Associate Professor of Surgery, family man, house church, HIPEC research, Peritoneal Surface Oncology Research, Proteomics in postoperative complications
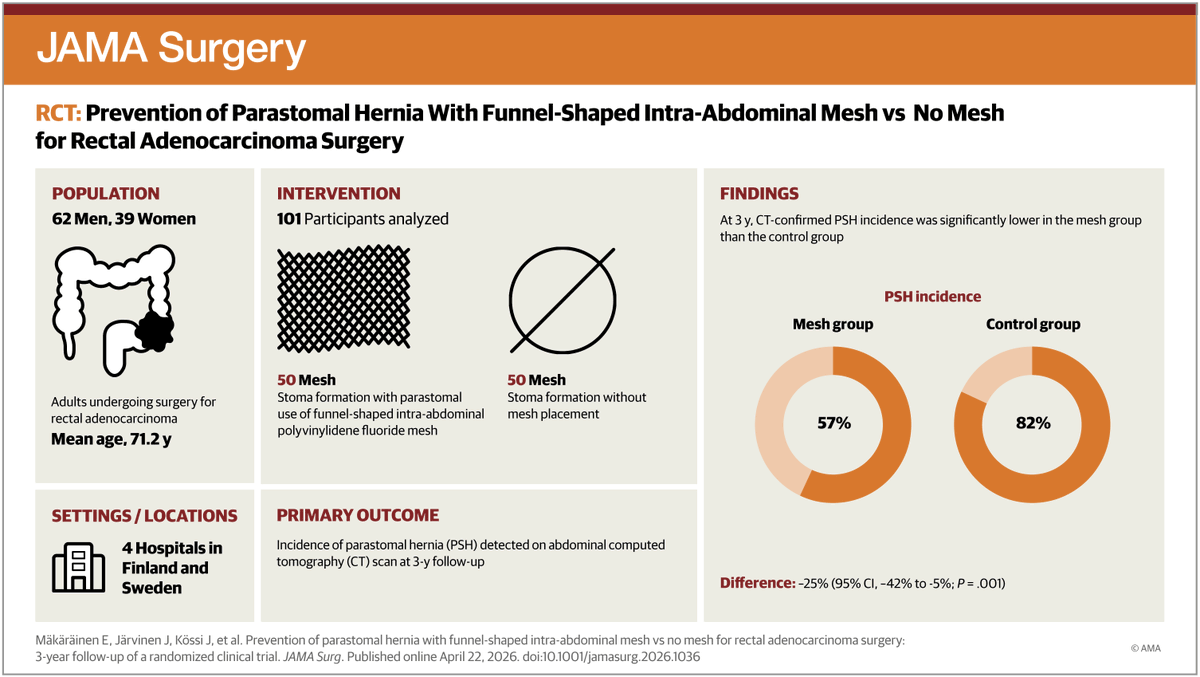
In patients undergoing permanent colostomy for #RectalCancer, use of a funnel-shaped intra-abdominal mesh reduced parastomal hernia incidence and size at 3 years without increased complications compared with no mesh. https://t.co/RQkiWexN0a
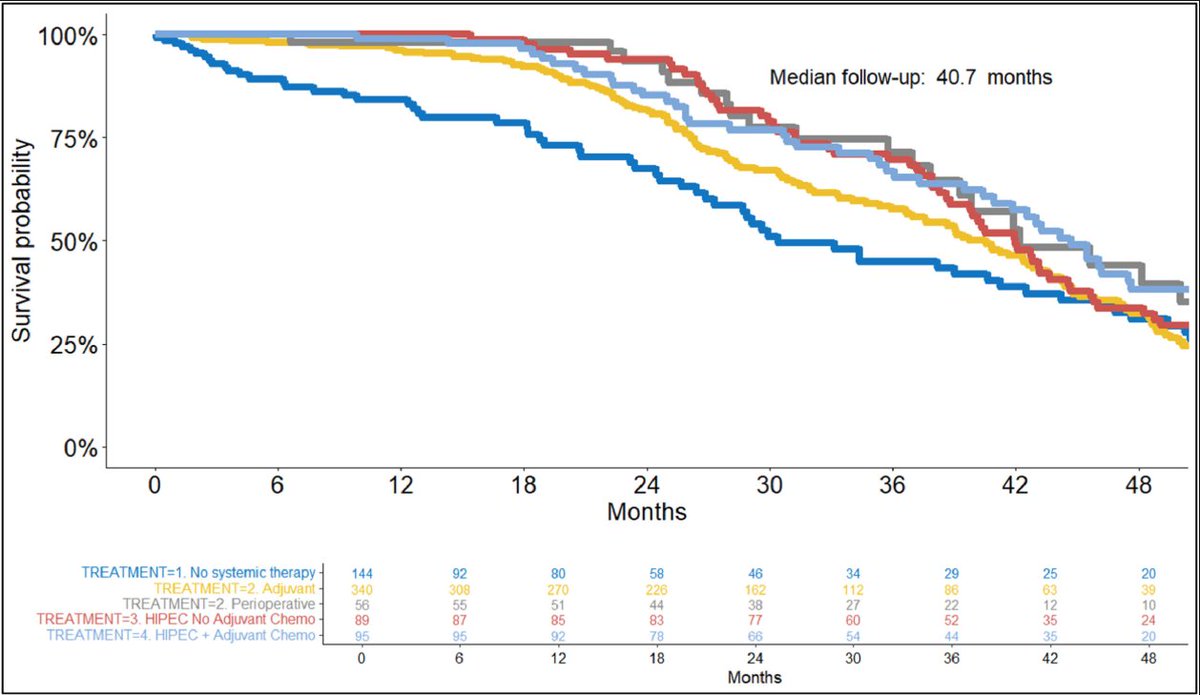
Efficacy and safety of intraoperative hyperthermic intraperitoneal chemotherapy for locally advanced colorectal cancer (HIPECT4): final analysis of randomized clinical trial @aecirujanos@PSOGI_EC@indepso@GrupoTTD@ISSPP1 https://t.co/3BLppbgBbz
Slightly disheartening! More studies need to look att biological mechanisms of tissue healing. Perhaps more relevant prehab interventions can be found… microbiome interventions seem to show some promise.
Effects of Multimodal Prehabilitation on High-impact Surgery Outcomes: a prospective stepped-wedge, hospital-wide implementation study
➡️ https://t.co/LzLXfdfpiD
In this hospital-wide stepped implementation study, multimodal prehabilitation showed partial adherence and did not reduce postoperative Clavien–Dindo grade ≥2 complications or length of hospital stay in a heterogeneous surgical population
Although no statistically significant effects were observed, the confidence intervals included potentially clinically meaningful differences, meaning a relevant effect cannot be excluded
Exploratory analyses suggested a trend towards fewer complications in patients undergoing gastrointestinal oncological surgery, supporting further evaluation of targeted prehabilitation in high-risk populations
Work by Luuk D Drager, MD , Femke Atsma, PhD , Dieuwke Strijker, PhD , Linda A G van Heusden-Scholtalbers, MSc , Monique J M D van Asseldonk, MSc , Jonas Rosenstok, MA , Joost P H Seeger, PhD , Sjors Verlaan, PhD , Laurien M Buffart, PhD , Prof Cornelis J H M van Laarhoven, PhD , Baukje van den Heuvel, PhD on behalf of , the F4S PREHAB Collaborative Group
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @RCPSGTrainees @aecirujanos@SEIQuirurgica@iss_sic #MedicalTechniques @BJSAcademy@young_bjs@BJSOpen@evanscolorectal@robhinchliffe1@bplwijn@MalinASund@nfmkok@TejedorPat@paulo_sutt@PVaughanShaw@JJEarnshaw@juliomayol@ksoreide #some4hpb #some4tpl @DPCG_official@pancreatitis_nl@PancreasClub #PancreasClub2023 #PancreaticCancer #Pancreatitis #HCC @PanCAN #PanCANawareness @EurPancClub@P_C_E_@dice_europe #PancreaticCancer #cholangiocarcinoma #colorectalsurgery #StepUp4CRC @FightCRC@ACPGBI #ERAS @dice_europe #Crohn #proctology @Dukes_Club@ACPGBI_EduTrain@AECP_FAECP@PelvExGroup@escp_tweets@YouESCP #TeachMeColoproctology
#Some4COLoprocto #some4UGI #uppergi #esophagealcancer #gastriccancer #reflux @ISDE_net@Augishealth@roux_group@T4UGIS@SARONG_Trial@YoungIFSO #bariatricsurgery
@simonds_m@ouroborossun@BarbaraOneillAU You have the added bonus of all circulating cells disappearing as the body takes care of them. Without the primary tumor, no new cells will be released. But with the primary tumor left in the body, new cells will release into bloodstream continually until massive metastases.
@simonds_m@ouroborossun@BarbaraOneillAU You can measure circulating tumor cells very early already in stage I disease (they haven’t gained the ability to metastasize yet). Is it possible this goes up slightly during surgery. Sure. But not removing the tumor garantees it will increase and lead to metastasis as it grows.
If you look at all open close cases from different studies, the median survival is basically always under 12 months. Patients with extensive peritoneal disease do not survive long on systemic chemo. It seems that the overall survival is increased by about 1 year. Should we do it?
Are we aborting CRS attempts in too many patients in fear of a CC-1 cytoreduction? It may be costing our patients survival time.
The clinical benefit of a near complete cytoreduction in patients with... https://t.co/8K0DVWLKq4
⭐️Just published - The role of systemic chemotherapy to CRS/HIPEC in patients with appendiceal cancers
⛔️ No role for systemic chemo
❓Where does chemo fit❓
@jpshen_md#GI26 Abst#840 also shows no benefit of AC in early stage dz
https://t.co/zO19wWn6E5
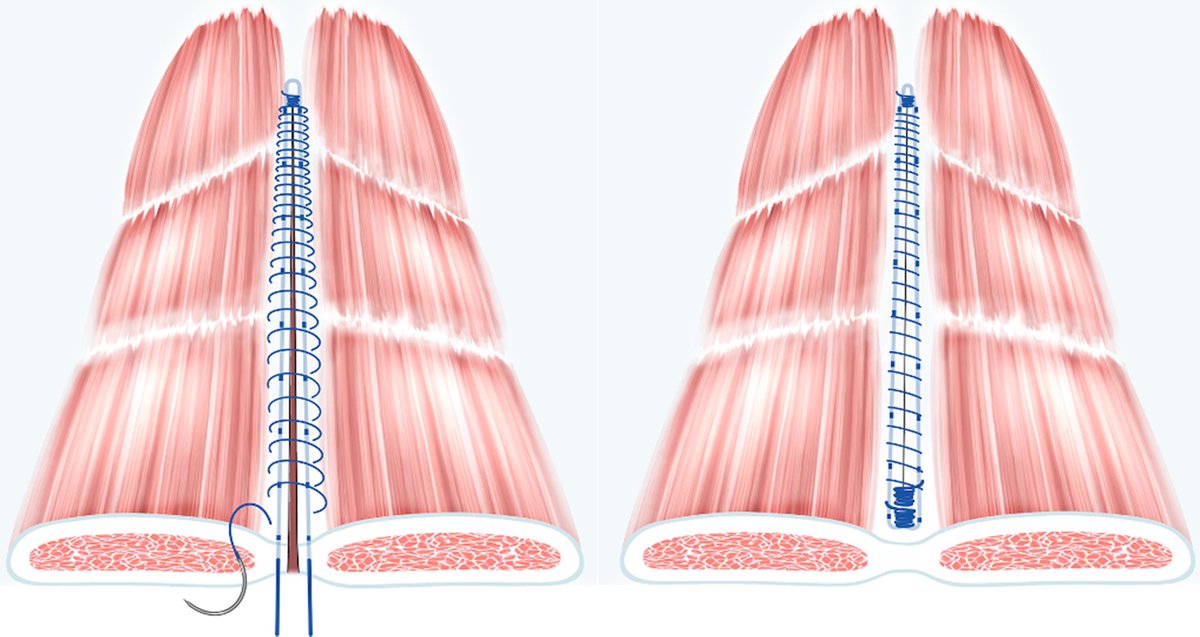
Reinforced tension-line suture after laparotomy: long-term results of Rein4CeTo1 randomized clinical trial
➡️https://t.co/AqYmnd5yex
The aim of this randomized clinical trial was to investigate whether a reinforced tension-line (RTL) suture reduces 3-year computed tomography-detected incisional hernia incidence. The RTL technique significantly reduced the incidence of incisional hernia compared with the standard facial closure technique in patients undergoing open colorectal cancer surgery. The incisional hernia incidence was 6 of 43 (14%) in the RTL and 21 of 58 (36%) in the standard facial closure group.
👏👏👏Charlotta L Wenzelberg , Peder Rogmark , Olle Ekberg , Ulf Petersson , Carl-Fredrik Rönnow
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @BJSAcademy@BJSurgery@eurohernias #hernia #hernia @herniaistanbul@BritishHernia@HerniaIndia@awrsurgeons
Is it sexy? No.
Is it incredibly important for how we treat patients? Absolutely 🧠🧬
For over 20 years, 6 months of oxaliplatin plus a fluoropyrimidine has been the default for stage III colon cancer, and often high-risk stage II and rectal cancer. The cost has always been cumulative neuropathy that can follow patients for life ⚡️🖐️
The SCOT trial, the largest study in the IDEA collaboration, gives us long-term clarity with nearly 6,100 patients and more than 6 years of follow-up:
📊 5-yr DFS identical with 3 vs 6 months: 72.9% vs 72.9%
📈 5-yr OS identical: 82.4% vs 82.4%
✅ Noninferiority for OS formally met for 3 months
Where this really matters clinically:
🟢 CAPOX clearly supports 3 months
🟢 Low-risk stage III shows no OS penalty
🟡 Even high-risk disease sees only tiny absolute OS differences
⚠️ Meanwhile, neuropathy nearly doubles when oxaliplatin is extended to 6 months. Many patients pay a lifelong price for minimal benefit.
SCOT also uniquely included rectal cancer patients treated with upfront surgery, and here too, 3 months held up. This fits perfectly with modern TNT strategies 🧩
Takeaway:
This isn’t flashy, but it’s foundational. For most patients with localized colon or rectal cancer, 3 months of adjuvant CAPOX is enough. Six months should be the exception, not the rule, and always a shared decision 🤝
Sometimes the most important advance is knowing when to stop.
@OncoAlert@TheGutOncLab
#GI26
https://t.co/geX09H4ltq
@ConsorciCSI Intravenous lidocaine infusion compared to thoracic epidural analgesia in cytoreductive surgery with or without heated intraperitoneal chemotherapy. A retrospective case-cohort study https://t.co/heuiHaXhPz
New article from the Uppsala HIPEC center looking at the use of preoperative chemotherapy in colorectal peritoneal disease. Could FOLFIRI + bev be the optimal choice for preop chemotherapy in colorectal peritoneal disease?
https://t.co/3KCGmqIeYj
Anastomosis versus rectal stump procedure in cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for colorectal and appendiceal peritoneal metastases: A comparative study - Ghanipour - 2025 - Colorectal Disease - Wiley Online Library https://t.co/3DUHGqBPJB
⚖️ TNT in Rectal Cancer: Promise or Premature?
💊 Total Neoadjuvant Therapy (TNT) has been hyped for LARC, but does it really beat standard chemoradiation (CRT)?
👥 4 Key RCTs:
•RAPIDO → ↓ distant mets, �� no OS gain
•PRODIGE-23 → ↑ DFS, small OS edge (but early curve drop & underpowered)
•POLISH II → initial OS benefit → vanished at 8 yrs
•STELLAR → ↑ 3-yr OS (86.5% vs 75.1%), but short f/u
📊 pCR rates: higher with TNT (22.5% vs 13.3%) but confounded by shorter CRT–surgery interval.
🚨 Takeaway: TNT = modest ↓ distant mets, unclear OS benefit, more toxicity. CRT remains standard until better biomarkers guide who truly benefits.
📖Ubink et al. JCO Oncol Pract. 2025.
DOI: https://t.co/OQSE3RPRPj
#OncoTwitter #ColorectalCancer #RadiationOncology #Oncology
@OncoAlert @esmo_open @myESMO @ASCO @JCOOPjournal