Would love to know more about how this index is constructed.
When will we see the effect of Fable? And when will we see the effect of Apple's on-device-first LLM?
We’ve been talking about this chart in @cfromhertz ‘s room. It’s fascinating to me. It’s the Token Expenditure Index and it’s available on a Bloomberg terminal. It measures the cost of 1,000,000 tokens. Let’s talk about why the index is going down.
There are actually a ton of reasons. I will highlight a few of the most important:
1) Companies and individuals are getting smarter about token use because it’s so expensive. People are creating routing systems to save money. Need to summarize something —> send to a cheap model. Need to do Deep Analytical thinking —> expensive model
2) Companies are bringing open source models in house. I’m seeing this first hand. Build a small cluster of GPUs and point your open source LLM to it. Tell your coders to use it. There are even tools like Cline that drop into VSCode to help your coders code. All of this can be in house and your tokens utilized are staying within your own network. BIG SAVINGS HERE and I think this, and #1 above, are probably the most important points.
3) LLMs are better at prompt caching. For common prompts or repetitive prompts, LLMs are caching results, thus no wasting of tokens on repetitive work.
4) Hyperscalers are selling tiered token plans where uses can get 50% off for more volume. However, this practice has been going on since 2024, so I don’t believe this one plays into it a whole lot.
5) Finally, and this one could be bearish. There are so many LLM models now. Are they competing hard with one another ultimately resulting in token costs being driven downward? Said another way, the plethora of open source models could be beginning to pressure premium models. What happens if the majority of companies choose “good enough” LLMs?
I honestly don’t know if the downturn of this index has to due with the downturn in markets. Is it a coincidence they turned down at relatively the same time?
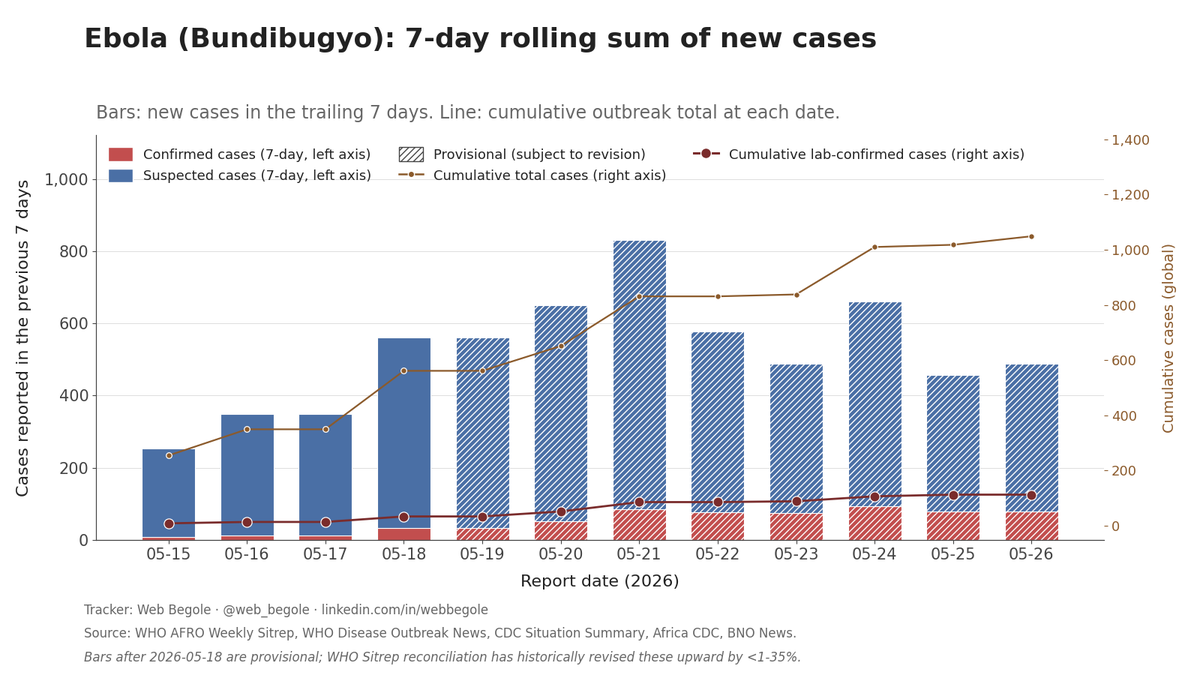
There has been a lot of changes over the past few weeks around reporting methods but now that we're focused on confirmed ebola cases it's easier to see: the situation is not improving.
@MikeZaccardi ChatGPT released November 2022. Rate hikes however started around the same time as the peak on your chart (early 2022)... The first rate hike was March 2022... Seems to fit better imo
This chart is looking encouraging, I'm hoping it's not just a lapse in reporting.
Latest update:
WHO Director-General Tedros Adhanom Ghebreyesus arrived in Bunia, the epicenter of the outbreak in Ituri Province, to meet local authorities, health workers, and affected families. "This is a difficult situation, and we recognize that. But the Democratic Republic of Congo has faced the Ebola virus many times before. We are confident that it can once again bring this outbreak under control," Tedros said after meeting with DRC Prime Minister Judith Suminwa Tuluka on Friday. He pushed back on the border closures imposed by Uganda, Rwanda, and the Trump administration's entry ban on non-US passport holders who had recently visited DRC, Uganda, or South Sudan: "Closing borders, as some countries have done, only discourages transparency."
Every year I spend two weeks around the holiday at the end of the land -- Cape Hatteras, NC -- grew up spending my summers here, It's the best mental reset I have and I always need it. I've brought many wonderful friends to join me and I've loved every moment. 🍻
Back to the grind next week, let's get it!
May 27.
Uganda ordered its border with DRC closed "with immediate effect" for four weeks. Dr Diana Atwine, Director General at Uganda's Ministry of Health, said emergency crossings for Ebola response, humanitarian operations, cargo, and security will be allowed, with anyone entering placed in mandatory 21-day isolation. The measure goes against WHO guidance, which has warned that border closures push movement to informal crossings that aren't monitored. The Uganda-DRC border runs several hundred miles and is crossed daily by families and traders. Uganda's case load stayed at 7 confirmed and 1 death.
The same day, a DRC Ministry of Health situation report (carried by Xinhua) pushed the cumulative DRC count past 1,000 suspected: 1,077 suspected cases, 238 suspected deaths, 121 lab-confirmed cases, 17 confirmed deaths across 13 health zones in Ituri, Nord-Kivu, and Sud-Kivu. DRC is also tracing more than 3,000 possible contacts. WHO Director-General Tedros called for a ceasefire in eastern DRC to allow safe access for responders, writing that "attacks on health facilities make tracking cases and their contacts nearly impossible." Congolese authorities released the first known survivor of the outbreak from a treatment center in Rwampara. The Trump administration said it plans to send Americans exposed to Ebola while abroad to a new facility in Kenya rather than to U.S. hospitals.
More here:
https://t.co/Dd2Y8yxu72
@it_is_Randy@sp3cul8r Right just highlighting the possibility.
I feel like all these models have their own personality -- things you learn you can trust them on, and things you learn you need to eyeball to be sure they're inline with your expectations -- and you can be tripped up if the model changes
@sp3cul8r@it_is_Randy There's a risk in those -- a dev that has been used to top tier models and trusting them not to make mistakes may trust the output without realizing that its a smaller model requiring more review
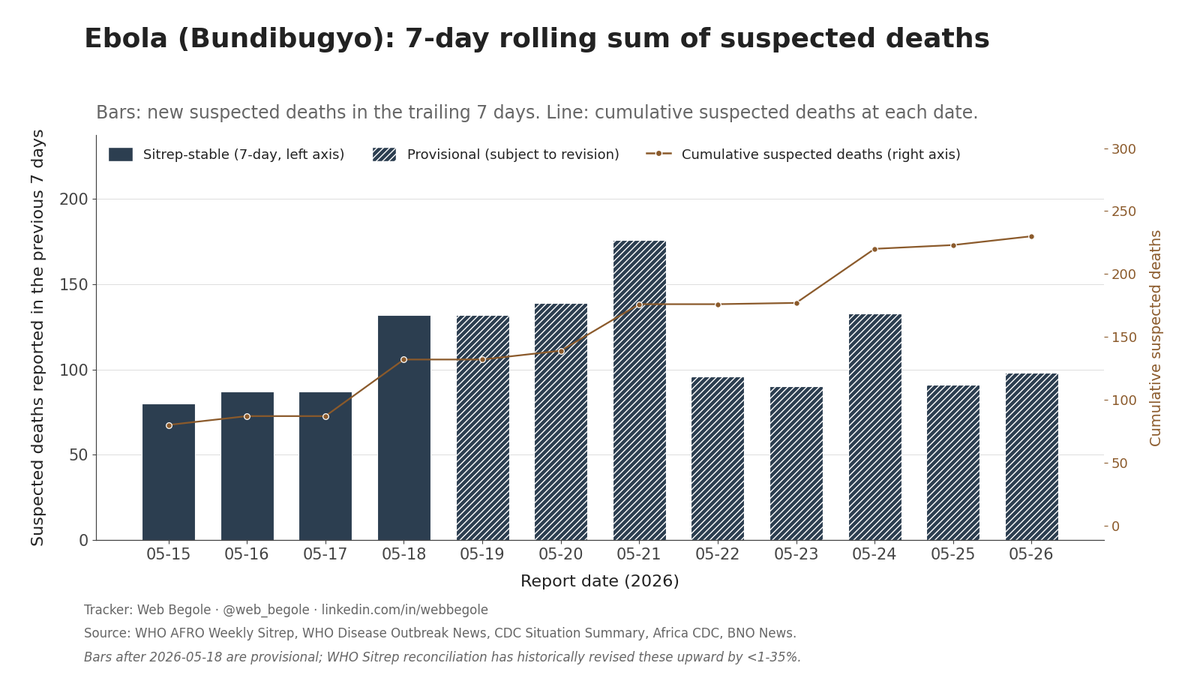
Bundibugyo Ebola in DRC and Uganda. Through May 26: 1,049 cases, 241 deaths. BNO Situation Report adds +31 DRC cases and +7 DRC deaths since yesterday. Uganda unchanged. The BNO graphic doesn't split sus and conf, so today's row attributes the growth to suspected pending WHO Sitrep reconciliation. Striped bars are residuals.
This headline is unnecessarily alarmist.
There is currently no evidence that the Bundibugyo species is somehow uniquely more infectious than other ebolaviruses.
The concern with this outbreak is not that it is a “mystery super strain,” but rather:
• no approved vaccines/therapeutics specifically for Bundibugyo
• delayed detection
• transmission in conflict-affected areas with fragile health systems
We should communicate risk accurately, not sensationalize it.