🔥 More is not always the best
REDUCE trial demonstrated that every 12 weeks denosumab is not inferior to standard every 4 weeks
✅ Non inferior efficacy
✅ Improved safety profile
✅ Reduce cost
I love this type of trials!
Congratulations to all investigators
#ASCO2026 - Advanced Gastric cancer
Abstract 4007 - Adding oral EP4 antagonist ONO-4578 to chemo + IO in Stage IV gastric cancer.
- Median PFS was significantly longer with ONO-4578 vs placebo
9.0 vs 6.9 months; HR 0.67; 90% CI 0.48–0.92; P=0.040.
- Median OS favored ONO-4578 (not reached vs 12.7 months; HR 0.60; 95% CI 0.37–0.96).
- ORR was higher in the ONO-4578 group (62.0% vs 48.7%). Serious TEAEs occurred in 53.7% vs 42.7%.
IMPORTANT: Results were better for PD-L1 positive tumors.
This Phase II RCT shows that adding the EP4 antagonist ONO-4578 to standard nivo + chemo improves PFS and trends toward OS benefit in 1L HER2-negative gastric/GEJ cancer.
Although OS data are immature and this is a Phase II trial, this is a first demonstration that PGE2-EP4 pathway inhibition can enhance immunotherapy efficacy in this setting - warranting Phase III confirmation.
#GIonc #StomachCancer
@MoffittNews
EMERALD-1, EMERALD-3, CARES-005, LEAP-012, (and maybe Imbrave 050, although for post-resection or ablation; and EMERALD-Y90 for post-Y90) all test a similar idea: will adjuvant systemic therapy improve outcomes after local regional therapy? PFS benefits are seen across all studies (except 050). But OS are all immature. Are we just giving systemic therapy earlier for these patients who would eventually have more advanced disease? Without final OS, post-TACE systemic therapy is probably not given universally as of today. Hopefully we will have the data soon.
But for some high risk patients, there might be benefits. We need to investigate who in the control arm “have no chance” to receive systemic therapy upon progression. Those are the patients we want to consider treating earlier.
And the debates continue…
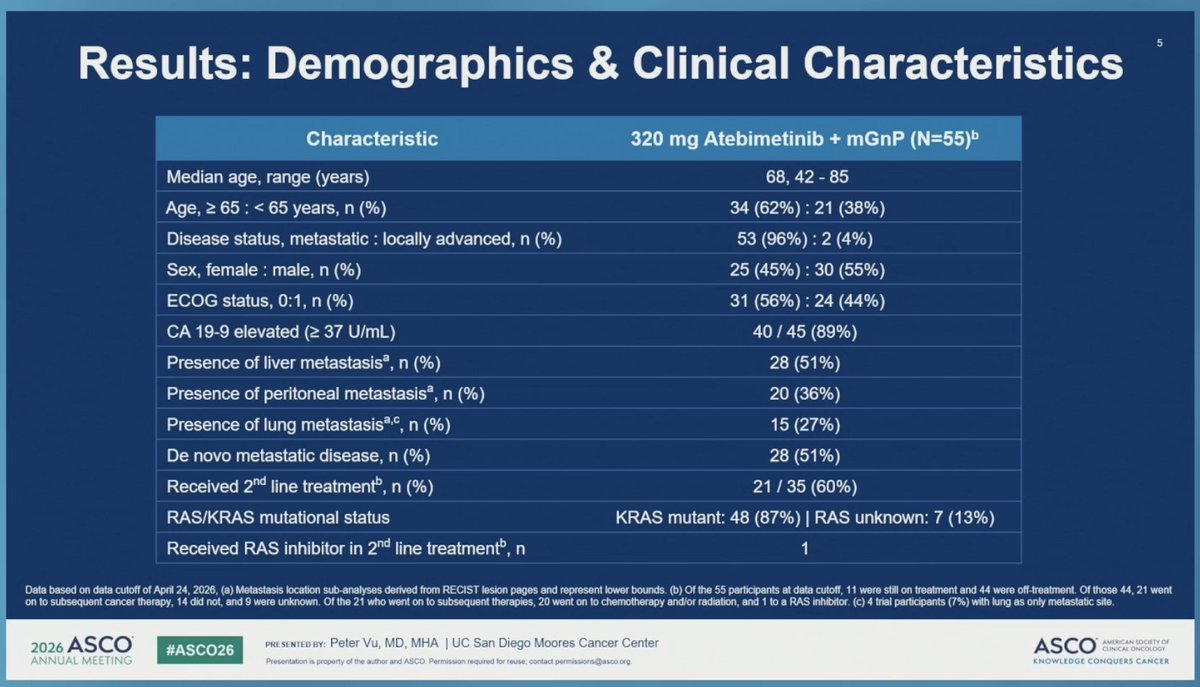
Results from a phase 2a study of atebimetinib in combination with mGnP in advanced or metastatic pancreatic cancer
👉ORR , mPFS 8.3, mOS 17.3
🧐Intersting data, targeting RAS/MEK is moving forward, phs-3 ongoing
@myesmo@ASCO
Dr. Marlana Orloff presented results from the OptimUM-02 trial of darovasertib + crizotinib in metastatic uveal melanoma
at #ASCO26 ➡️ https://t.co/gAq7mdksur
Important study re: ctDNA for non-op surveillance in rectal ca.
Pos ctDNA associated w regrowth (60%) & distant mets (60%), but neg ctDNA doesn't exclude local regrowth (sensitivity only 41%)
ctDNA good for risk stratification but not surveillance replacement #ASCO26@OncoAlert
Day 3 #ASCO26 5 plenary highlights:
1. #PROTEUS: PeriOp/PostOp Apa in Prostate Ca
2. #SARC041: Adj Abema in dediff liposarcoma
3. #LIBRETTO432 : Adj Selpercatinib in NSCLC
4. #HARMONi6: 1L Ivonescimab in Sq mNSCLC
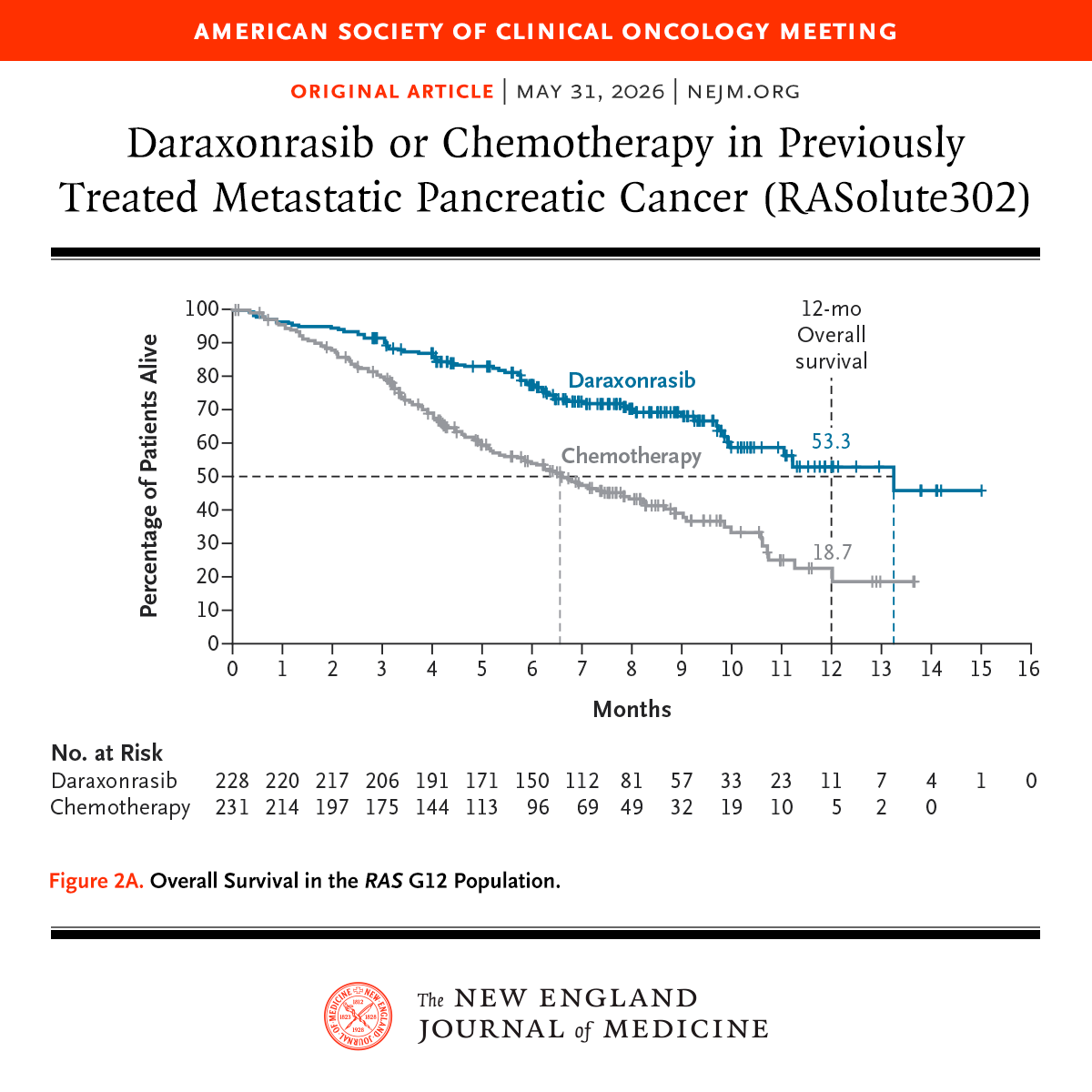
5. #RASolute302: 2L Daraxonrasib in Panc Ca
@ASCO
1/6
#EMERALD3 data at @ASCO#ASCO26
LenvaDurvaTremeTace (Arm A) vs DurvaTremeTace (Arm B) vs Tace (Arm C)
Primary end-point PFS:
🥳A better than C
😊But B also better than C
😳And A and B not so different
OS pending - promising
Tox: more drugs -> more toxicity
🤨Lenva needed?
Nilvanstomig, an anti- PD-1/TIGIT bispecific, plus beva vs. sintilimab plus beva biosimilar as 1L for advanced HCC: A randomized, multi-center, phase II trial
#ASCO26ORR
👉ORR 54 vs 50 vs 34%
👉mPFS NR vs NR vs 5.8
🧐Interesting data, supports targeting TIGIT in HCC
@myesmo@ASCOPost
“X % of patients found the side effects acceptable” strikes me as far more authentic than “manageable toxicity”, and acknowledges who’s actually experiencing the AEs!
When the patient & oncologist meet, there are 2 experts in the room: one embodied & one necessarily removed
#ASCO26@ASCO
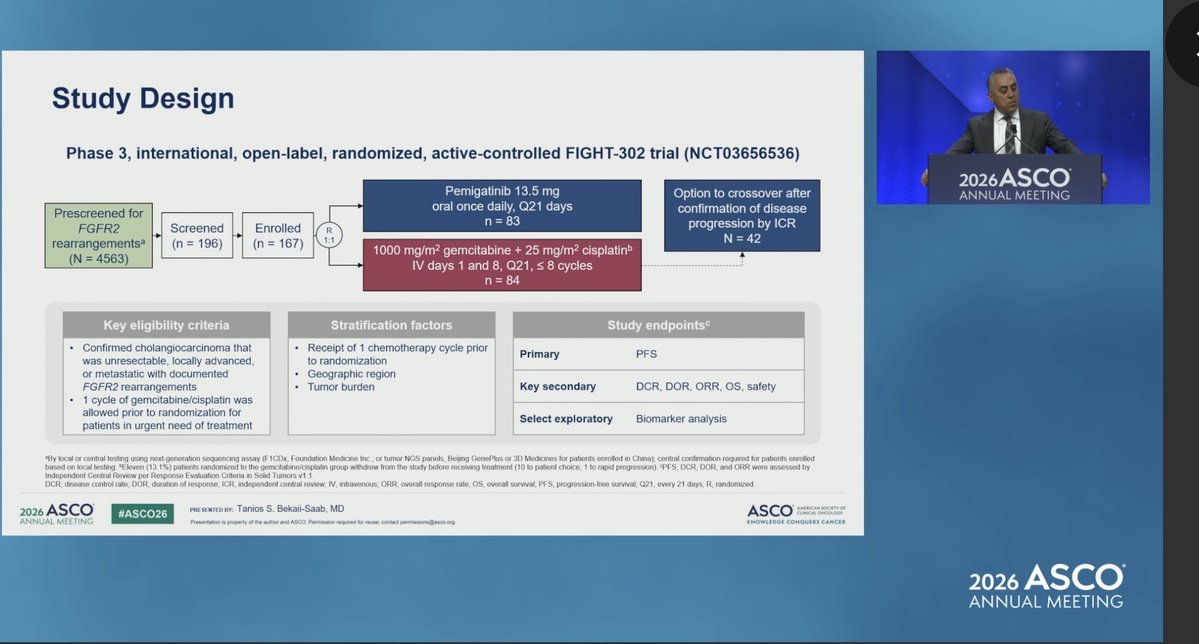
FIGHT-302 @GIcancerDoc
1L Pemigatinib vs gem/cis in FGFR2-rearranged advanced cholangiocarcinoma
Closed early d/t change in 1L SOC, n=167 (4563 screened, <4% positivity rate)
- ORR 47% vs 15%
- PFS 8.3m vs 6.8m
- no diff in OS with 50% crossover (mOS 24.4m vs 25m)
Kudos for this effort 👏
Simultaneous @JCO_ASCO publication
@OncoAlert #BTCsm
Also at @ASCO#ASCO26
CamrelizumabRivoceranibTace vs Tace
Positive in PFS; Improved ORR
Consistent findings summarised by @StephenLChan1
👉Tace better with systemic (aware of tox)
😉I would add that we must select patients to see who may be “just fine” with sequential approach
EMERALD-3:
STRIDE/Len/TACE v STRIDE+TACE v TACE #HCC#ASCO26
N=760 , prim endpoint PFS arm A v C(multiple testing)
➡️ includes BCLC A/B/C
➡️mPFS arm A v C 13.0 v 9.8 mths
➡️mPFS arm B v C 12.9 v 8.1 mths
?OS benefit? 👇Mature data needed!
@ASCO@OncoAlert
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
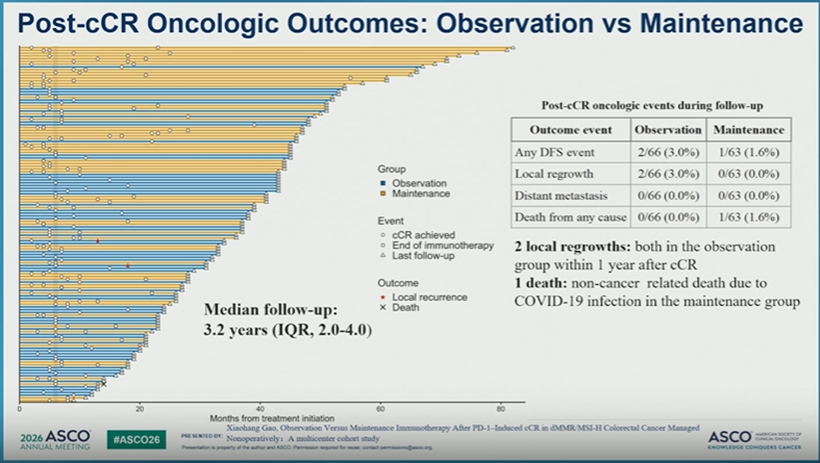
#ABS #3502 #ASCO26: Observation vs. Maintenance #PD-1 therapy after clinical complete response (cCR) in dMMR/MSI-H managed with #NOM suggesting holding IO therapy at time of cCR does not negatively impact prognosis. @ASCO#cancerresearch@OncoAlert#cancer
Pancreatic cancer treatment will never be the same again.#asco26
🎯
And
There's a lot of work that needs to be done:
- Compare with other/newer RAS inhibitors?
- How to impact early stage/resectable disease?
-How to combine with other therapy
- ideal sequence of rx?