In Atrial Functional MR can get “Hamstringing”of posterior MV leaflet due to massive LA dilation;this “atriogenic” leaflet tethering is from displaced posterior annulus onto crest of LV inlet resulting in⬆️in annulopapillary distance restricting leaflet motion #echofirst
atrial functional mitral regurgitation📝
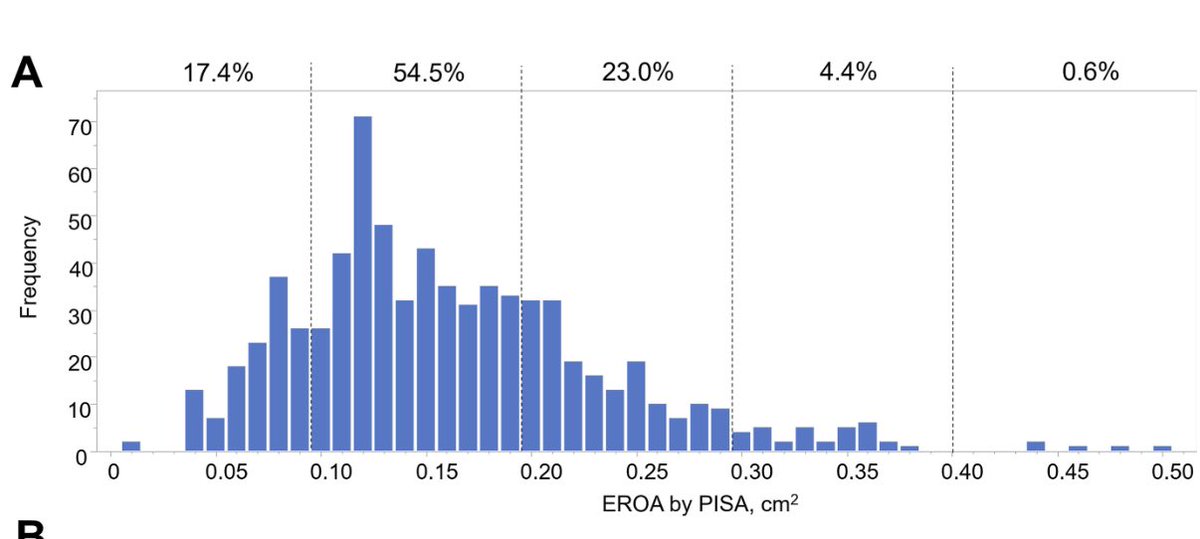
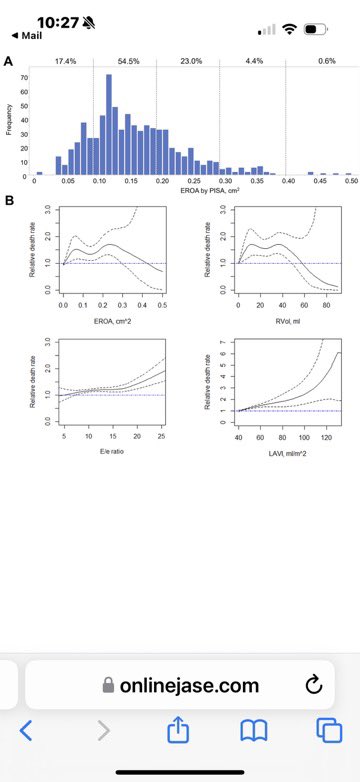
🔺Diastolic dysf, E/e′ ratio & LAVI ≥ 40 mL/m2 assoc w⬆️☠️not EOA
🔺AFMR presence more prognostic than EROA severity
🔺AFMR EROA orifice shape elliptical underestimates severity
🔺2/3 of pts w mod or >AFMR had AFib https://t.co/triYxKmfy1
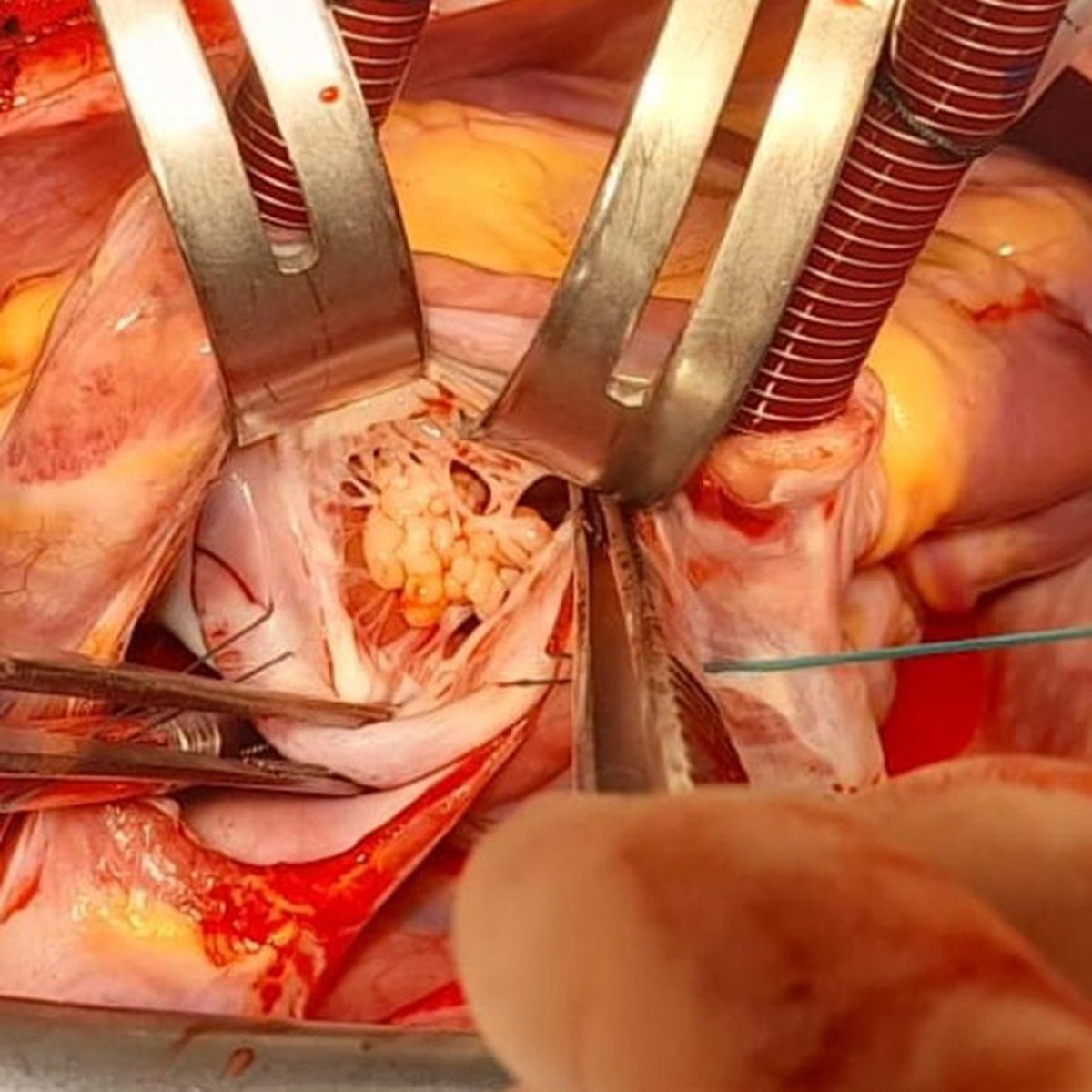
A previously fit and well 25-year-old woman with headaches ended up being diagnosed with papillary fibroelastoma (PFE). Read the case report titled Sea anemone invades the heart: Unusual lesion of the mitral valve in #JTCVS Techniques: https://t.co/gH1AObEwWT
1/ Strain Imaging in Echocardiography:
A powerful tool for detecting subtle myocardial dysfunction, far beyond LVEF.
Here’s why it’s transforming cardiology — and how you should be using it. A thread:
#CardioTwitter#Echo#FOAMed
#TechniquesThursday: Researchers found robotic myxoma resection using an ultrasonic aspirator system is simple, safe, and reliable. Read more from Chibanishi General Hospital in #JTCVS Techniques: https://t.co/hYUnJyxHR6
1/8
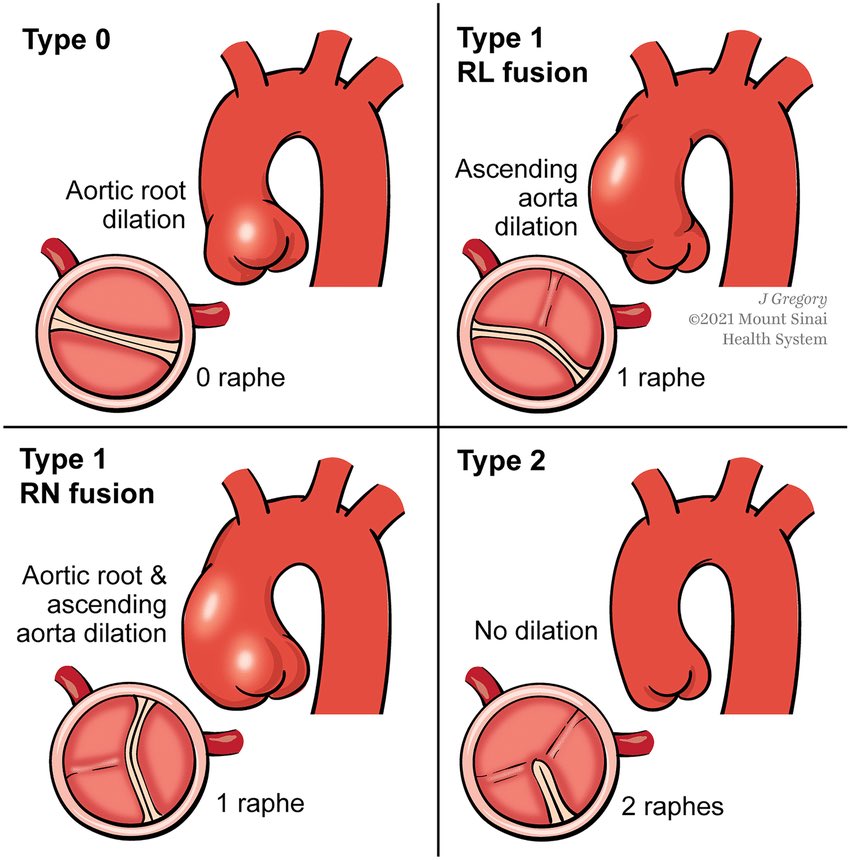
How often should patients with a bicuspid aortic valve (BAV) be monitored?
Let’s break down the latest guidelines to help prevent complications like aortic dilation, aneurysm, or dissection
#echofirst & MR
How to assess MR for proper decision making?
Follow standardized echo protocol answering the following
questions:
❓ How much
❓Structural integrity
❓Why
How much MR is there?
👉GL do recommend PISA & regurgitation volume & fraction MANY PITFALLS (N. Merke)
👉 https://t.co/L75q5vYump
👉GL asking for vena contracta
👉indirect parameter as E- wave inflow velocity > 1,2 m/s & DVI > 1,4
👉Pulmonary vein inflow reduction or flow reversal
🎯look at LV volumes as a simple byproduct of LV EF a parameter we all believe in
🎯look at forward stroke volume another parameter we do believe in
🎯never forget to do quality check by looking at RVOT SV & RVSV (in isolated MR LVOT SV = RVOT SV = RVSV)
Structural Integrity
👉LVEDS?
👉LAVI?
👉sPAP
Why?
Seen by 2D & 3D TTE first so often no need for TEE in diagnostic work up
TEE needed if TTE inconclusive or for interventional planning of therapy
SMR atrial vs ventricular
PMR
2D:
👉Look at leaflet position using Mitralvalve annulus as reference plane
🎯leaflets flat (atrial SMR)
🎯leaflets pointing towards left ventricle (ventricular SMR)
🎯leaflets pointing towards left atrium (primary MR)
Look at jet direction if eccentric or central
Eccentric jet
🎯jet direction is pointing away from prolapse
🎯jet direction is pointing towards the tethered leaflet
ventricular SMR or in case
of restricted posterior leaflet atrial SMR
Central jet
🎯jet central in atrial SMR
🎯jet central in symmetrical tethered leaflets as in DCM ventricular SMR
🎯jet central in bileaflet prolapse in primary MR
Timing of jet (use Color M Mode)
🎯holosystolic in atrial and ventricular SMR
🎯late systolic in primary MR
3D
Using 3 apical views to achieve 3 datasets from the mitral valve including the. 👉entire valve apparatus, 👉landmarks as aortic valve, the left atrial appendage and the coronary sinus furthermore 👉avoid artifacts as air
Use atrial perspective to image leaflet movement and direction
🎯primary MR shows leaflet displacement towards left atrium by using translumination facilitate by showing shadow as hint for prolapse
🎯secondary MR shows leaflet flat or from ventricular perspective pointing towards left ventricle
Leaflet position in 2D & 3D, jet direction and jet timing will help to determine the WHY
Report:
Severe primary MR due to P2 Prolapse
LV SV ml, LVOT SV ml, Reg. Vol. ml, Reg. Fraction %
PISA not possible as jet is eccentric
Vena contracta
E wave > 1,2 m/s
LV / LA dilated
LV EF & GLS
Always quality check look at RV SV & RVOT SV
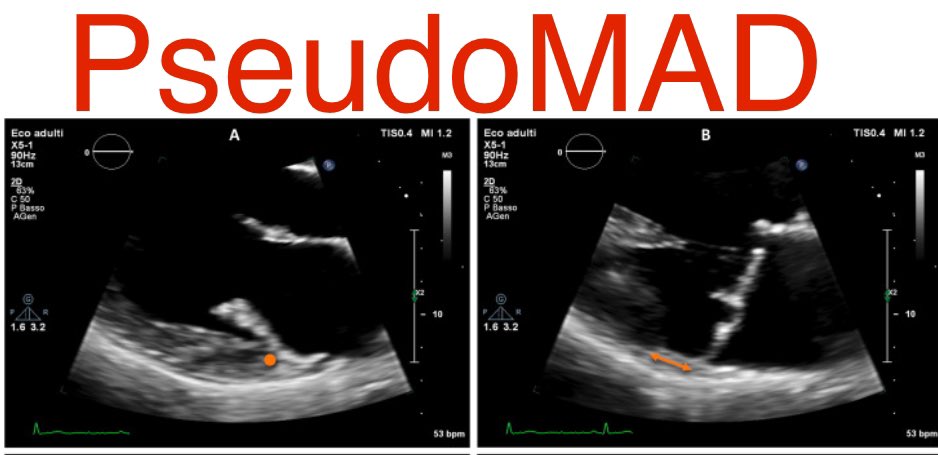
What’s in a name?
most patients with MAD actually should be called Pseudo-MAD (apparent systolic MAD) part of myxomatous degeneration assoc w curling Pickelhaube arrhythmias but not a true anatomical substrate which is seen in sys & diastole #echofirst https://t.co/cfdIr9EdNp
Bicuspid aortic valve aortopathy can progress after valve replacement! This pt is 45 years post first op and 36 years post ball-in-cage AVR (still working) now with >5cm aneurysm #LifelongCare@ClevelandClinic#AortaCenter#StarrEdwards
(1/x) A 'clot in transit' is a rare echo finding that when you see it, you might double guess yourself.
Finding a clot in transit can be a game changer for the management of pulmonary embolism 🫁🩸
A 🧵of clot in transit cases (with some important mimics)
What an amazing skill and result of apical myectomy for #apicalHCM by @HSchaffMD ! Meticulously avoiding injury to papillary muscle. Presented at our annual #EchoNY. The procedure improves LV cavity size, LV filling pressure , and clinical outcome. @MayoClinicCVS@MayoClinicCV