Thoracic Medical Oncologist, Assistant Professor @MayoClinic AZ ☀️ Specializing in solid tumor cellular therapies, phase 1 trials, lung cancer 🫁 Views my own
Very good read @JTOonline Moving more towards forgoing the term "carcinoid" and recognizing NET G3 as an entity!
@OncoThor#NET#Carcinoid
https://t.co/nDnP2s8uV3
We spend time explaining staging, mutations and treatment options.
Patients retain ~30% of it. This one-page visual from LCRF does a lot of the heavy lifting for patients and family.
Tools like this should be standard in every thoracic oncology practice.
@lcrf_org@OncodailyLung@Lung_Cancers@YoungLungCancer@lungoncdoc
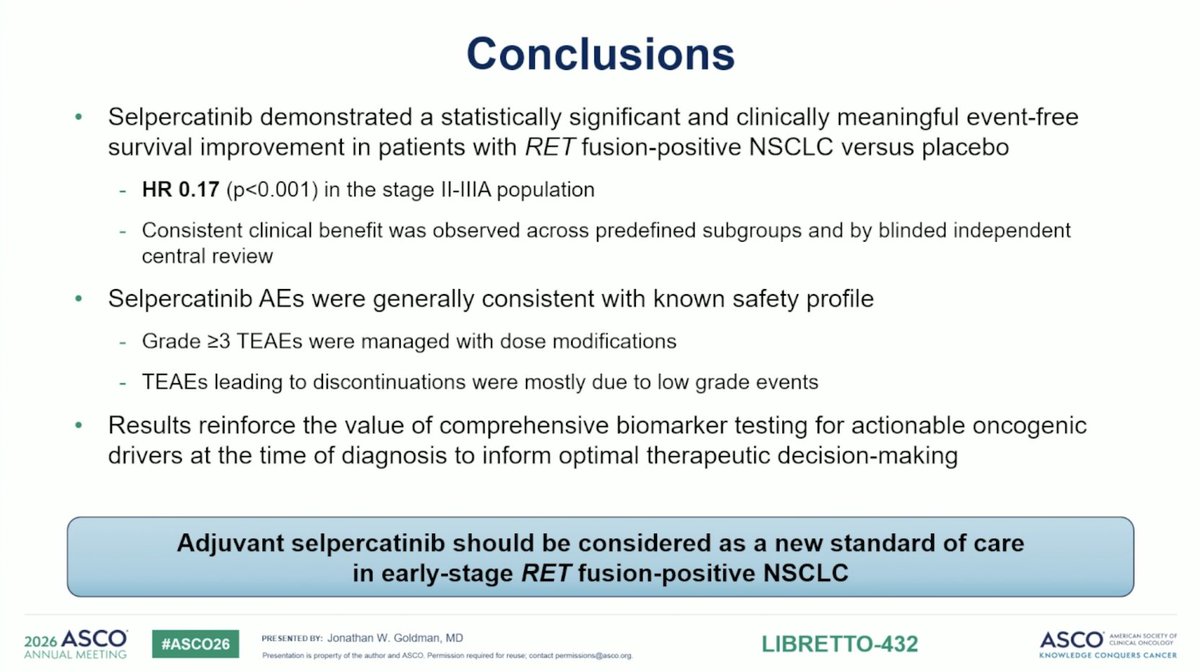
#ASCO26 AEs as expected; most common was LFTs. Rate of discontinuation of selpercatinib was 17% - would value granularity as to specific AE that led to discontinuation. Overall - fits the expected paradigm set by ADAURA and ALINA and sets new standard of care effective now.
1/2 🚨 @OncoAlert Now Live!
My coworkers & I are excited to share this just published review article @JCOOP_ASCO on:
✅Cellular Therapies in Solid Tumors
https://t.co/MMOICciNgy
2/2 ✅ We provide a practice-oriented framework for understanding emerging ACT platforms, clinical data, toxicity considerations, and implementation strategies relevant to contemporary solid tumor oncology care.
🚨 Live in Clinical Lung Cancer!
Neoadjuvant Chemoimmunotherapy in Resectable NSCLC with PD-L1 Expression <1%: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials #lcsm#nsclc#lungcancer
https://t.co/EzbiSGkrhv
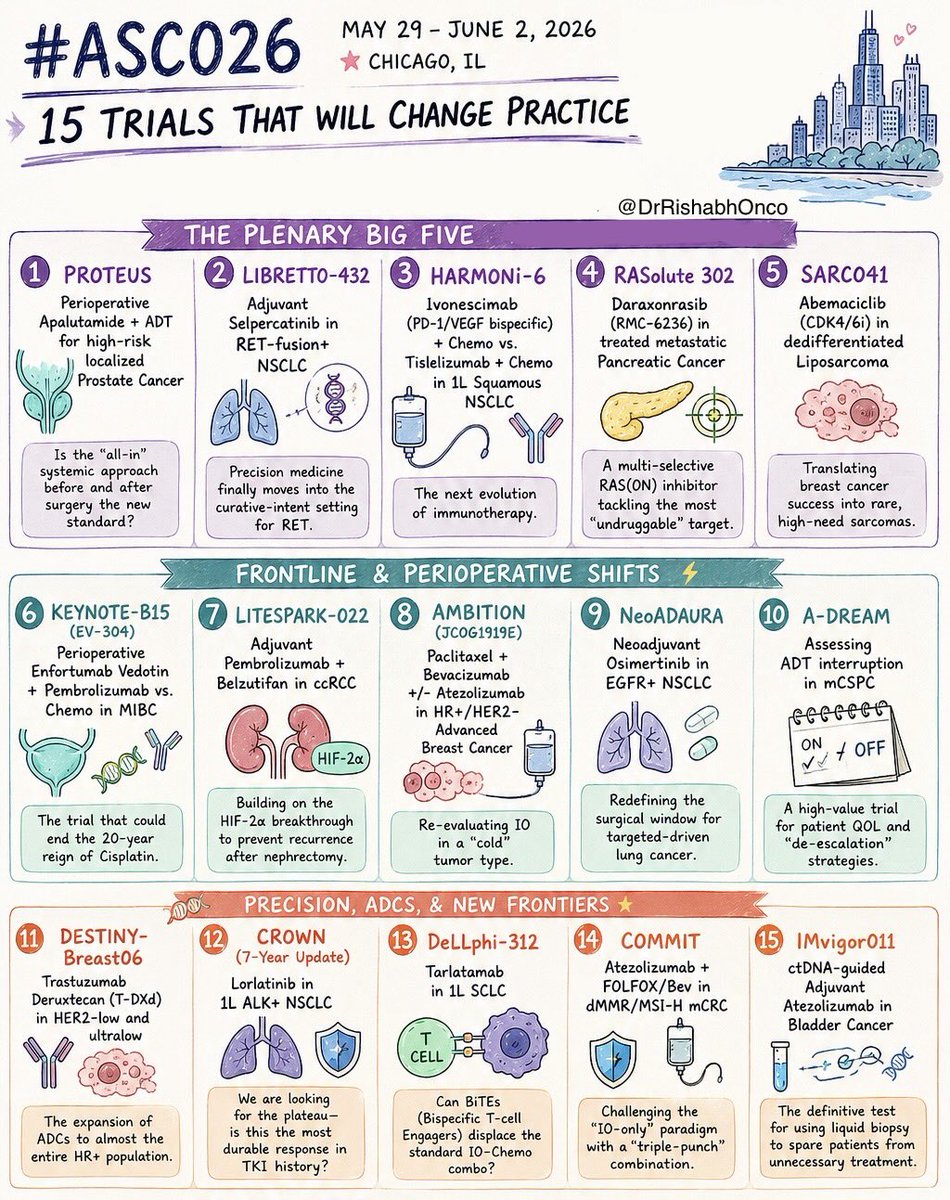
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26
May 29 - June 2 | Chicago
Which trial are you watching most closely?
🌟 PLENARY GAME-CHANGERS
1️⃣ PROTEUS
Perioperative apalutamide + ADT in high-risk localized prostate cancer
2️⃣ LIBRETTO-432
Adjuvant selpercatinib in RET+ NSCLC
3️⃣ HARMONi-6
Ivonescimab + chemo vs tislelizumab + chemo in squamous NSCLC
4️⃣ RASolute 302
Daraxonrasib (RMC-6236) in metastatic pancreatic cancer
5️⃣ SARC041
Abemaciclib in dedifferentiated liposarcoma
⚡ FRONTLINE & PERIOPERATIVE SHIFTS
6️⃣ KEYNOTE-B15 / EV-304
EV + pembrolizumab vs chemo in MIBC
7️⃣ LITESPARK-022
Pembrolizumab + belzutifan in adjuvant ccRCC
8️⃣ AMBITION
Paclitaxel/bevacizumab ± atezolizumab in HR+ breast cancer
9️⃣ NeoADAURA
Neoadjuvant osimertinib in EGFR+ NSCLC
🔟 A-DREAM
ADT interruption strategies in mCSPC
🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY
1️⃣1️⃣ DESTINY-Breast06
T-DXd expands into HER2-ultralow disease
1️⃣2️⃣ CROWN (7-year update)
Lorlatinib durability in ALK+ NSCLC
1️⃣3️⃣ DeLLphi-312
Tarlatamab in frontline SCLC
1️⃣4️⃣ COMMIT
Atezolizumab + FOLFOX/Bev in MSI-H mCRC
1️⃣5️⃣ IMvigor011
ctDNA-guided adjuvant atezolizumab in bladder cancer
#OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert@ASCO@JCOPO_ASCO@OncBrothers
🔥Non-invasive profiling of the TME with spatial ecotypes (SEs)
🆙 @Nature
🎯SEs recoverable from plasma cfDNA
🎯Outperform TMB & PD-L1 for ICI outcome prediction
🎙Dr. Wubing Zhang @AaronNewmanLab#LiquidBiopsy@OncoAlert@Larvol
https://t.co/v8MwR5K3L8
Real world analysis of tarlatamab in SCLC (n=27) @JCOPO_ASCO: RR 18%, PFS 5.9m. Signs of CNS activity: in 14pts with brain mets, 2 CR & 1 PR; in 4pts with no baseline mets, none had new CNS mets. C1D1: CRS in 37%, ICANS in 30%. C1D8, CRS 40%, ICANS 16%.
https://t.co/nNlIBVhOqg
A MUST-READ!
This is probably one of my most important papers where I try to teach how to fish rather than offer fish.
How I Read a Clinical Trial Report?
BG’s primer for Busy Clinicians.
Thank you @JCOOP_ASCO@EthicsdoctorP for the kind invitation. I hope the readers will find this useful.
https://t.co/HJhZlsBpU2
Valioso y bello testimonio de una doctora en la revista JAMA.
La autora, sana, no fumadora y con una vida estable, es diagnosticada inesperadamente de cáncer de pulmón. Eso rompe prematuramente la percepción de control que tenía sobre su vida. La enfermedad introduce de forma concreta la posibilidad de morir y, sobre todo, de no ver crecer a sus hijos. Asimismo, reflexiona sobre cómo la medicina, al fomentar el sacrificio, posterga la vida personal y normaliza así una existencia de agotamiento.
Creo que cuando la enfermedad irrumpe en el cuerpo desenmascara nuestras verdaderas prioridades. El testimonio de esta doctora pone de manifiesto, con una claridad poco común, que la medicina puede dar sentido, pero no puede sustituir la presencia. Cuando la finitud se hace presente -y deja de ser abstracta-, lo que más importa ya no se aplaza. El tiempo, al revelarse finito, hace que la vida deje de ser prorrogable. Entonces se ha comprendido que el trabajo, cualquier trabajo, por vocacional que sea, no es el hogar
🔥🚨@OncoAlert Hot Off The Press.
Just published @NEJM
Results of #FirstLine Cohort in #Beamion LUNG-1 phase 1a/1b of:
⭐️#Zongertinib
(#Oral, irreversible, #HER2#TKI) for:
🔵#Patients with advanced #HER2-mutant non-small- cell #LungCancer (#NSCLC) with no prior #Treatment.
✅#RR: 76%
✅#mDOR: 15.2 months
✅#mPFS: 14.4 months
#FDA approved in #1st line in Feb 2026
👇🏻
https://t.co/s2obTLMtlu
Transformed small cell… best practices below by Dr Carl Gay
🔵1L platinum etop + osi
🔵2L if DLL3 greater than 50% consider tarla + tki, if less , consider lurbi osi
Most important message - consider a trial here! This space is in dire need of support !
Key takeaway:
There is massive support for AI integration in MedEd and clinical practice, BUT perceptions vary wildly. Physicians have significantly fewer concerns than nonphysicians (P=.002). To succeed, AI must strengthen patient care, not burden it! 📊
https://t.co/sXo5TgV0rr
As a heme/onc fellow starting my training at Mayo Clinic in 2003, I saw a lot of patients with myeloma. I had melphalan and prednisone, thalidomide and some other marginally active but toxic stuff in my toolbox.
I had my spiel ready for every new patient I saw. It was a sad and short spiel for many. At the end of my training in 2007, we had lenalidomide and bortezomib and some exciting things on the horizon. My spiel had changed and there was hope.
Fast forward to 2026. Unbelievable!
This has not just been observed hematology but also some parts of oncology such as NSCLC and melanoma. We GI oncologists have lots of work to do to catch up but we sure are trying...
What REALLY makes a good oncologist? in @JCO_ASCO
After 10 years and 203 JCO essays, one thing became clear: expertise alone isn’t enough.
Patient-centered care.
Clear, authentic communication.
Emotional intelligence.
And the harder work
Showing up again and again.
Openness to uncertainty.
Carrying the burden of cancer care.
Continuous growth.
Clinical competence is expected
Human connection makes the difference.
Science treats disease.
Presence treats fear.
https://t.co/g9hGjSLpGu @OncoAlert