“If you are that special lover (woo)
And love keeps you tied to another
That's the way it goes on love's train
You don't need no, you don't need no ticket to ride “
🌸 THE 10 MOST IMPORTANT BREAST CANCER TRIALS OF #ASCO26
Chicago is loaded this year.
From ctDNA-guided endocrine switching to frontline ADCs and next-gen HER2 platforms, these are the studies most likely to shape breast oncology practice 👇
🩷 HR+ / HER2- DISEASE
1️⃣ persevERA BC (LBA1006)
Giredestrant + palbociclib vs letrozole + palbociclib in 1L metastatic disease
Despite missing the primary PFS endpoint, biomarker/subset analyses may define where oral SERDs still fit.
2️⃣ SERENA-6 (LBA1007)
Camizestrant for emergent ESR1 mutations detected via ctDNA BEFORE radiographic progression
Possibly the biggest ctDNA-guided endocrine strategy discussion of the meeting.
3️⃣ VIKTORIA-1
Gedatolisib + fulvestrant ± palbociclib after AI + CDK4/6i progression
Huge unmet-need population.
Post-CDK4/6 sequencing remains one of the biggest HR+ questions.
4️⃣ lidERA BC (Abstract 502)
Adjuvant giredestrant in early ER+/HER2- disease
Moving oral SERDs into curative-intent therapy.
5️⃣ FOURLIGHT-2 (Abstract 1042)
Next-gen CDK4-selective inhibition with atirmociclib + letrozole
Can we reduce neutropenia while preserving efficacy?
🔥 TNBC & ADC ERA
6️⃣ ASCENT-04 (LBA1000)
Sacituzumab govitecan + pembrolizumab vs chemo + pembrolizumab in PD-L1+ mTNBC
Could ADC + IO combinations become the frontline standard?
7️⃣ TROPION-Breast02
Dato-DXd vs chemotherapy in metastatic TNBC
A major test of the “ADC-first” paradigm.
🎯 HER2+ & NEXT-GEN NEOADJUVANT PLATFORMS
8️⃣ KN026-004 (LBA660)
Novel biparatopic HER2 antibody vs classic CLEOPATRA-style therapy
Watch the pCR data carefully.
9️⃣ I-SPY 2.2 (LBA514)
Rilvegostomig + T-DXd in high-risk HER2-negative disease
IO + ADC combinations continue moving earlier.
🔟 DESTINY-Breast05 Update
Long-term outcomes for T-DXd vs T-DM1 in residual HER2+ disease
Which breast abstract are you watching most closely?
#BCSM #OncoTwitter #ASCO26 #BreastCancer #MedEd @asco@myesmo@esmo_open@OncoAlert@OncBrothers
🚨 HYPOKALEMIA IN ONCOLOGY – The sneaky but deadly electrolyte emergency every oncologist must master!
Hypokalemia is extremely common in cancer patients and can cause muscle weakness, paralysis, QT prolongation → Torsades, arrhythmias, and sudden death — while also amplifying chemotherapy toxicity.
This high-yield infographic covers everything:
✅ Major causes in oncology (GI losses from chemo, cisplatin-induced renal wasting, drug-induced, hypomagnesemia, ectopic ACTH, cancer cachexia)
✅ ECG progression (flattened T waves → prominent U waves → QT prolongation → VT/VF)
✅ When it becomes an emergency + practical evaluation
✅ Step-by-step management (treat cause + safe K replacement + magnesium correction is NON-NEGOTIABLE)
Key Clinical Pearls 🔥
• Hypomagnesemia makes hypokalemia refractory — always correct Mg simultaneously or K replacement fails!
• Never give IV potassium as a push/bolus — dangerous!
• KCl is the preferred salt in most oncology patients
• Platinum agents (especially cisplatin) are one of the biggest culprits
Save this for your next ward round or night call 📌
Perfect companion to the Hyperkalemia in Oncology infographic!
RT to help fellows & residents 🔥
Follow @DrRupamOncology for more high-yield Cancer Concepts Explained
#Hypokalemia #Oncology #MedTwitter #MedEd #FOAMed #Electrolytes #CancerCare #Chemotherapy #TumorLysis #FOAMed
🚨 Why Must Gemcitabine Be Administered Over 30 Minutes?
Gemcitabine is traditionally infused over 30 minutes because longer infusion times (>60 min) significantly increase toxicity — especially myelosuppression, fatigue & constitutional symptoms — without clearly improving efficacy in standard practice.
This high-yield infographic breaks down: ✅ Pharmacologic basis (prodrug → dCK activation → dFdCDP & dFdCTP) ✅ Why 30 minutes is optimal (best efficacy–toxicity balance) ✅ What happens with prolonged or Fixed Dose Rate (FDR) infusion ✅ PK concept (AUC & intracellular exposure) ✅ Common regimens & practical clinical pearl
🔖 Save this as your quick reference
📌 Share with your residents, fellows, chemo unit & oncology team!
Cancer Concepts Explained by
Dr Rupam Manna MD
Medical Oncologist
@DrRupamOncology
#Gemcitabine #Chemotherapy #Oncology #MedEd #OncoTwitter #MedTwitter #CancerEducation #CancerConceptsExplained
@Rconstantino Nossa, imagina quando você souber das roubalheiras e artimanhas do PT. Btw, você ouviu falar sobre a mudança da coordenação dos inquéritos relacionados às fraudes no Instituto Nacional de Seguro Social (INSS) só pra livrar a cara do Lulinha? Se sim, pode mudar de foco por favor?
🚨 Jaundice in a cancer patient is an oncologic emergency until proven otherwise.
From malignant biliary obstruction to immune-mediated hepatitis, rapid diagnosis and timely intervention can be lifesaving.
📌 Key focus:
✅ Obstructive vs hepatocellular vs hemolytic jaundice
✅ Cholangitis recognition
✅ ERCP/PTBD decision-making
✅ Immunotherapy hepatitis management
✅ Chemotherapy dose considerations
✅ Practical oncology algorithm for real-world practice
Early biliary decompression and sepsis control often determine outcomes.
#Oncology #MedicalOncology #Jaundice #Cholangitis #LiverMetastasis #Immunotherapy #CancerCare #ERCP #Hepatology #GIOncology #PancreaticCancer #Cholangiocarcinoma #CancerEducation #MedEd #FOAMed #DrRupamManna
🚨 FDA expands the role of Enhertu in curative-intent HER2+ early breast cancer.
AstraZeneca + Daiichi Sankyo’s trastuzumab deruxtecan is now approved in the US in BOTH:
🔹 Neoadjuvant setting (DESTINY-Breast11)
🔹 Adjuvant residual disease setting (DESTINY-Breast05)
Key data 👇
🔹 DESTINY-Breast11
Enhertu → THP vs ddAC-THP
📈 pCR:
67.3% vs 56.3%
Absolute improvement: +11.2% (p=0.003)
🔹 DESTINY-Breast05
Enhertu vs T-DM1 in residual disease
📉 IDFS events reduced by 53%
(HR 0.47)
📊 3-year IDFS:
92.4% vs 83.7%
This potentially reshapes BOTH pre-op and post-op HER2+ early breast cancer management.
But important caution:
⚠️ ILD/pneumonitis remains clinically relevant.
In DESTINY-Breast05:
• ILD: 9.6% with Enhertu
• 2 treatment-related deaths reported
Still, this is a major move of T-DXd deeper into curative-intent disease.
📖 Full details:
AstraZeneca press release
#BreastCancer #OncoTwitter #MedTwitter @OncoAlert@myesmo@esmo_open@asco
💉🩺 DEXAMETASONA EN URGENCIAS
Glucocorticoide potente y de acción prolongada con efecto:
✅ Antiinflamatorio
✅ Antiedema
✅ Antialérgico
✅ Inmunosupresor
⚙️ Mecanismo de acción:
🔹 Inhibe mediadores inflamatorios (prostaglandinas y citocinas)
🔹 Disminuye permeabilidad capilar y edema
🔹 Reduce respuesta inmune exagerada
🔹 Disminuye inflamación de vía aérea
📌 Usos frecuentes en urgencias:
🚑 Crup
🚑 Asma y sibilancias
🚑 Anafilaxia (adyuvante)
🚑 Edema cerebral NO traumático
🚑 Meningitis bacteriana
🚑 Antiemético
💡 Perlas clínicas:
🔹 La vía oral suele ser tan efectiva como IV/IM en cuadros leves-moderados.
🔹 La ampolla IV puede administrarse VO en pediatría.
🔹 NO reemplaza adrenalina en anafilaxia.
🔹 Su larga vida media permite muchas veces dosis única.
📚 Medicina práctica y basada en urgencias.
#Dexametasona #Urgencias #Pediatría #Asma #Crup #Emergencias #Farmacologia #DrSoquendo #EducacionMedica
📊 NAPOLI-1 Trial Summary | Nanoliposomal Irinotecan in Metastatic Pancreatic Cancer
The landmark Phase III study that changed second-line therapy forever.
✅ Median OS: 6.1 vs 4.2 months
✅ HR 0.67 (p=0.012)
✅ Now standard of care (NCCN & international guidelines) after gemcitabine failure
Full visual breakdown with trial design, toxicities, mechanism & clinical pearl 👇
#PancreaticCancer #GIOnc #Oncology #MedTwitter #CancerResearch
Follow for more Cancer Concepts Explained 👉 @DrRupamOncology
Rituximab – Side Effects & Administration Guide 🧬
One of the most commonly used monoclonal antibodies in lymphoma, CLL, autoimmune diseases & vasculitis.
This high-yield infographic covers everything you need:
✅ Premedication & baseline evaluation
✅ Safe infusion rates (first vs subsequent)
✅ Infusion-related reactions (highest risk in 1st cycle)
✅ Tumor Lysis Syndrome precautions
✅ Mandatory Hepatitis B screening & reactivation risk
✅ PML, hematologic, cardiac, pulmonary toxicities
✅ Practical oncology pearls & reaction management
Essential quick reference for residents, fellows, hem-onc teams & nurses!
🔖 Save this post
📌 Share with your team
Cancer Concepts Explained by
Dr Rupam Manna
Medical Oncologist
@DrRupamOncology
#Rituximab #Lymphoma #CLL #HemOnc #Oncology #MedTwitter #MedEd #CancerEducation
🚨 AstraZeneca update in bladder cancer.
Phase III VOLGA trial met its primary endpoint:
Perioperative durvalumab (Imfinzi) + neoadjuvant enfortumab vedotin (EV) significantly improved EFS in cisplatin-ineligible or cisplatin-declining MIBC. 🔥
🧪 Trial arms:
1️⃣ Durvalumab + EV + tremelimumab
2️⃣ Durvalumab + EV
🆚
🏥 Radical cystectomy ± adjuvant therapy
📌 Key takeaways:
✅ Statistically significant & clinically meaningful EFS benefit
✅ Favorable OS trend
✅ Manageable safety profile
✅ Potential perioperative option for cisplatin-unfit patients
After NIAGARA and POTOMAC, VOLGA becomes another major positive perioperative bladder cancer readout for durvalumab.
The perioperative uro-oncology landscape is changing rapidly.
📖 Full release in comment ⬇️
#BladderCancer #uroonc #MedTwitter @OncoAlert@myesmo@esmo_open@asco@AstraZe
🔬 Significance of Serum Free Light Chain (SFLC) in Multiple Myeloma
My latest comprehensive infographic on this key biomarker that has transformed diagnosis, prognosis, renal monitoring & treatment decisions in MM.
Covers everything in one visual: ✅ Basic concept & what SFLC actually measures
✅ Normal ranges + κ/λ ratio
✅ IMWG myeloma-defining event (involved/uninvolved SFLC ratio ≥100)
✅ Light-chain, oligosecretory & non-secretory myeloma + AL amyloidosis
✅ Risk stratification & prognostic implications
✅ Myeloma cast nephropathy & renal failure
✅ Rapid treatment monitoring (half-life 2–6 hrs!)
✅ Early relapse detection & practical clinical pearls
Save 📌 this as your quick reference guide!
Cancer Concepts Explained by Dr Rupam Manna
Follow for more → @DrRupamOncology
#MultipleMyeloma #SFLC #Myeloma #Oncology #HemOnc #MedEd #MedTwitter #Hematology
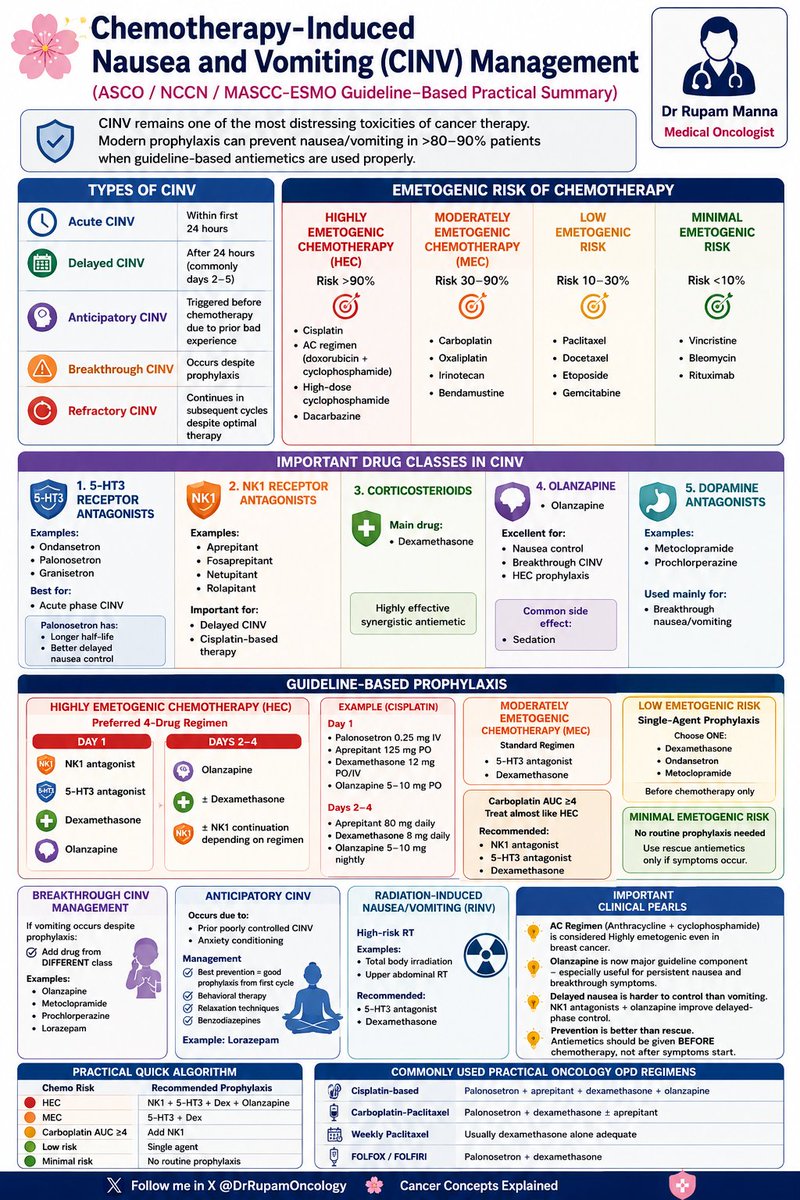
🛡️ CINV Management – ASCO / NCCN / MASCC-ESMO Guideline-Based Practical Summary
CINV remains one of the most distressing toxicities of cancer therapy…
But modern prophylaxis prevents nausea/vomiting in >80–90% patients when guideline-based antiemetics are used properly.
This infographic gives you everything in one place:
• Types of CINV (Acute, Delayed, Anticipatory, Breakthrough, Refractory)
• Emetogenic risk stratification (HEC/MEC/Low/Minimal)
• Preferred 4-drug regimen for Highly Emetogenic Chemo (incl. AC)
• Breakthrough & anticipatory CINV management
• Quick reference algorithm + clinical pearls
Perfect quick reference for daily oncology practice!
Save this infographic 👇
Share with your residents, fellows & team
#CINV #Oncology #MedicalOncology #Chemotherapy #ASCO #NCCN #ESMO #MedTwitter #CancerCare
Cancer Concepts Explained 🌸
Follow @DrRupamOncology for more such practical tools
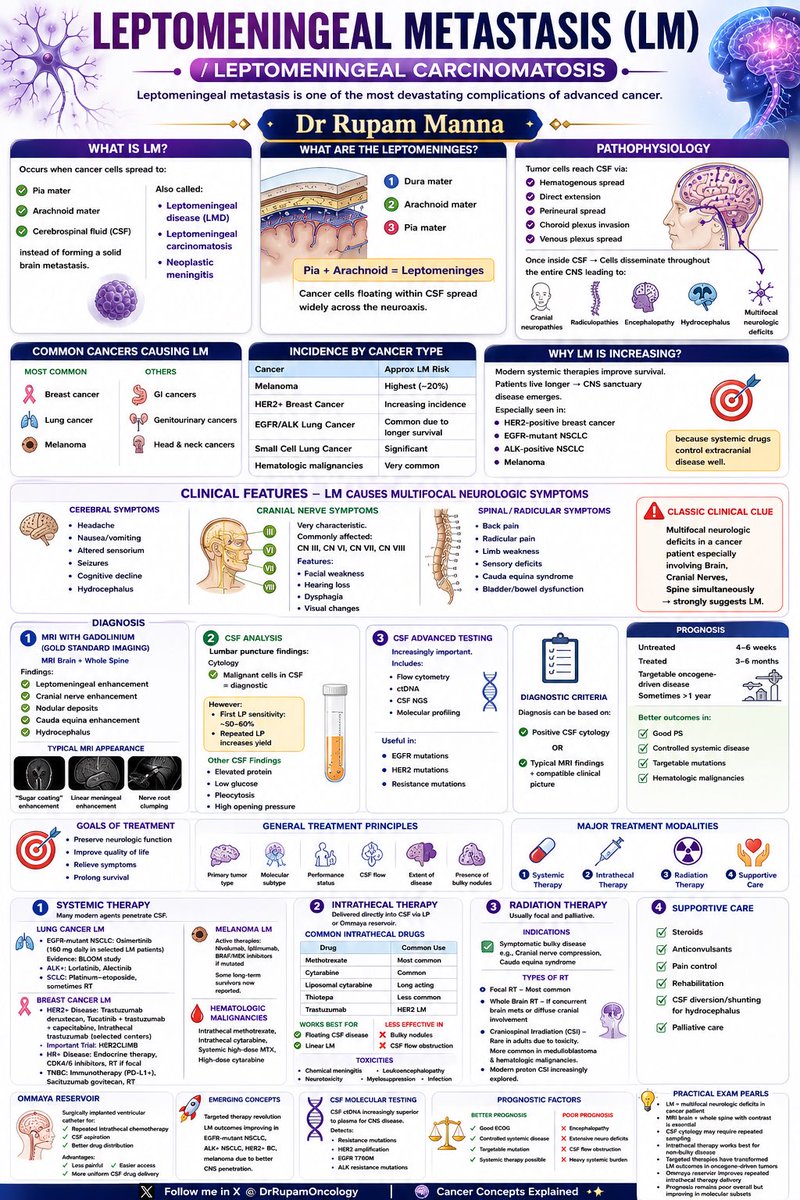
🧠 Triple IT (Triple Intrathecal Therapy) is a cornerstone of CNS prophylaxis and treatment in hematologic malignancies.
Understanding the role of:
✔️ Methotrexate
✔️ Cytarabine
✔️ Hydrocortisone
is essential in managing:
🔹 ALL
🔹 High-grade lymphomas
🔹 CNS leukemia/lymphoma
🔹 Leptomeningeal disease
⚠️ And remember:
Intrathecal Vincristine = FATAL neurotoxicity.
A must-know concept for every oncology trainee and clinician.
#TripleIT #IntrathecalTherapy #MedicalOncology #HemOnc #ALL #Lymphoma #CNSLeukemia #LeptomeningealDisease #Chemotherapy #OncologyEducation #MedEd #CancerConcepts #DrRupamManna #OncologyResident #Hematology #NeuroOncology #CancerConceptsExplained
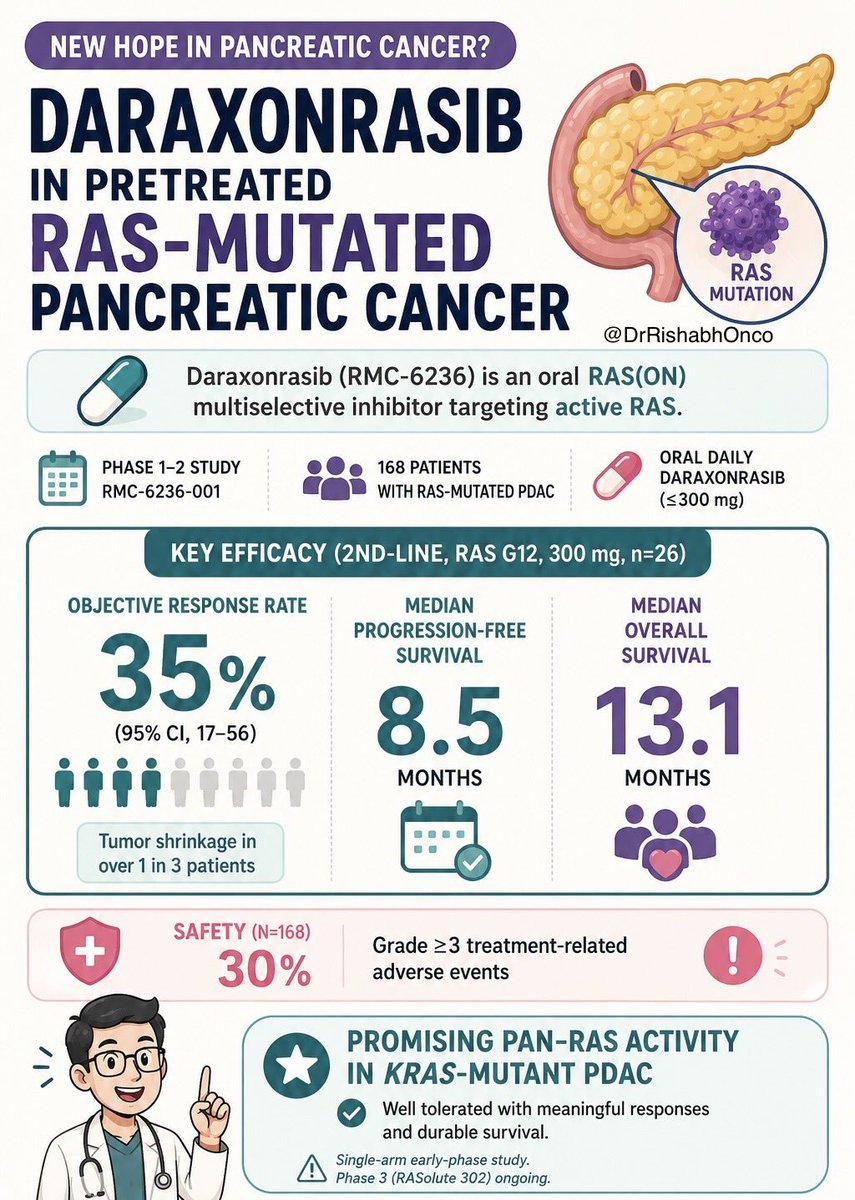
A new RAS era in pancreatic cancer?
Daraxonrasib, an oral RAS(ON) multiselective inhibitor, showed activity in previously treated RAS-mutated PDAC.
🧬 Phase 1-2 | N=168
💊 Oral daily daraxonrasib
🎯 2L RAS G12, 300 mg: ORR 35%
📈 mPFS 8.5 mo | mOS 13.1 mo
⚠️ Grade ≥3 TRAEs: 30%
Key nuance: single-arm early-phase study. Phase 3 RASolute 302 will define its real place.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #PancreaticCancer #GIOnc @OncoAlert@myESMO@NEJM