An easy NEJM image challenge today - endoscopic findings of the oesophagus in a patient with coffee ground vomiting. These were the findings on admission (top row) and one week later (bottom row). What’s the name of this syndrome?
ASN has released the program this year's #KidneyWk and I always thought they should lean into controversy, but this is going over the line.
A cage match?
Bare knuckle boxing?
Considering non-myopathic causes of elevated CK before initiating an extensive neuromuscular workup is essential for diagnostic efficiency, patient safety. Up to 1.3% of the general population exhibits asymptomatic or oligosymptomatic hyperCKemia, #eular2026#london#autoimmune
An HbA1c of 6.4% does not ALWAYS mean Prediabetes (as shown in this case)
A patient underwent routine testing.
🔹 HbA1c: 6.4%
🔹 Hemoglobin: 7.5 g/dL
🔹 MCV: 75 fL
🔹 MCH: 20 pg
At first glance, many would label this patient as having prediabetes. But that conclusion may be wrong.
1/n
Esmolol, a short acting cardio-selective Beta-1 adrenergic antagonist, is one the common drugs used for:
-rate control in SVTs
-hypertensive emergencies
-aortic dissection
-thyrotoxicosis
and in the Perioperative period as a hypotensive agent.
It is given as boluses/ continuous infusions, at well defined rates of 150-1000mcg/kg/min.
One needs to understand that Esmolol is hydrolysed by RBC and Plasma non-specific esterases, into acid metabolites (1/1500 times potent as esmolol) and METHANOL. Both the products are excreted by renal routes.
The methanol produced is barely closer to toxicity thresholds. But, on prolonged continuous infusions, accumulation of methanol can result in toxidrome of it's own.
It isn't very common occurrence and only anecdotes are all we have now, but, unexplained metabolic acidosis with High anion and Osmolal gaps in a patient on continuous infusion of ESMOLOL should probe you to think of its metabolite: METHANOL.
Sources:
1.https://t.co/gMuusvIcJ2
2.https://t.co/1oLxnvKkPo
I'll start- the neutrophil/lymphocyte ratio (NLR) substantially outperforms the WBC for detection of infection
using WBC as an indicator of infection made sense 50 years ago. we have better instruments & its time to move on from the WBC
more on NLR here: https://t.co/unXP991e7p
@PulmCrit A fun exercise to do with a CBC is to show people the counterintuitive fact that most of their 35 trillion cells are RBCs.
Normal RBC count = 5 million / uL
= 5 billion / mL
= 5 trillion / L
5 trillion RBCs/L * 5 liters = 25 trillion RBCs
25 / 35 = 71% of your cells are RBCs
How I perform informed consent in oncology!
1.Discuss diagnosis
2.Natural course of disease without treatment
3.Treatment options (pros/cons)
4.Explore patients opinions on above
5.Make treatment recommendation, explain why (integrating #4)
6.Toxicities
7.Ask patient to explain in own words
8.Document
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
Eyelid myokymia: benign fasciculation of the orbicularis oculi, a clinical diagnosis
An isolated 10-minute episode does not require hospital admission for MRI Brain and Neurology consult.
Reassurance is the treatment of choice 👍
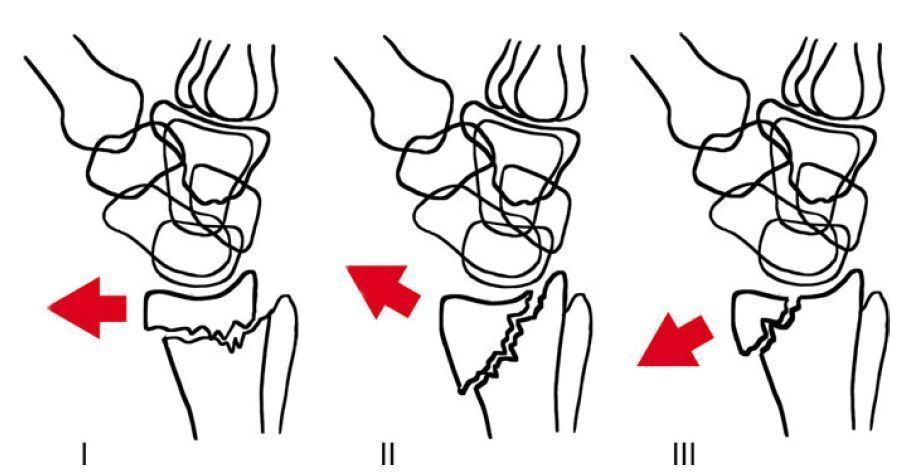
Smith’s Fracture Classification
Type I: Extra-articular
Type II: Intra-articular, involving the dorsal joint surface
Type III: Intra-articular, entering the radiocarpal joint (volar Barton’s)
Never forget B12 deficiency can cause a pseudo TMA that mimics TTP.
I just saw a case!
Rapidly progressive thrombocytopenia
Schistos
Elevated LDH
Hints it’s B12 deficiency include leukopenia and and hyperseg PMNs
Fortunately it’s an easy fix and fire up the B12