#ASCO2026 Short-Term Fasting (STF) vs Free Diet in Advanced OC (Marchetti et al.)
🎯 Objective: Insulin reduction after 3 NACT cycles
🔬Method: Pilot RCT, N=36 HGSOC on carbo/paclitaxel NACT; STF (36h pre → 24h post each cycle) vs free diet
📊 Results: Insulin Δ: −1.12 vs +9.76 µIU/mL, p=0.01
CRS 3 at ICS: 58.8% vs 17.6%, p=0.03
mPFS: 38 vs 24 mo, p=0.045
Short-term fasting during neoadjuvant chemotherapy for advanced ovarian cancer is one of the more intriguing non-drug interventions presented at #ASCO2026.
The study met its primary endpoint: fasting prevented the chemotherapy-associated rise in insulin levels and demonstrated a favorable metabolic shift.
The headline result was a PFS signal:
• mPFS 38 months with fasting vs 24 months with free diet •
HR 0.26 • Log-rank p=0.045
Before we get too excited, several important limitations deserve attention:
🔹 Only ~18 patients per arm after exclusions
🔹 Trial was powered for insulin changes, not PFS
🔹 Open-label design
🔹 Borderline statistics (95% CI 0.06–1.00; Cox p=0.056)
🔹 Multiple secondary and exploratory analyses increase the risk of false-positive findings
🔹 BRCA-mutated patients were more common in the fasting arm (50% vs 33%), which could influence outcomes
🔹 Median follow-up was only 16 months despite reporting a large difference in mPFS
🔹 Immune findings were hypothesis-generating with p-values around 0.06–0.07
🔹 Analysis appears vulnerable to selection bias from withdrawals and compliance-related exclusions
The most convincing finding is that short-term fasting is feasible and biologically active, affecting insulin and metabolic pathways.
The least convincing finding is a 14-month absolute PFS improvement from a dietary intervention in a 36-patient study.
Interesting study.
But extraordinary efficacy claims require validation in a larger multicenter randomized trial before fasting enters routine ovarian cancer practice.
@OncoAlert@ASCO #asco26
#ASCO26
📖 Concomitant publication in NEJM.
Pancreatic cancer may have just entered the RAS era. 🧬🔥
In the phase III RASolute 302 trial, daraxonrasib nearly doubled survival vs chemotherapy in previously treated metastatic PDAC. 🚨
👥 Study population:
500 patients with previously treated metastatic PDAC
91.8% had RAS G12 mutations
⚡ Daraxonrasib vs investigator’s choice chemotherapy
📈 Median OS: 13.2 vs 6.7 months
🎯 HR 0.40 (60% reduction in risk of death)
📉 Median PFS: 7.2 vs 3.6 months
🧪 ORR: 31.6% vs 11.2%
What stands out is not just the efficacy. It’s the magnitude.
An oral RAS(ON) inhibitor delivering median OS >13 months in second-line pancreatic cancer would have sounded impossible a few years ago. 👀
💬 QoL also improved:
🩹 Longer time to pain deterioration
❤️ Better global health status
🩺 Safety:
Mostly dermatologic/GI toxicities.
Grade ≥3 TRAEs were LOWER than chemotherapy (43.6% vs 57.5%).
Treatment discontinuation due to TRAEs: 1.2% vs 11.2%. ✅
Pancreatic cancer has long been the graveyard of targeted therapy.
This may finally be a turning point. 🌊
@NEJM@OncoAlert@myesmo@asco@esmo_open@AACR #OncoTwitter #MedTwitter #PancreaticCancer #RAS
The question isn’t PCS vs NACT, but who benefits from which TRUST gives us signals to sharpen that selection.
1. if redesigning the trial, exclud pts with pleural effusion/carcinomatosis from the PCS arm?
2. In truly resectable disease, PCS still shows a meaningful PFS advantage
💭 My take
67% had PFI >12mo, control mPFS 9.8mo (vs 7mo assumed).
ORR doubled but curves converged by 12mo → depth ≠ duration vs platinum + PARPi.
•PFI 6–12mo: HR 0.68 ✅
•PFI >12mo: HR 1.11 ❌
Hard to beat platinum in truly sensitive disease?
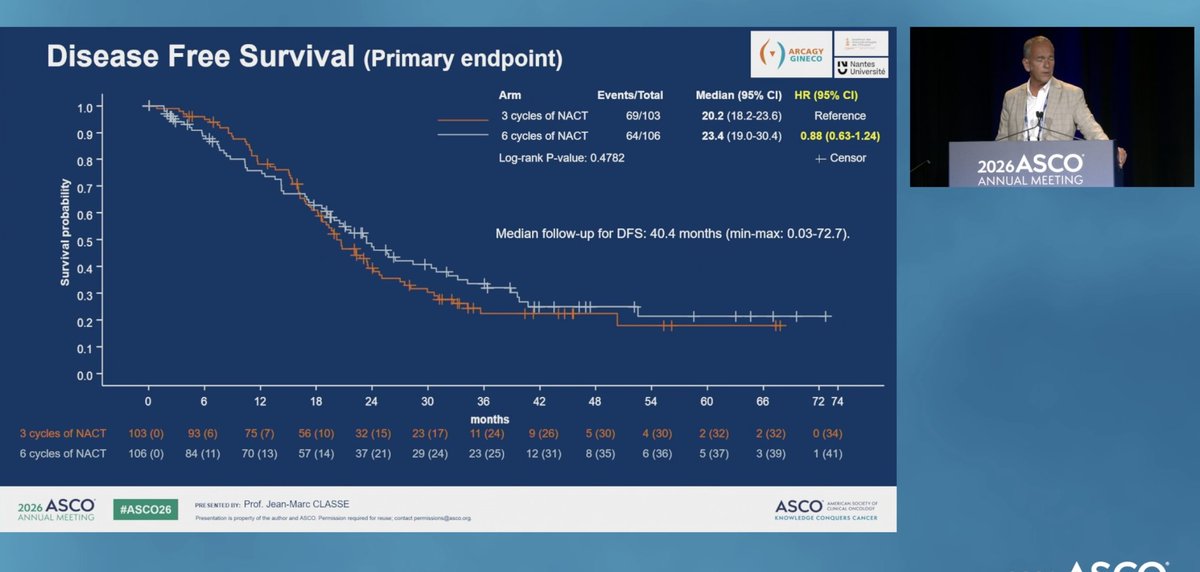
#ASCO26 Gyn Oral Abstracts #gyncsm CHRONO: A randomized ph II trial of the chronology of surgery after neoadjuvant chemotherapy for ovarian cancer. ( 3 cycles of chemo then surgery vs 6 cycles chemo then surgery.) 10% each arm HIPEC. QOL no significant difference
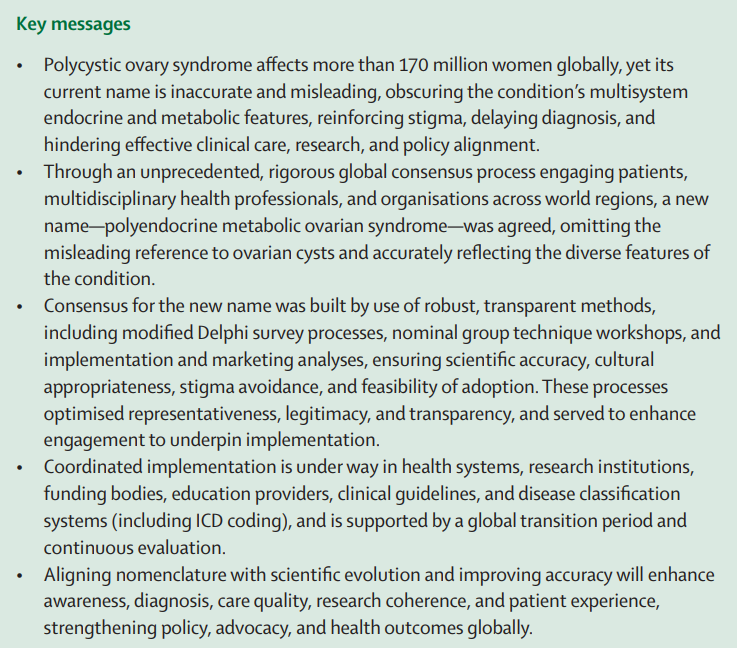
Experts reach consensus to rename polycystic ovary syndrome (PCOS), better reflecting the condition’s full health impacts.
Find out more 👉 https://t.co/Azue7YDFcn @ESEndocrinology#ECE2026
The ovarian cancer drug market
https://t.co/Fj7xf8ekXY
This new article analyses the pipeline of drugs in development for ovarian cancer, such as antibody-drug conjugates, and their expected impact on the market
🔥Two decades of PARP inhibitor synthetic lethality in cancer
🆙 @Nature
🎯BRCA–PARPi synthetic lethality: from basic discovery to approved therapies for breast, ovarian, prostate & pancreatic cancer
🎙 @IcrLordLab @Ashworth_SF@OncoAlert@Larvol
https://t.co/4EHfGJYGcf
Effects of ovarian ablation or suppression on breast cancer recurrence and survival: patient-level meta-analysis of 15 000 women in 23 randomised trials - The Lancet https://t.co/9nWVFxGIVT
A MUST-READ!
This is probably one of my most important papers where I try to teach how to fish rather than offer fish.
How I Read a Clinical Trial Report?
BG’s primer for Busy Clinicians.
Thank you @JCOOP_ASCO@EthicsdoctorP for the kind invitation. I hope the readers will find this useful.
https://t.co/HJhZlsBpU2
🚨 Anthropic's own team just showed how to actually use Claude Code properly.
30 minutes. free. the person who created Claude Code.
watch the workshop. bookmark it.
worth more than every $500 course you almost bought.
you've been using Claude without knowing 40 of its commands.
Then read the guide below.