I wonder what implications it has for further line therapy but if very high CR then it matters less
Love the exploration of new combination ideas so we can more rationally optimize!
SWOG S2611 (ARCIS): a randomized comparison of intravesical therapies: a phase III study of cretostimogene grenadenorepvec/gemcitabine (CRETO-GEM) vs gemcitabine/docetaxel (GEM-DOCE) for the treatment of BCG-unresponsive and BCG-exposed #NMIBC. Presentation by @MarkTysonMD@MayoClinic. #AUA26 written coverage by @chavarriagaj@PSH_Urology > https://t.co/4UM8Imzfw9 @AmerUrological
Shout out to soon to be @SUO_YUO fellow Melinda Fu for excellent presentations on our work with intravesical therapy time toxicity and optimization! Very important to study as our treatment options continue to grow @RutgersCancer@rwjurology@BladderCancerUS
Many congrats Jacob Taylor et al on @BJUIjournal paper of the year! #aua26
Long-term outcomes of bladder-sparing therapy vs radical cystectomy in BCG-unresponsive non-muscle-invasive bladder cancer