@Satyayadav__ This effectively closes #CPX-351 role in children with #AML with #AAML1831 also showing futility in interim analysis. interesting the experiment arm in that trial also had a trend towards lower EFS.
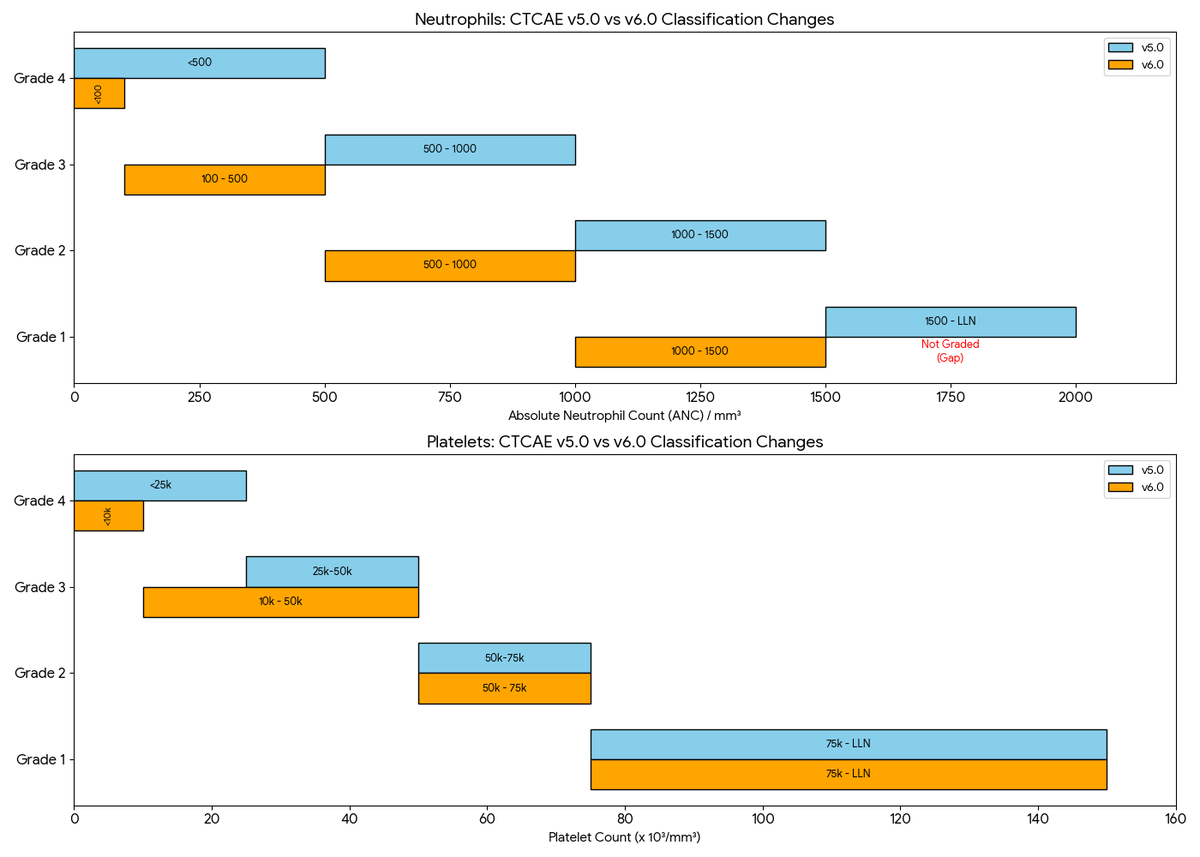
💣 Important Shift in Cytopenia Grading: CTCAE v6.0 Update
If you are a PI running #Hematology or #Oncology trials, note these key changes in the new CTCAE v6.0 vs v5.0:
📉 General Trend: "Downgrading" of severity. Many counts that were previously Grade 3/4 are now lower grades.
🧪 Neutrophils:
Grade 1 Gone: ANC 1000–1500 is now Grade 1 (was G2). The old Grade 1 (1500–LLN) is no longer graded.
Stricter G4: threshold drops from <500 to <100/mm³.
🩸 Platelets (Thrombocytopenia):
Wider G3: Now covers 10k–50k (previously 25k–50k).
Stricter G4: threshold drops from <25k to <10k/mm³.
v6.0 also adds "transfusion indicated" to Grade 3 and "urgent intervention indicated" to Grade 4 criteria.
Overall, IMO these new thresholds align better with clinical practice.
#ClinicalTrials #MedEd #OncTwitter #DrugSafety
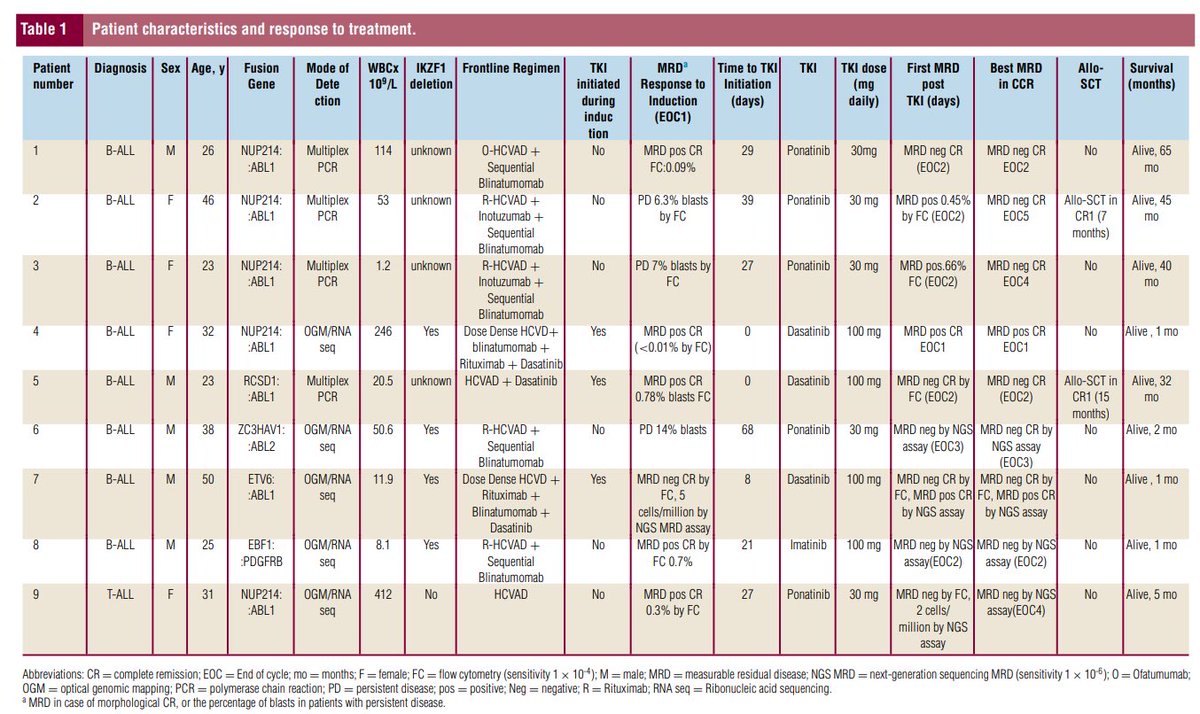
👉Delighted to share case series of pts with ABL class fusion ALL who received TKI with frontline Rx for ALL.Notably all 9 patients remain in CR1.
👉 Highlights need for early identification of kinase sensitive fusion and initiation of TKI @BraishJulie@MDAndersonNews
Link👇
Bone Marrow Transplantation for Sickle Cell Disease:
A Study of Parents' Decisions: New England Journal of Medicine: Vol 325, No 19
1991 NEJM study found that 54% of parents of kids with sickle cell disease were willing to accept a 15% mortality risk from bone marrow transplant to achieve a cure.
@Satyayadav__
#SickleCell #BMT
https://t.co/uskCsxHOcj
29% higher risk of B-cell #Acuteleukemia before 5 years of age in a child(mainly boys 41% higher risk) born through PLANNED C-SECTION!—A Swedish population‐based study. #VaginalDelivery not only prevents Allergies, Asthma or Diabetes but also #Leukemia! https://t.co/N20EsMP031
🧬✨ ATRA Goes Beyond APL! 🔬💊
All-trans retinoic acid (ATRA), the vitamin A derivative that cured APL by reactivating differentiation in leukemic blasts, is now stepping into non-APL AML 🧠🔥
🧱 In a new twist, ATRA doesn’t target blasts directly—but instead acts on the bone marrow niche! Specifically:
➡️ Targets osteoblasts with activated β-catenin
➡️ Induces proteasomal degradation of β-catenin (GSK3-independent) 🚫🧬
➡️ Suppresses JAG1-Notch1 signaling that fuels AML 🚷📉
🧪 In mouse models & primary AML samples, this niche-targeting effect showed promise—especially in ~40% of AMLs with active β-catenin in osteoblasts.
👨⚕️ Clinical highlight: An AML patient resistant to azacitidine + venetoclax achieved CR after ATRA was added. 💥
🔍 Ongoing trials (Germany 🇩🇪 & China 🇨🇳) are evaluating ATRA + HMA ± venetoclax in front-line AML.
💡Takeaway: ATRA may be repurposed as a non-cytotoxic, niche-targeting agent in AML, reviving the relevance of retinoids in modern oncology. Solid tumors like pancreatic cancer may be next! 🍊🧪🧱
https://t.co/LFT6tjTyVA
@TalhaBadarMD@NitinJainMD@Daver_Leukemia@DrHKantarjian@doctorpemm@jayastuMD @GCC_Cortes @bose_prithviraj@RaajitRampal@Alkalidr@PratzKW@davidsteensma@Dr_AmerZeidan@drsangeetmd@lane_andy@CarrawayHetty@nihardesai89@akhilrk1989@mithunap11@chepsyphilip@pb10_bmt@vishvdeepkhush@udaypkulkarni@DrArunCMC@Fadihaddad_MD@AuclairDan
At many large institutions, it’s now common for nurses to have the authority to question, and sometimes override, physician decisions.
This isn’t inherently a bad thing. Patient safety should always come first, and questioning orders when there's a genuine concern should be encouraged.
But balance matters. A flight attendant doesn’t knock on the cockpit door every 10 minutes to make sure the pilot really wants to follow that flight path. Trust and role clarity are essential to any high-functioning team.
What’s more troubling is the asymmetry of authority. Nurses are empowered to second-guess physicians, but they’re restricted from exercising basic clinical judgment. They can challenge a medication decision, but can’t give Tylenol at midnight without a physician logging into the EMR. They can raise concerns about a diet, but can’t update a diet order themselves.
They’re trusted to question, but not to act.
Meanwhile, physicians bear all the liability, all the documentation burden, and all the bureaucratic clicks, yet their authority is increasingly undermined.
Responsibility without authority is a recipe for burnout. And ultimately, for worse care.
Intrathecal MTX Prophylaxis 💉🧠 in DLBCL: No Impact on Parenchymal CNS Relapse
•Key Point: Most CNS relapses in DLBCL are parenchymal, not leptomeningeal
•Implication: IT chemotherapy alone (e.g., MTX) doesn’t prevent CNS relapse
•Multiple trials confirm:
•RICOVER-60: 6.9% vs 4.1% (no benefit with rituximab)
•Tai et al: 18% CNS relapse despite IT
•Schmitz et al: No CNS benefit
•GOYA / UK NCRI / NCCN datasets: consistent lack of efficacy in CNS relapse prevention
•Why?
•IT chemo distributes in CSF → targets leptomeninges
•Parenchymal CNS involvement needs systemic high-dose MTX or CNS-penetrant agents
•Takeaway:
•Do not rely solely on IT MTX for CNS prophylaxis in high-risk DLBCL
•Consider HD-MTX or systemic CNS-directed therapy in select high-risk patients 🧠🔥
#DLBCL #CNSRelapse #Hematology #Oncology #ASH2024 #CNSProphylaxis #HighRiskDLBCL