Congratulations to @YndigegnY for a successful defence of his PhD today (1st author of REDUCE-AMI trial https://t.co/bOKP4UF07b ) at the University of Lund (I was the external examiner) with supervisors @AlexSchiopu10 and @DavidErlinge
This was a public examination with a strong defence. Thankfully Mrs Yndigegn is still inviting me to the evening dinner celebration in honour of her husband 😜
Thank you to David and Alex for hosting me in Lund with a memorable dinner last night
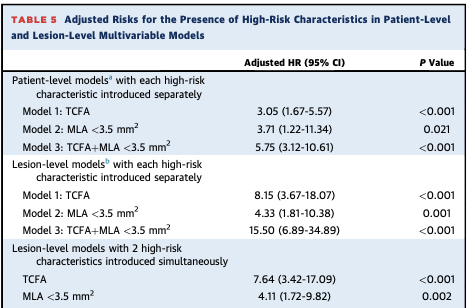
Our latest PROSPECT II pub in Circ CV Int supports a possible use for NIRS during PCI. FU stent edge–related MACE was ↑ if post-PCI stent edge maxLCBI4mm was >~100 with stent edge plaque burden >50% (adj OR 4.11). Suggests slightly longer stents to cover lipid MAY ↓MACE.
🚨INFINITY-SWEDEHEART: #DynamX® Bioadaptor meets primary endpoint and significantly reduces adverse events vs. DES after six months!
Full data: https://t.co/JHaax2X9sn
CE marked. Not for sale in the U.S.
#cardiotwitter#ESC2024
PMN 2001 REV A
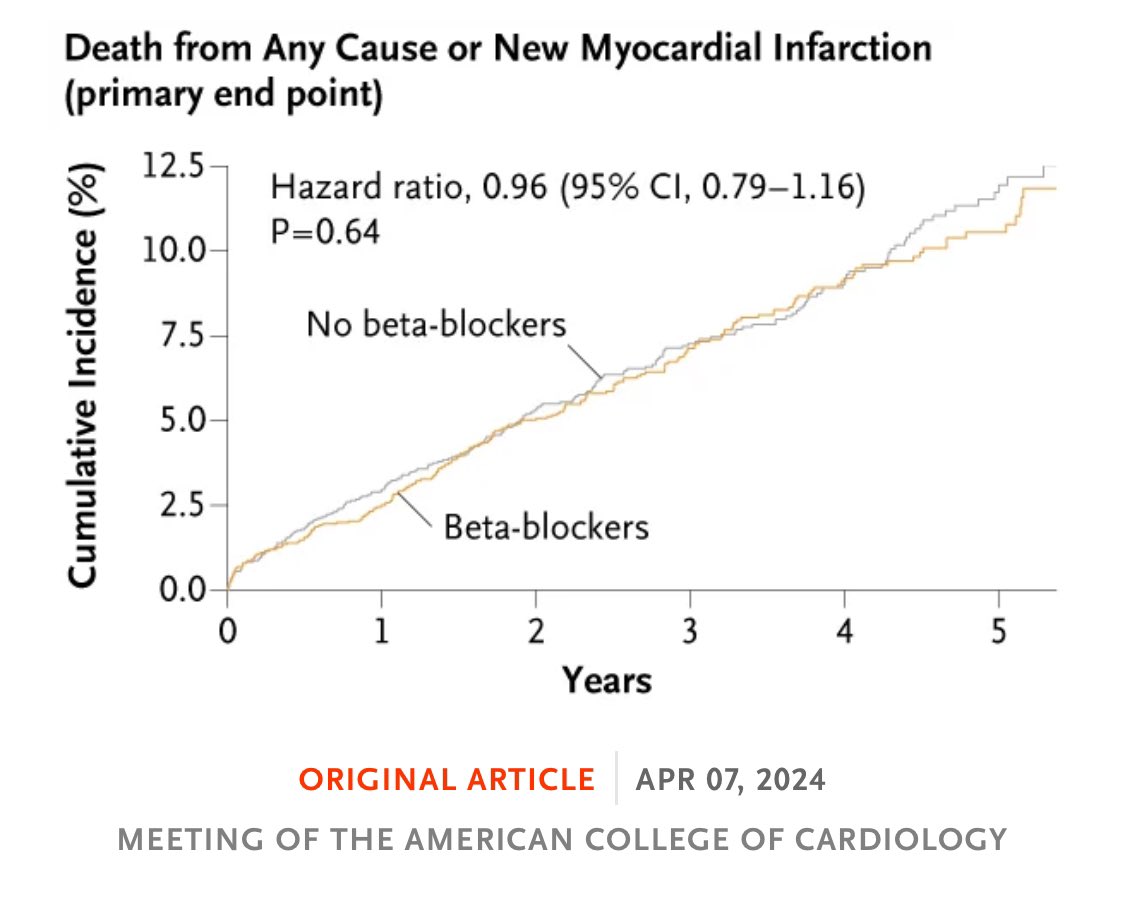
I am passionate about neutral studies, but only when their results are true negatives, not false negatives due to low statistical power. I particularly appreciate them when they eliminate drugs with seemingly routine indications but are actually poorly supported by literature or developed in an era where it was easy to beat placebo. Think of beta-blockers in REDUCE-MI. Or what is happening in the aspirin-free realm. These "x-free studies" could be a new research trend, where randomized registries have tremendous potential. Imagine a statin-free study in patients with PCSK9 inhibitors. Where is it written that we must always test drugs in addition? Couldn't we test drugs in subtraction more often?
@kaulcsmc@FrobertOle@drjohnm The REDUCE-AMI trial is the only trial powered to guide decision in post MI-patients with LV =/>50%. The KM-curves are virtually overlapping and if cross-over was supposed to affect the result one would expect an early delta which would disappear and this is not the case.
Use of AI to integrate plaque composition characteristics that increase risk for ACS
1. delta FFR across lesion
2. Plaque location & burden at site
3. Total plaque volume
4. Low attenuation plaque volume
5. Percent myocardial blood flow
Lumen narrowing not as important !!
#snackablehealth s/b HeartFlow
An area of Lp(a) research that is lacking is outcomes post PCI/CABG. Data suggests pts with ⏫ Lp(a) have worse outcomes. @hsbhatia@DavidErlinge and I outline 2 trials, one pragmatic, to assess if outcomes can be improved. TY to @LipidJournal for opportunity to share thoughts
First 3-vessel OCT imaging study publ in JACC w/long-term FU showing OCT can identify vulnerable plaques with strong discrimination. Our editorial on whether inv imaging (OCT, NIRS-IVUS, RF-IVUS) can detect VP: "Case Closed"! There are now at least 10 good studies! @ziadalinyc
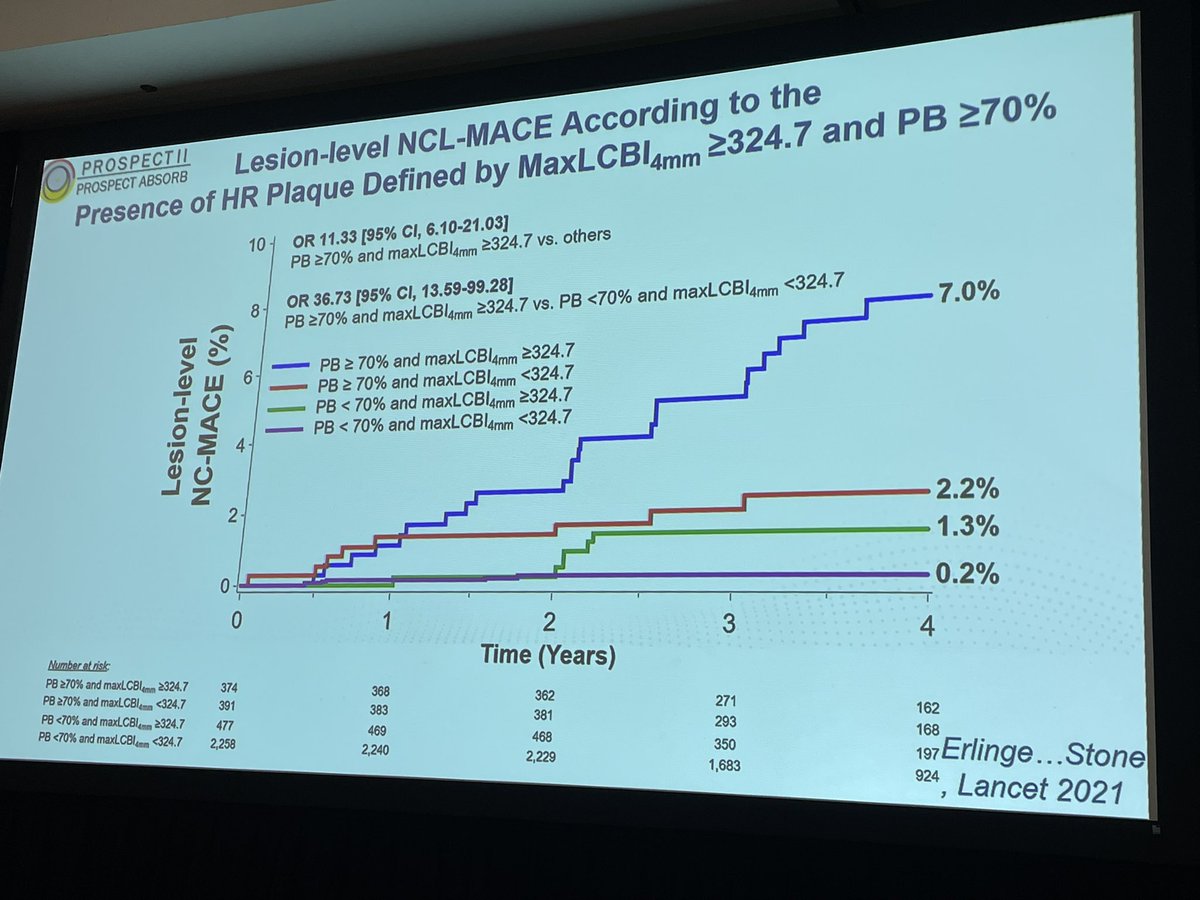
Excellent teaching by @DavidErlinge re: Biomarkers of vulnerable plaque - plaque burden, lipid content, et al- can help predict which coronary lesions will rupture @BiomarkerSymp
New SWEDEHEART study shows that using intracoronary imaging during percutaneous coronary intervention for proximal coronary artery lesions reduces the risk of target lesion revascularization and all-cause mortality
https://t.co/ibxV5pgCZr
#Cardiology#PCI#IntracoronaryImaging
10/ Conclusion: Among patients with STEMI undergoing primary PCI with radial access, bivalirudin with a median 3h post-PCI high-dose infusion reduced 30-day all-cause death and BARC types 3-5 major bleeding compared with heparin monotherapy. Published in today’s Lancet.
Coronary atherosclerosis progressed more frequently in men, in the proximal segments of the left coronary artery, and in the presence of risk factors, the relative importance of which was greater in younger patients and women.
On Natural History study of stenosis progression: Nationwide study of 248 736 patients with 2 661 245 coronary artery segments with <50% luminal stenosis, progression to ≥50% luminal stenosis within 15 years occurred in 2.6% of segments, incidence rate 1.45/1000 segment/years.