Practice changing EMERALD-3 trial: STRIDE improved PFS from 8.1 to 12.9 months in patients with HCC treated with TACE. Lenvatinib appears to add no additional benefit with added toxicity. @GABOUALFA@MSKCancerCenter@MSK_DeptOfMed
Immune-mediated AEs and OS with STRIDE and durvalumab in unresectable HCC: HIMALAYA phase III randomized clinical trial
@HEP_Journal
10.1097/HEP.0000000000001385
👉Pts who experienced imAEs with STRIDE, but not Durva had better outcome
🧐same as with Nivo/Ipi
@myESMO@ASCO@ilca@EASLnews
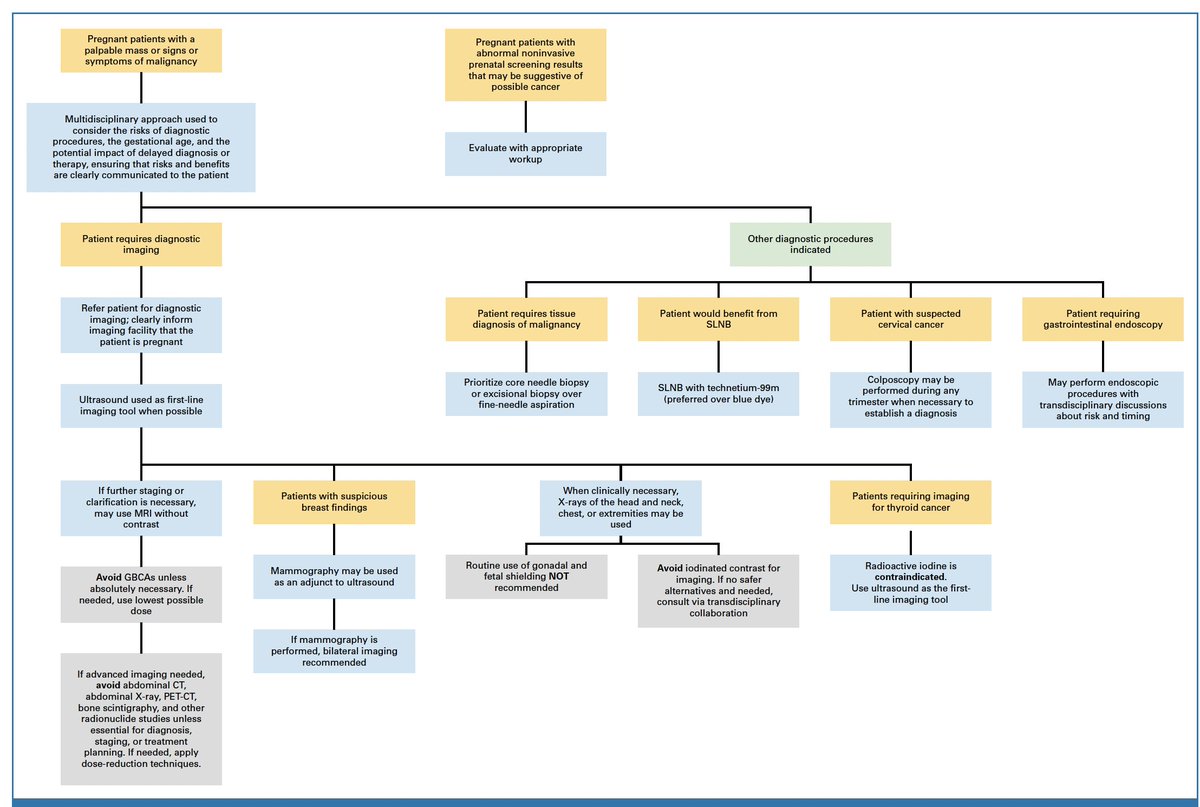
Management of Cancer During Pregnancy: ASCO Guideline
@JCO_ASCO
https://t.co/KZTF4OHCuS
👏Very useful guidance on the recommended management of cancer in pregnant patients
👉Systematic review of 450 studies
👉Many systemic therapies are contraindicated
@myESMO@ASCO
🫁 Poor PS, high PD-L1—can IO still work?
IFCT-1802 SAVIMMUNE (Ph2) evaluated 1L durvalumab in stage IV #NSCLC with ECOG PS 2–3 & PD-L1 ≥25%.
◼️ Grade ≥3 TRAEs (8 wks): 10%
◼️ ORR: 26%
◼️ 1-yr OS: 40%
◼️ PS improvement at 8 wks: 44%
Important data for a population often excluded from trials. @LungCancerRx@OncoAlert@oncodaily@JTOonline https://t.co/slBfnKXnLc
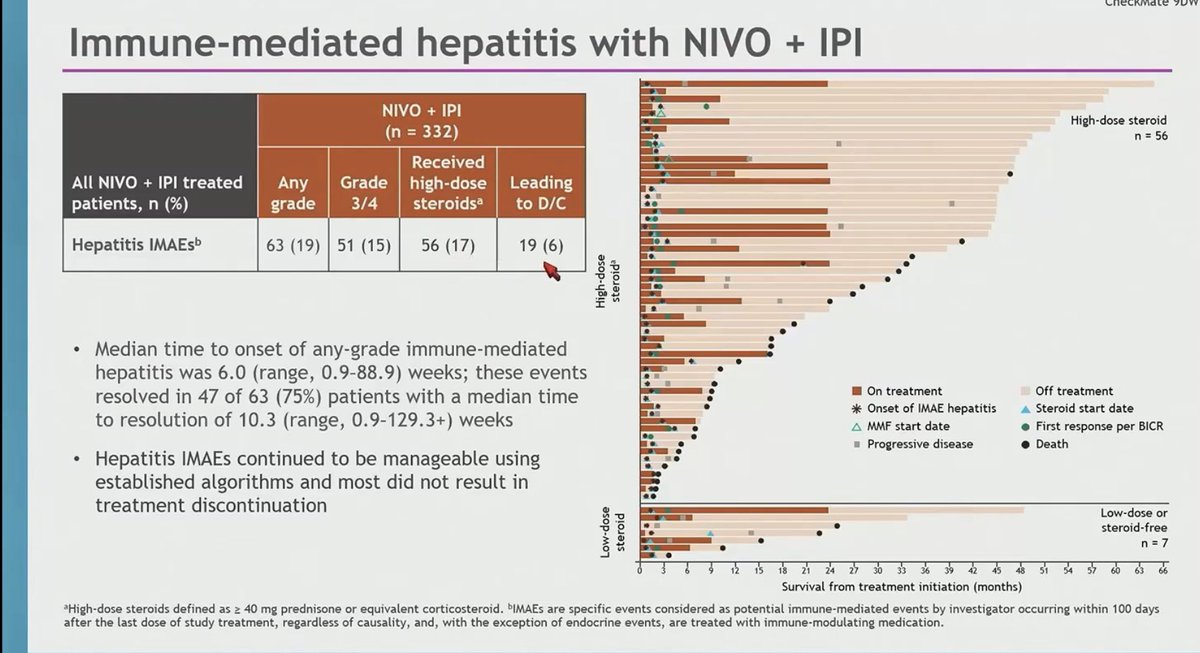
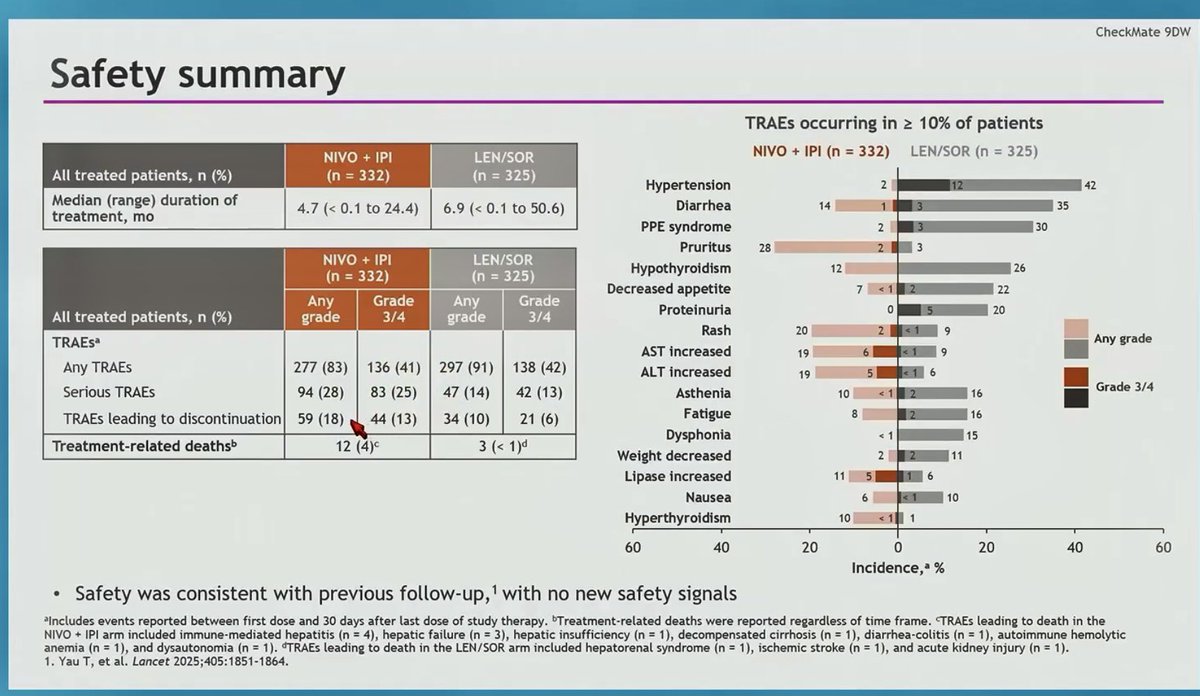
Updated CheckMate 9DW #HCC
Nivo+ipi v len/sor
➡️follow up 52mths
➡️1 in 4 pts BCLC B
➡️mOS 23.7 v 20.6mths;
➡️48mth OS rates 31 v18%
➡️G3/4 TRAEs 25 v 13%
⭐️interesting hepatitis data 19% early event ~6 weeks ‼️close monitoring
@ASCO@OncoAlert@ILCAnews
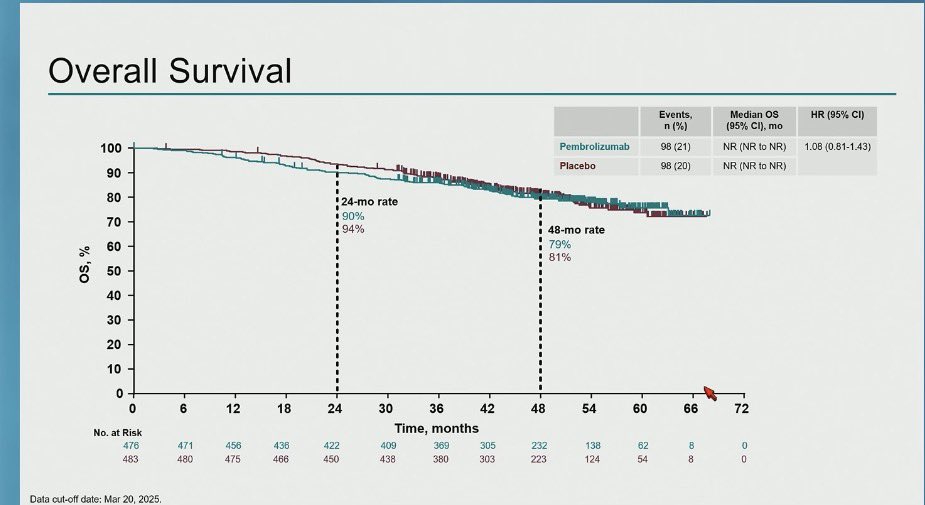
KEYNOTE-937- adj pembro v placebo #HCC
➡️ 2nd -ve trial; n=959, mFU 50.7mths
➡️ maj viral aetiology; 77% AFP<200, 83% BCLCA
➡️mRFS 46.7 v 45.5mo, mOS NR either arm
➡️≥G3 AEs 32 v 22%
higher mRFS than IMBrave050 & STORM
@ASCO@ILCAnews@EASLnews@OncoAlert#GI26
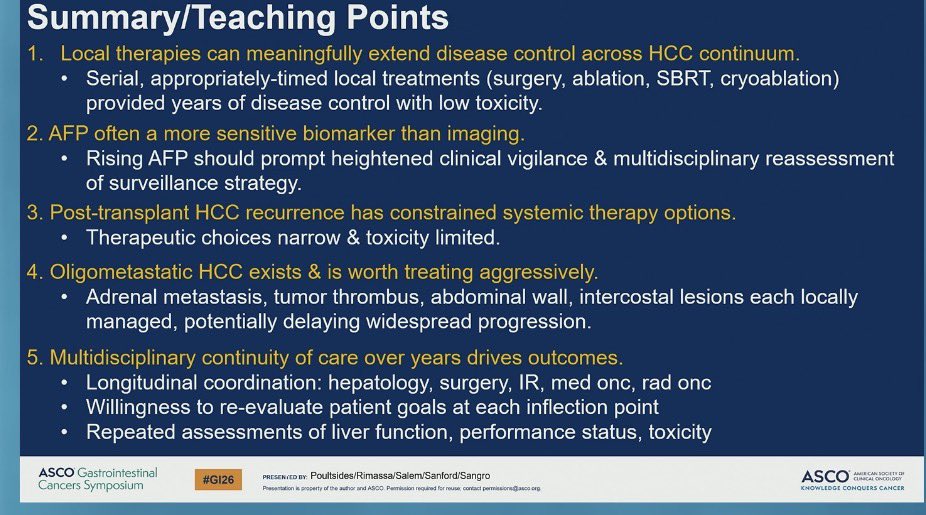
Liver Power Hour 👏 #HCC#GI26
MDT 3 cases with learning pts 👇
1. Post LT recurrence-‼️challenging Surgery/LRT where possible
2. BCLC B options- Surgery/LRT(Y90/SBRT/TACE)/systemic
3. Single lesion VP1/2 -getting to Sx Y90 v Systemic-note high risk recurrence @ASCO@OncoAlert
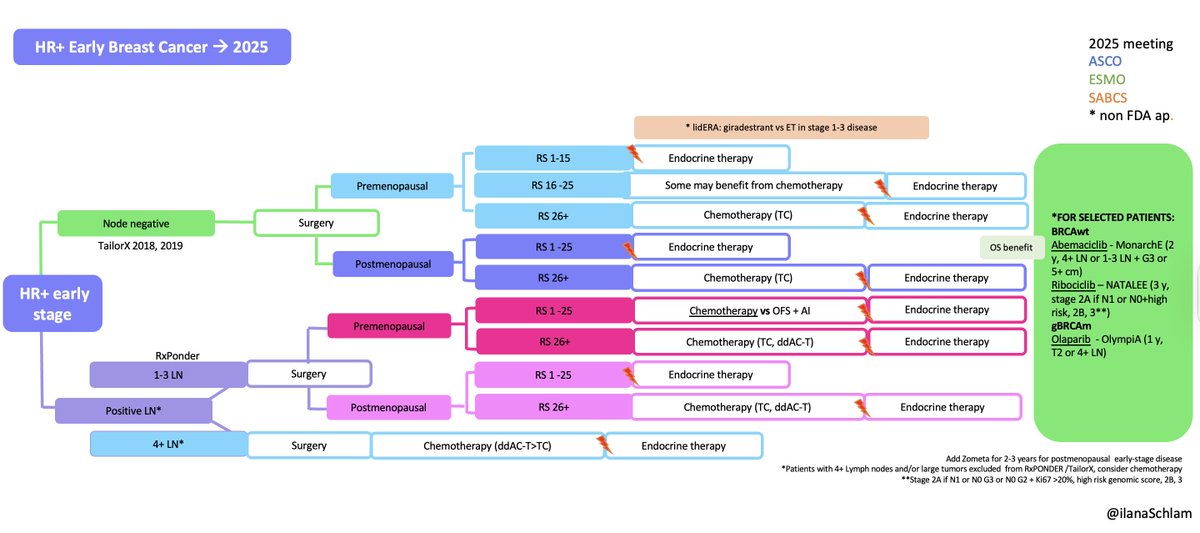
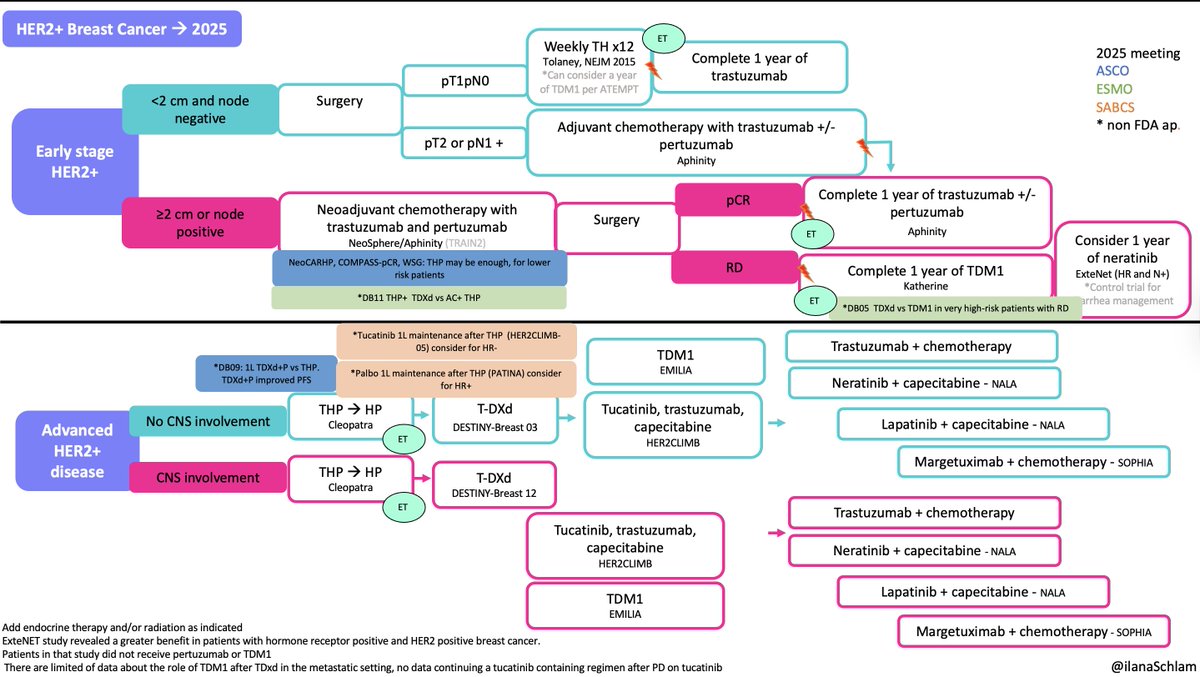
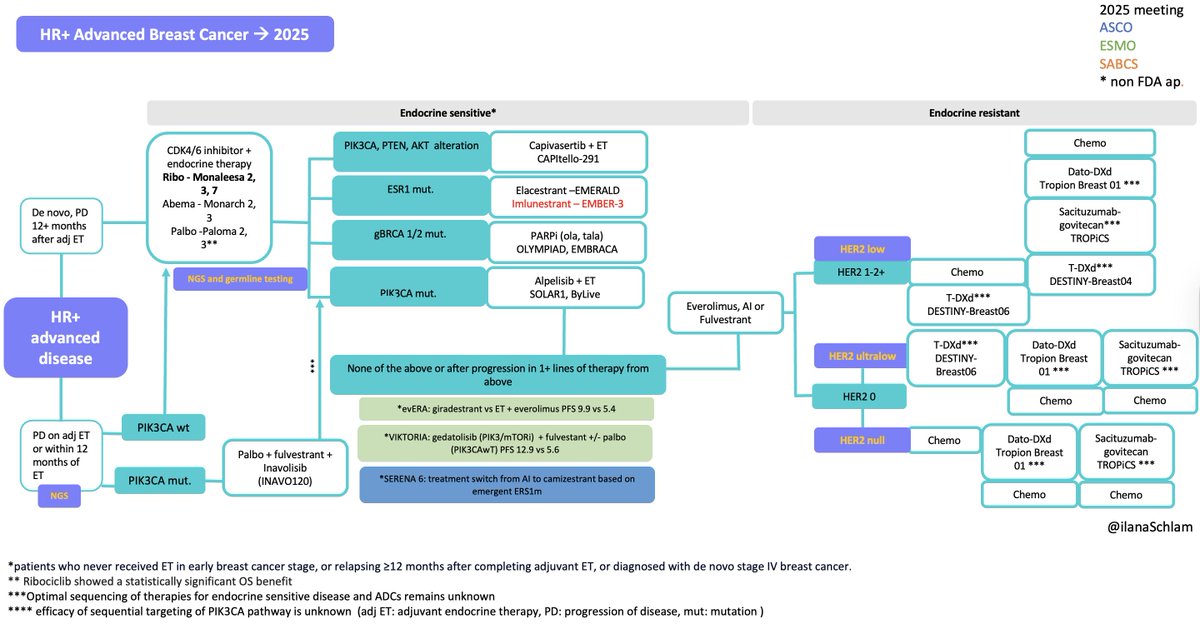
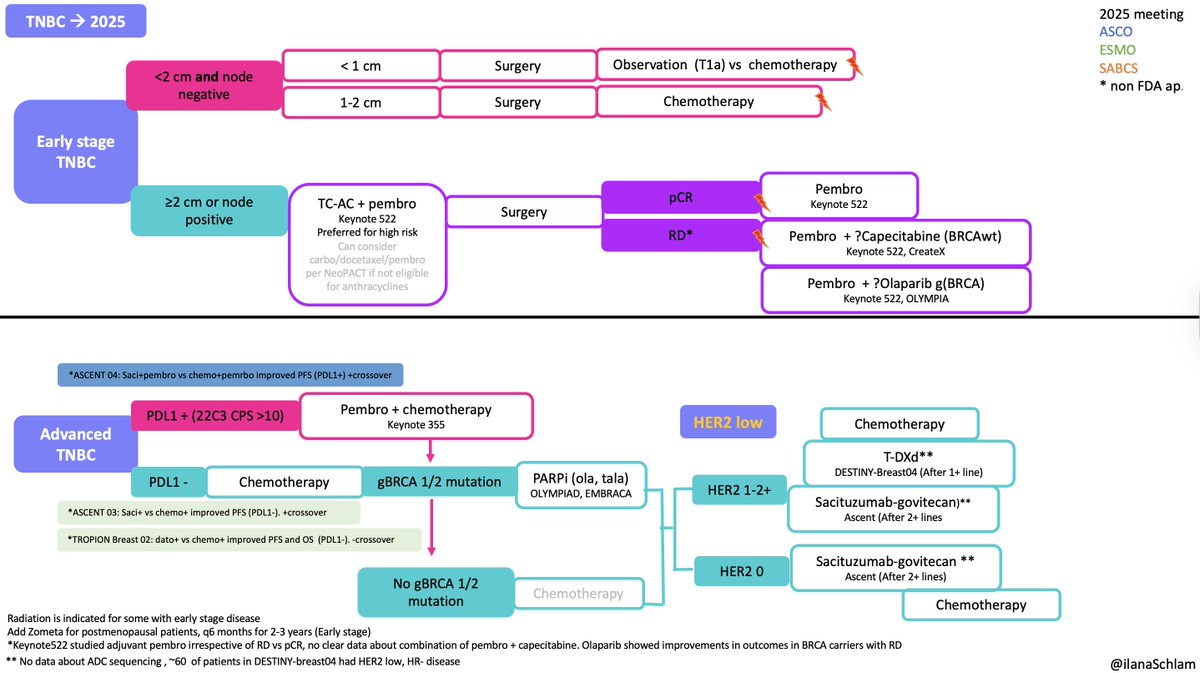
In 2025, many important and long-awaited studies were published. I included them but kept the algorithms unchanged, as there are open questions about how these data will impact practice, particularly in early and metastatic HER2+ disease and mTNBC.
@DFCI_BreastOnc#SABCS25
🚨 ONCO EMERGENCY: How to Manage EXTRAVASATION in 30 Seconds 🩺💉
Extravasation of chemotherapy = oncology emergency.
Early recognition + immediate action = tissue saved.
Here’s the crisp, protocol-ready approach 👇
1️⃣ STOP Immediately
❌ Stop infusion
❌ Do not flush
✔️ Leave cannula in situ
✔️ Aspirate as much drug as possible
✔️ Mark the area + click a photo
2️⃣ Identify the Agent
Classify the drug:
🔥 Vesicant (DNA-binding / Non-DNA)
😣 Irritant
🙂 Non-vesicant
(Anthracyclines, Vinca alkaloids, Taxanes, Platinum, Mitomycin etc.)
3️⃣ Two Key Pathways
A) “Localise & Neutralise” – DNA-Binding Vesicants
(Anthracyclines, Mitomycin, Dactinomycin)
❄️ COLD compress 20 min × 4/day × 1–2 days
💊 Antidotes:
<3 ml anthracycline → Topical DMSO
3 ml anthracycline → Dexrazoxane (Savene) within 6 hrs
Mitomycin → DMSO
B) “Disperse & Dilute” – Non-DNA Binding Vesicants
(Vinca alkaloids, Taxanes, Trabectedin)
🔥 WARM compress 20 min × 4/day × 1–2 days
💉 Hyaluronidase 150–1500 IU SC around site (5 injections)
4️⃣ Elevate, Analgesia, Plastics Referral
✋ Elevate limb
💊 Analgesics if required
🏥 Early plastics/flush-out team for large-volume or CVAD extravasa
tion
5️⃣ Follow-Up
Mandatory review within 1 week
Patient counselling: monitor for redness, blistering, worsening pain
Document EVERYTHING (site, size, drug, photo, interventions)
💡 TAKE-HOME
Extravasation is rare but high-stakes.
Most injuries are preventable with:
Good venous access
Trained staff
Fast action
Correct antidote pathway
Oncology teams save tissue before they save time. ⏱️🩺
🔖 Save this. Share with your residents and healthcare staff.
#OncoTwitter #MedTwitter #ChemoSafety #Nursing #Oncology @myESMO@OncoAlert@ESMO_Open@asco