Ask your #renalpath question - add #askrenalpath to any tweet or quote RT. Bot created by @MedecineLibre will RT again. Moderated by @BCRenalPath & @Roboonya.
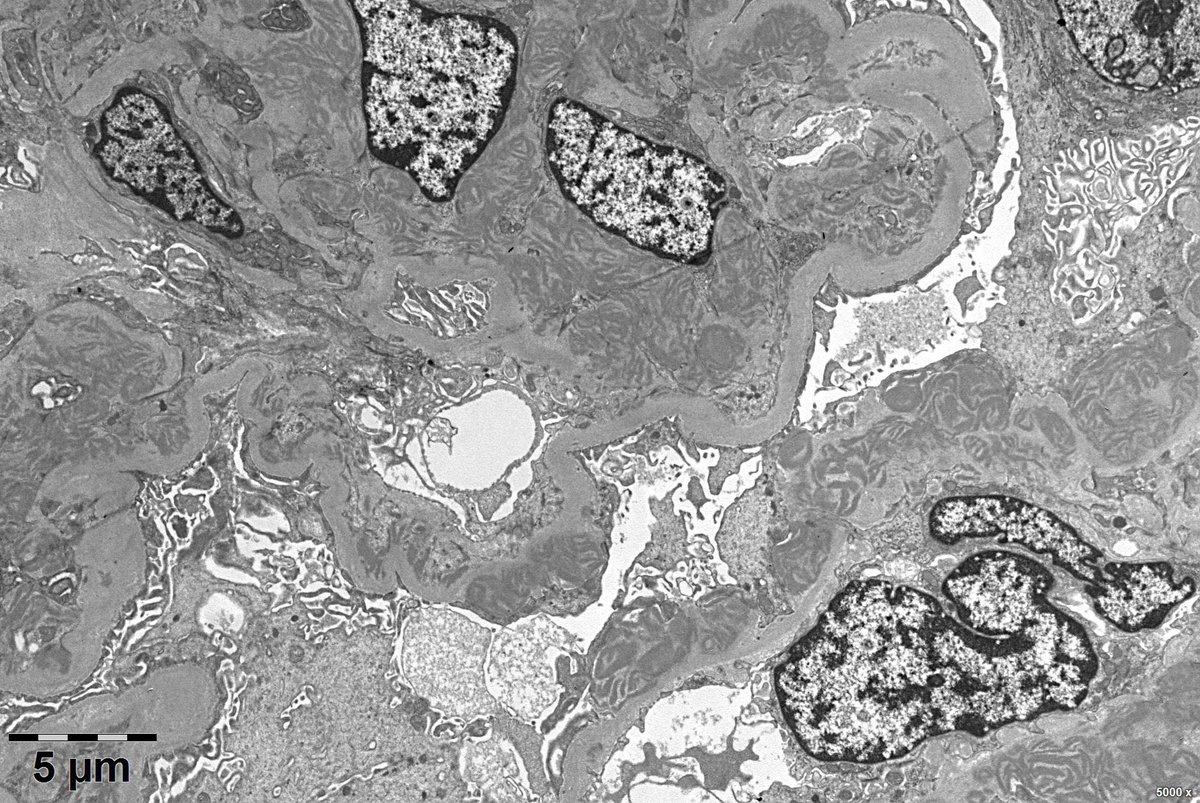
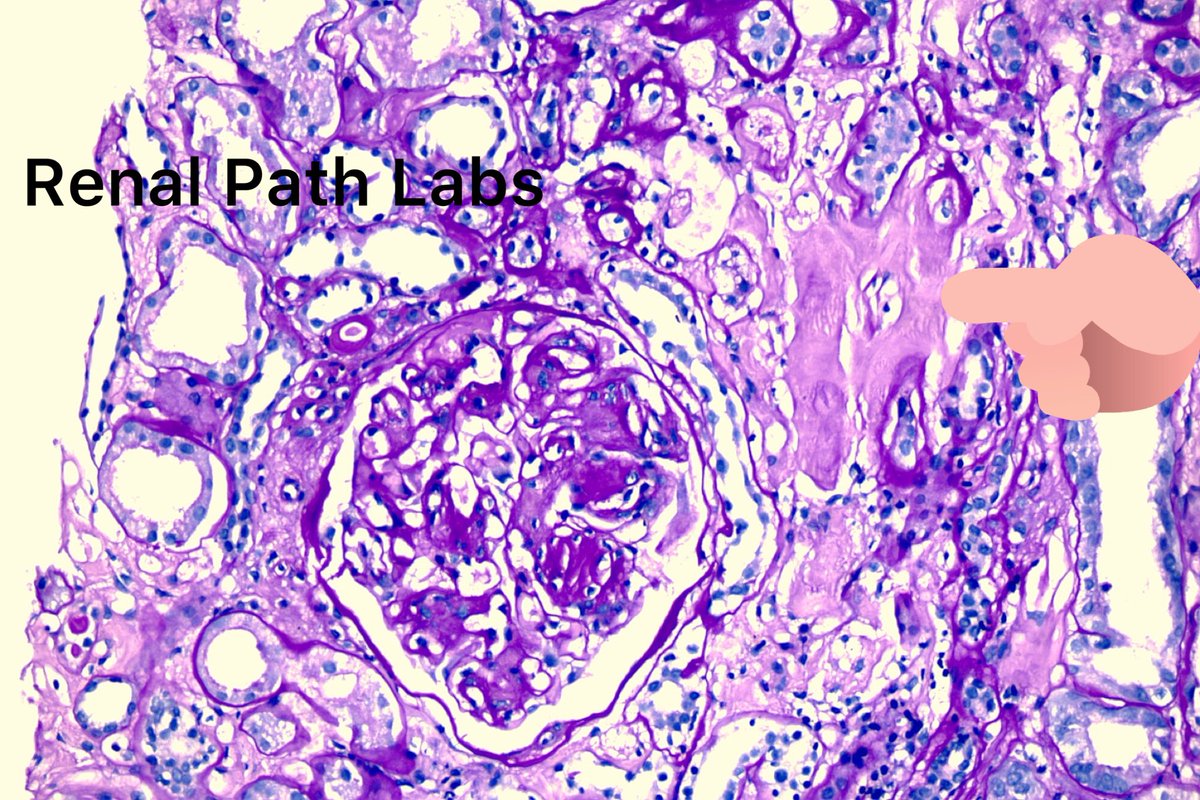
@RenalPathLabs@Ask_Renal@AskRenalPath@Renalpathsoc Case 1 granular deposits along capillary basement membrane case 2 linear deposits along basement membrane, in addition with crescents. Case 2 anti GBM disease. Case 1 MGN
@RenalPathLabs: One Ab,two patterns. Drastic difference in presentation! Thats the beauty of Science especially Renal Pathology!
Two consecutive cases we received at RPL! PathResidents, NephResidents
Shake your neurons!
@Ask_Renal@AskRenalPath@Renalpathsoc#Nephtwitter#Patht…
@askrenal: Question for #NephX#NephTwitter -
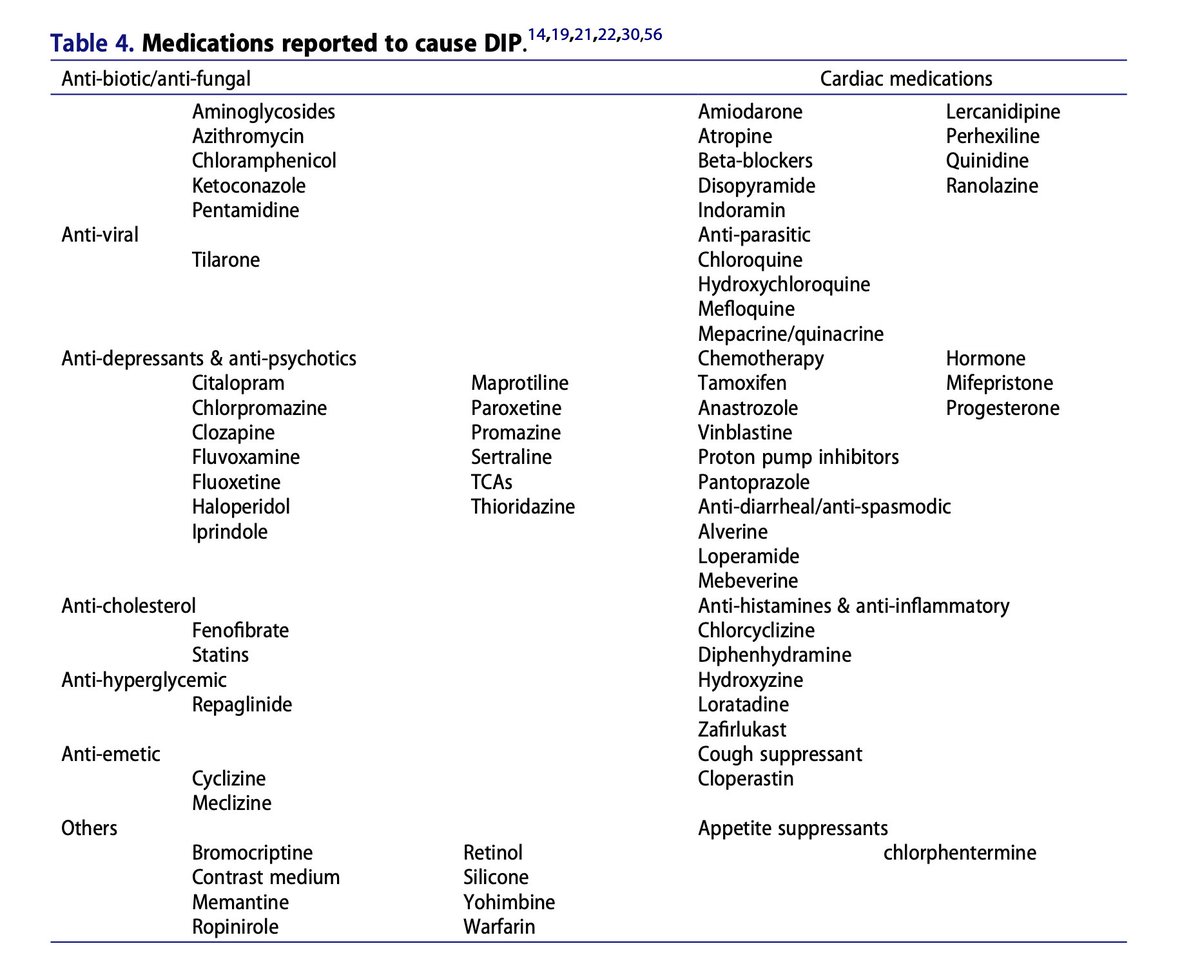
NephRodby: @askrenal@AskRenalPath Table from https://t.co/NARck4U4jb
Problem is "DIP" is NEVER defined in paper! https://t.co/vAE64szXIn https://t.co/oFo8YlHR3l
https://t.co/UbG3Q3mIZt #RenalPath
Question for #NephX#NephTwitter -
NephRodby: @askrenal@AskRenalPath Table from https://t.co/rUXRDqBAzt
Problem is "DIP" is NEVER defined in paper! https://t.co/VCuC5zBdyO https://t.co/oNTUaH3X81
@NephRodby: @askrenal@AskRenalPath Table from https://t.co/vINbpmfgtd
Problem is "DIP" is NEVER defined in paper! https://t.co/pK8qwXTecr
https://t.co/qmUWtUJk9Z #RenalPath
@askrenal: Question for #NephX#NephTwitter -
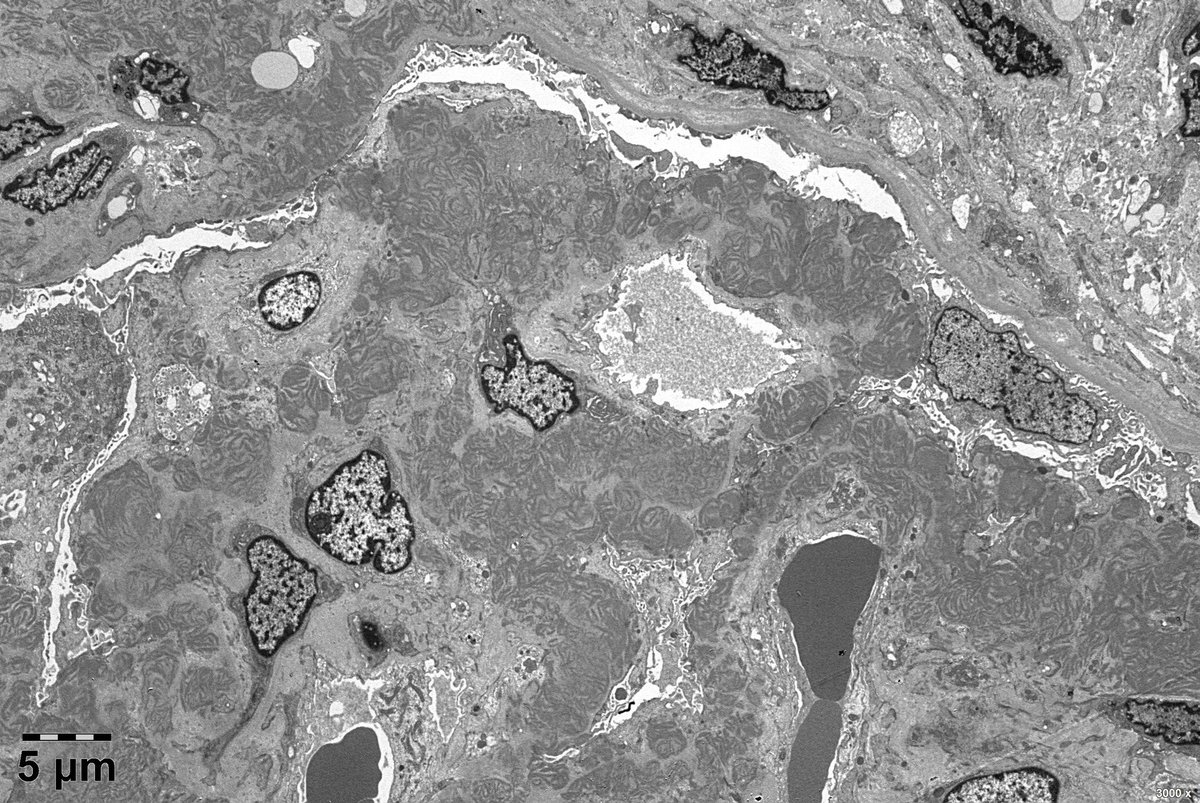
kdjhaveri: What are other causes of zebra bodies on renal bx besides chloroquine based drugs and Fabry's disease @AskRenalPath@askrenal https://t.co/S5GL8QVros
https://t.co/sLtvl5HKLp #RenalPath
Question for #NephX#NephTwitter -
kdjhaveri: What are other causes of zebra bodies on renal bx besides chloroquine based drugs and Fabry's disease @AskRenalPath@askrenal https://t.co/VlTmD1I3xF
@kdjhaveri: What are other causes of zebra bodies on renal bx besides chloroquine based drugs and Fabry's disease @AskRenalPath@askrenal
https://t.co/oXPbenUCxa #RenalPath
#askrenalpath old male, NS, SCr 1.1, normal C3 and C4, dsDNA-, ANA1:80, RF-, HCV-,splenomegaly, Pancytopenia , suspicious serum IgG-入.Numerous subendothelial, subepithelial and mesangial EDD with substructure. IF: IgG, C3, C1q, k, and 入+, few TBM and vessel wall also positive.
Renal transplant. PVN in July => IS minimization.
Currently AKI with anuria and biological TMA.
Bx: diffuse glomerular TMA, g1 ptc1 v1
Any ideas what these interstitial dots are?
Immune cells do not seem to bother about it; not the aspect of Russel bodies to me.
#askrenalpath
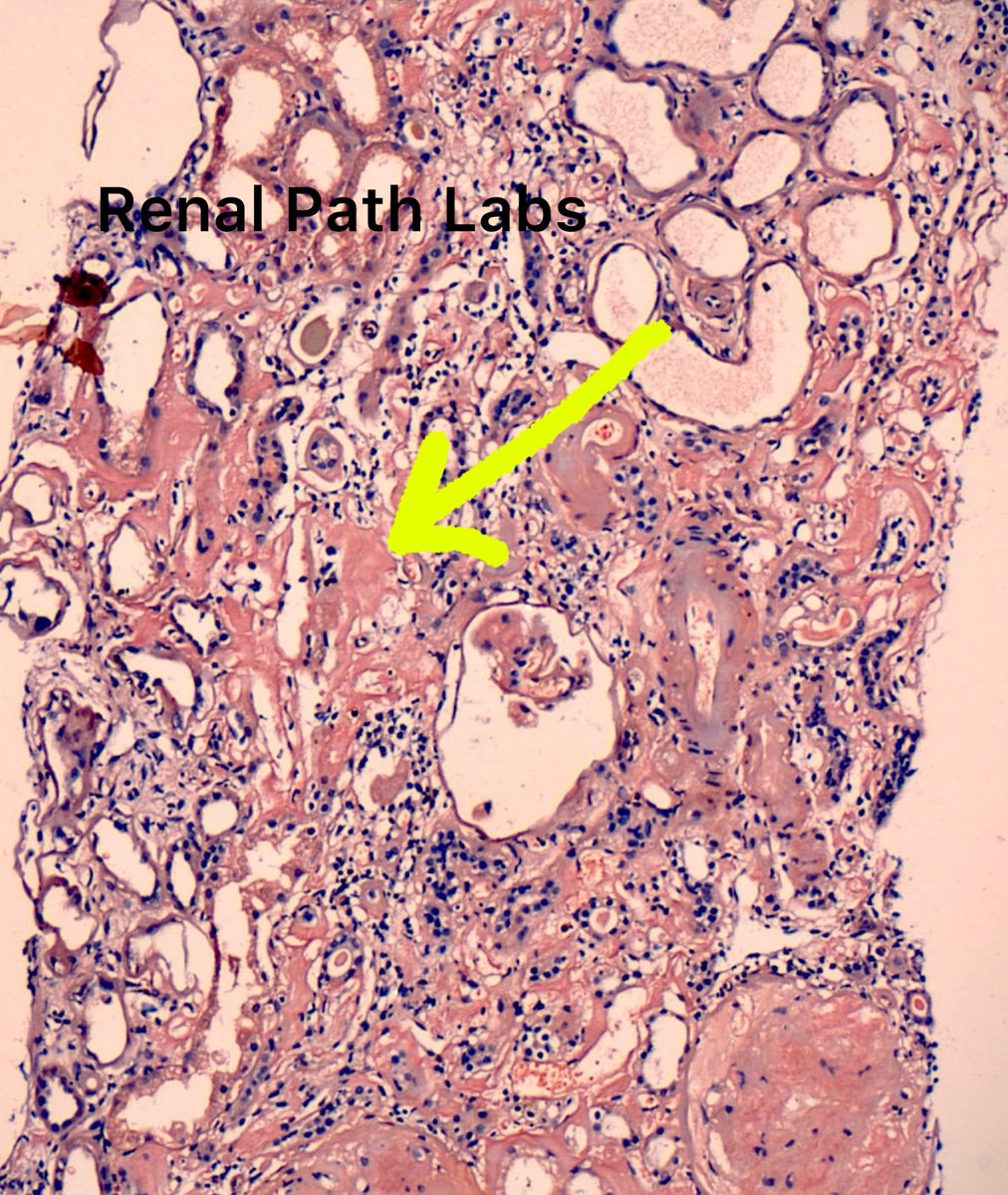
Yes,It is ALECT-2 Amyloid in kidney, coexisting with diabetes in this pt. It is rarely found in India.If interstitial amyloid is scarce, its difficult to pick.
Diabetic nodules are PAS positive,Amyloid is not.
#RenalPath#AskRenal#AskrenalPath@RenalPathLabs#NephTwitter
Subtle mesangiolysis seen with PAS
IF: 2+ granular C3 within cap loops
EM: No deposits
Favoured Dx Chronic TMA
Has anyone seen this with GVHD? #askrenalpath
If you treat type 1A rejection differently than 1B rejection, you do realize that this could be the difference of 1 lymphocyte for the tubulitis criterion, correct?
#askrenalpath