Excited to share our paper, now out in @JACCJournals! Important work led by @MAlvarezVillela:
🔥 Fever in AMI-CS is common and is associated with greater illness severity but seems to be noninfectious in most cases
#CardiogenicShock 🫀
https://t.co/d13b93sEhx
Very interesting from @GreggWStone
Makes sense intuitively - more ischemic time on an already stunned myocardium, elevating EDP, contrast delivery etc...
Non-shock doesn't necessarily mean patient is "stable".
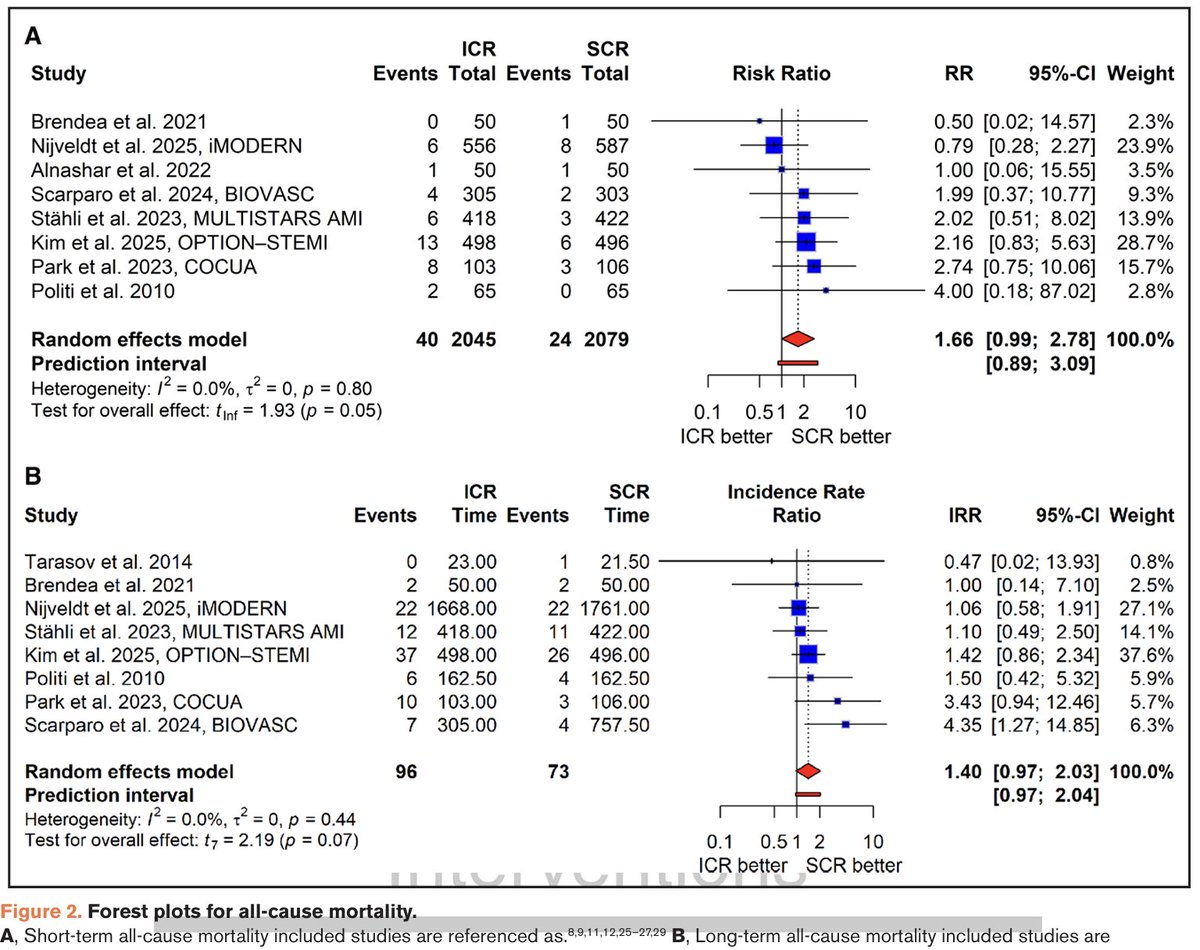
Complete revasc (CR) in pts with non-shock STEMI and multivessel ds. reduces MACE. But is the best timing for non-culprit lsn PCI immediate (during primary PCI) or staged? Our new meta-analysis publ in Circ CV Interv suggests immediate CR may increase mortality, same as in shock.
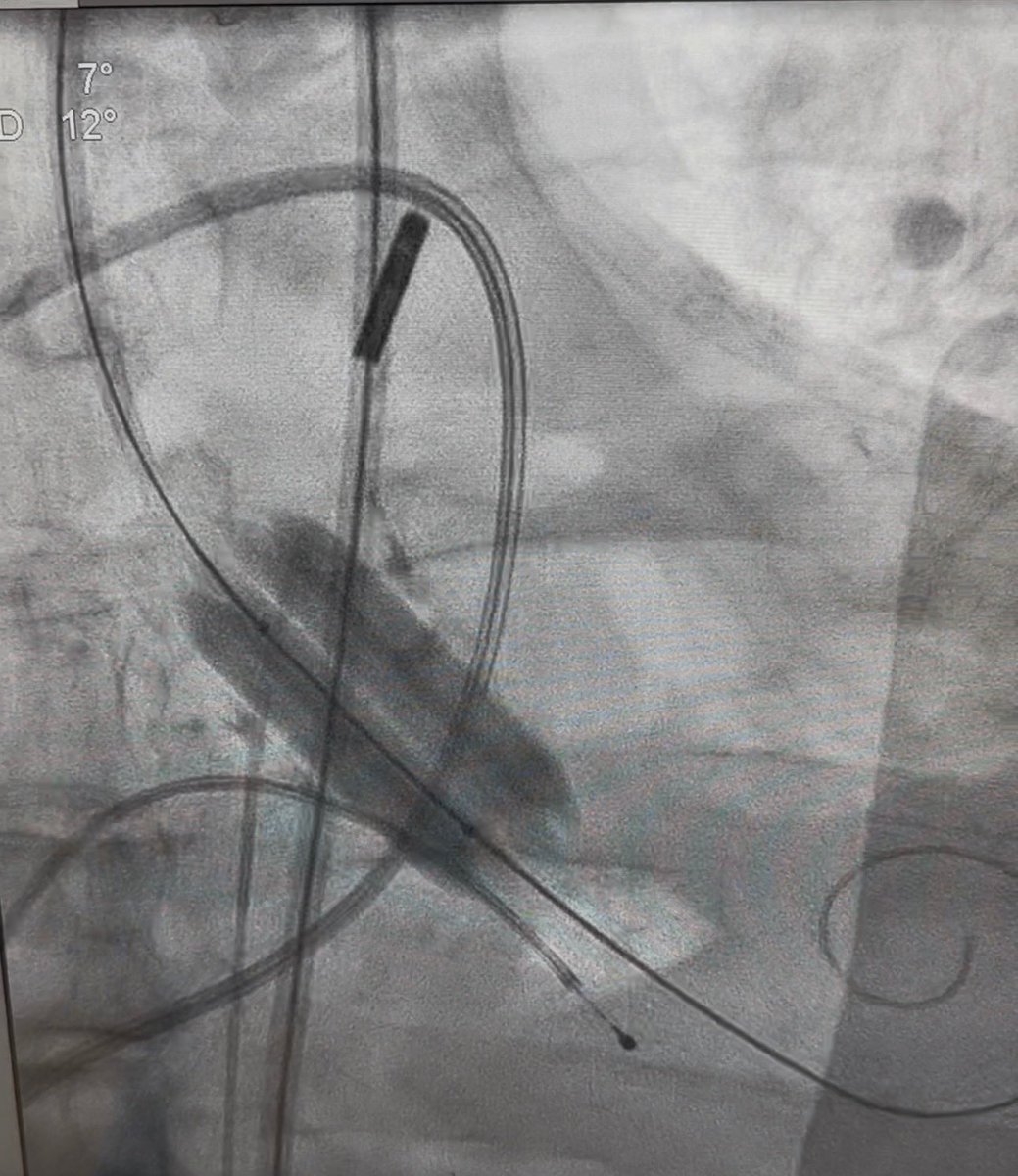
@SaidAshrafMD Prob eruptive nodule w/ thrombus, TIMI 3 is reassuring. (IABP & bring back also reasonable)
Would’ve wired that 📐 w/ 120 SC, tried 🎈(NC/Cut/IVL) first for atherotomy as primary Ca mod. OCT here.
Limit atherectomy w/ eruptive nodules to avoid no reflow, but Rota 1.5 if needed
@AdityaMandawat DES for sure. Long term outcome with covered stent will be poor.
DAPT - standard duration should be fine, after which I’ve done P2Y12 monotherapy over aspirin (which is becoming my standard as of late)
Had a similar case a few months back:
2/
Piling on to finish the call weekend:
Acute stent thrombosis of metal jacket LAD done a few days prior. With double layer in the prox
SCAI D AMI cardiometabolic shock
Multiple aspiration, repeated PTCA, distal vasodilators, MCS, lots of drugs
Very tough thrombus burden
What a Christmas 🎄 call
VT/electrical storm needing #ECMO
Valvular #cardiogenicshock needing salvage BAV
Mid LAD #STEMI w/ critical LM bifurcation disease
Tamponade w/ hemorrhagic effusion
& a CCU that has not let up, all during a snowstorm!
Wouldn’t have it any other way 🙏🏽
Last weeks complex case:
60s, dilated CDM (LV 6.8cm, EF 20%). P/w refractory angina, limited meds due to low BP on GDMT
Not sick enough for transplant yet (ambulatory, CI 2.5, on oral 💊). Surgical turndown due to risk
🫀team➡️ PCI for QOL/angina
How would you approach? #CHIP
3/
Ostial LM CSA - 3.2, severe dampening. 7Fr w/ SH, single access w/ tMCS
Wiring was tricky! Took an XTA & was able to wire into a septal off the aneurysm, then direct down to LAD
Up-front Rota 1.5 through LM -> mid LAD,
IVUS sized DESx2 mid LAD to Ostial LM. (Bumper wire)
@flatspin000001@brian_is_tired@PERTConsortium@InariMedical Apologies for the OP not being clear: this is an interventionaly approach to PE treatment - mechanical/suction thrombectomy using a large bore aspiration device @InariMedical. There are many available for use. Safety profile is excellent.
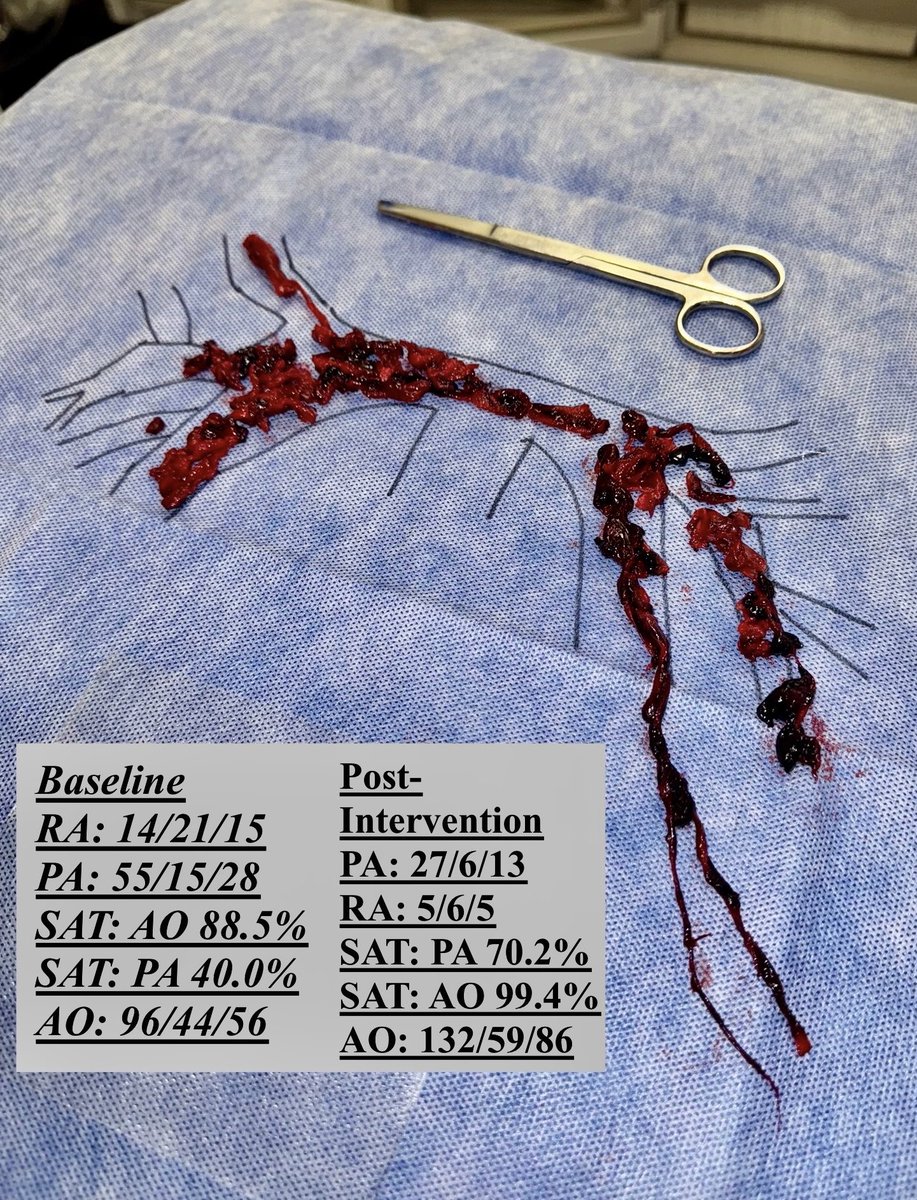
High risk PE on call last night🫀p/w syncope & ⬇️ BP
Heavily impacted bilateral PE w/ saddle, RV/LV 1.6. Opening hemos c/w normotensive shock (on inotropes CI 1.4). MCS on standby.
Immediate response to thrombectomy.
POD1 - walking, normal RV fxn on TTE.
#PERT@PERTConsortium
@Miazolam@Jonathan_PaulMD@PERTConsortium@InariMedical Unless its a true salvage situation, if there is a PE operator/cath lab available high-risk PE should be treated w/ intervention. Original data for lytics is shaky at best, w/⬆️ adverse events. Modern data for thrombectomy in HRPE is excellent both for mortality benefit & safety
@AlsaeediAlawiS@DrJayMohan@PERTConsortium@InariMedical I think the main scenarios 1) salvage hemodynamic state intra-procedurally, 2) actively coding/peri-arrest
If the RV is well into its spiral, then hemodynamic stabilization w/ MCS should be considered first
@jaygirimd and @GoldbergJBCTMD have given excellent talks on this
@jaygirimd@pritish_iyer@PERTConsortium@InariMedical 100% agree! Important data on the horizon.
We enroll as many as possible at our center when we’re involved in studies, & our research coordinators do a great job assist in that at all hours. Still a challenge.
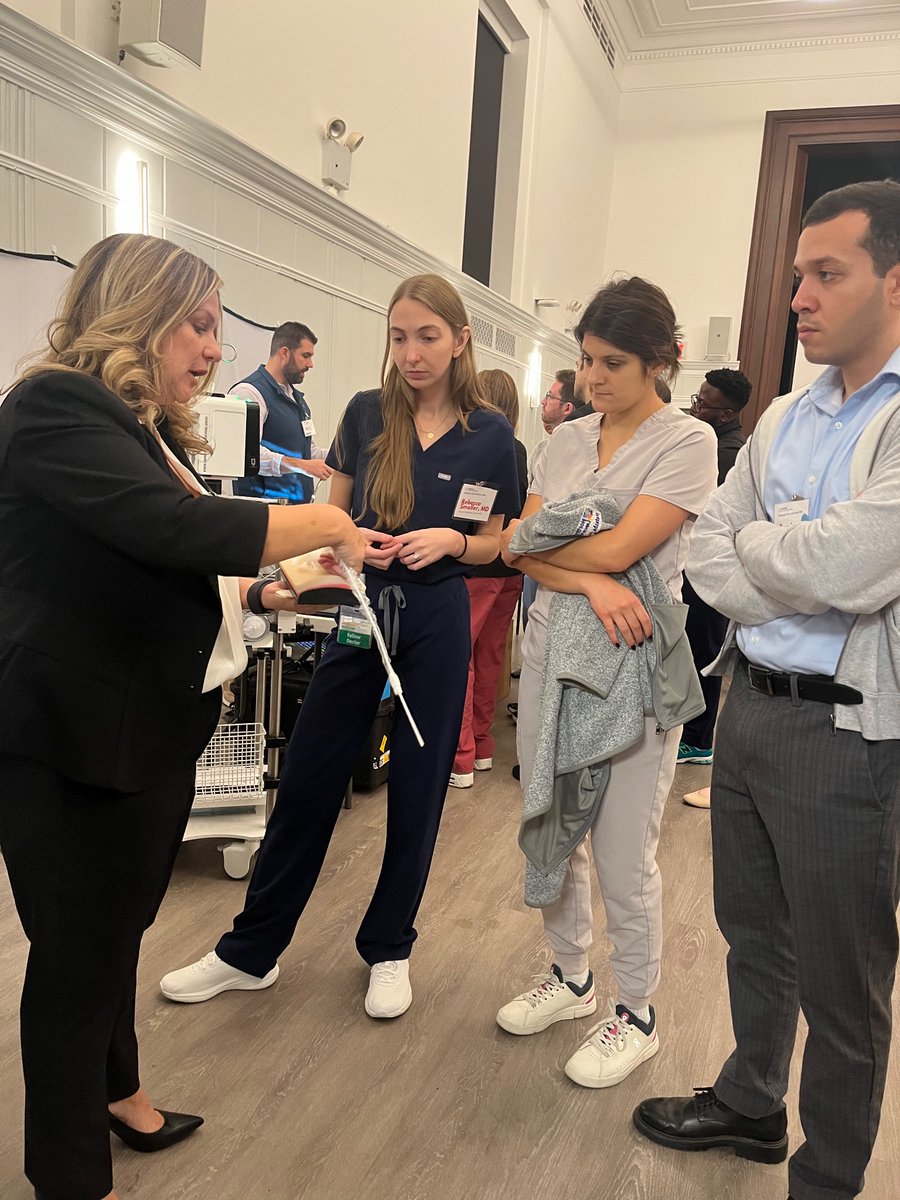
This week we hosted the first edition of the Northwell Cardiogenic Shock Skills day. Over 50 junior faculty members and fellows from cardiology, IC, CTS & CCM joined a day of hemodynamic simulations, hands-on tMCS and PAC learning and expert discussions of real-life CS cases.












![AHAScience's tweet photo. Key updates to this guideline include:
➡️ The use of the American Heart Association PREVENT-ASCVD equations to guide primary-prevention and lipid-lowering therapy decisions.
➡️ Testing Lp(a) at least once in a lifetime and selective apolipoprotein B measurement to improve risk assessment and guide treatment
➡️ The return of LDL-C and non-high-density lipoprotein cholesterol treatment goals (with lower targets for higher-risk groups)
➡️ Expanded use of coronary artery calcium scoring to reclassify risk[ME1.1]
✍🏼 @rblument1 @tygluckman @RonBlankstein @PamelaBMorris @pnatarajanmd @AnnMarieNavar @SethShayMartin @APRN_CNS @nyulangone @DrMichaelShapir @kgradneyrd @eugeniagianos @virani_md @KellieMcLain1 @ijeomaheartdoc @SamiaMoraMD @DrHeatherJohn @dmljmd](https://pbs.twimg.com/media/HDPXv0SXsAIEPMD.png)