@drjohnm@djc795@JAMA_current Kindly postpone blueberry ridicule until our placebo-controlled RCT in CVD and/or T2D is published. If negative, rant freely 😎
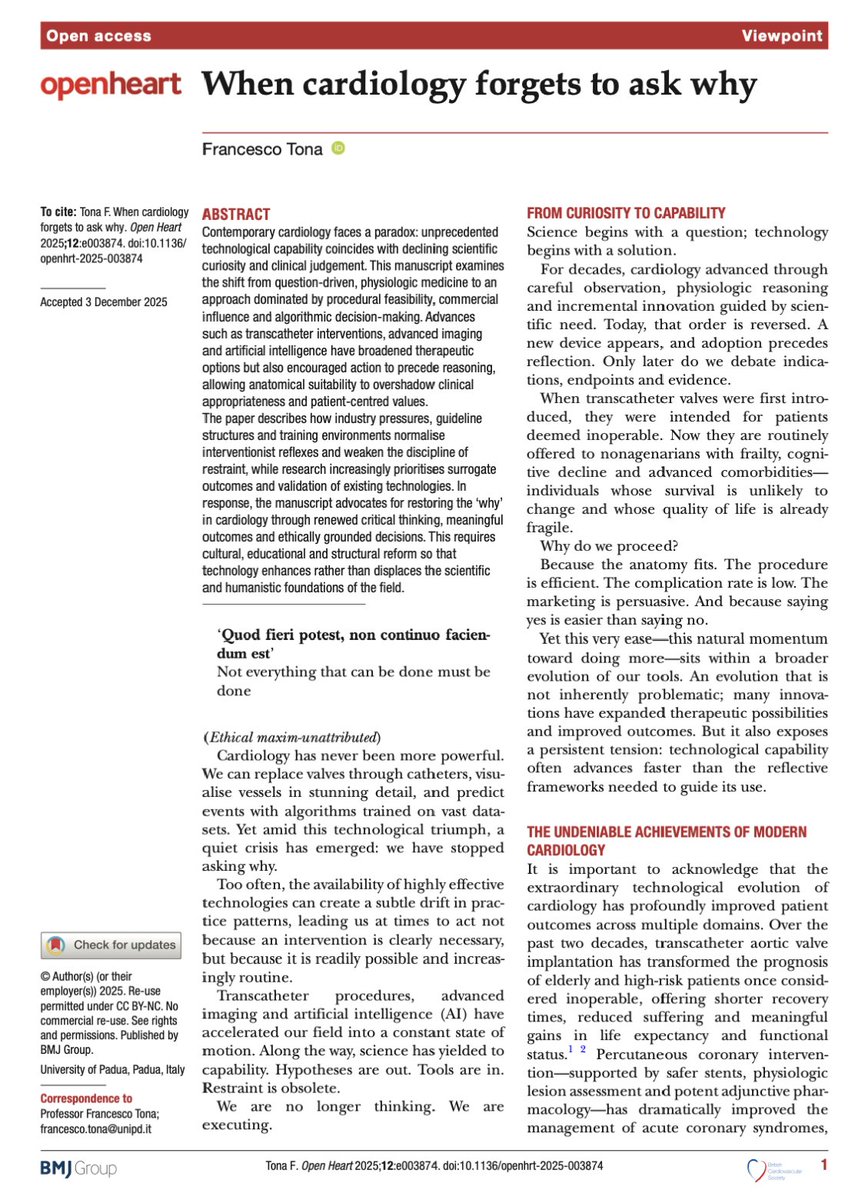
🧠🫀 When cardiology forgets to ask “why”: a timely wake-up call
This 2025 Open Heart viewpoint by Francesco Tona is not an attack on modern cardiology—but a deeply reasoned warning about what we risk losing amid unprecedented technological power .
⚙️ The paradox
Cardiology has never been more capable. We replace valves percutaneously, map anatomy in exquisite detail, and deploy AI to predict risk. Yet, the author argues, capability is increasingly replacing curiosity. Decisions are often driven by what can be done, not whether it should be done.
🧠 From “why” to “can”
Historically, cardiology advanced through physiologic questions and clinical reasoning. Today, the sequence is reversed:
- A device appears
- Anatomy fits
- The procedure proceeds
- Reflection, appropriateness, and patient-centred benefit too often come after execution—if at all.
🩺 When feasibility replaces judgement
Tona highlights a subtle but dangerous shift:
- Anatomical suitability eclipses clinical appropriateness
- Procedural success is mistaken for patient benefit
- Futility becomes “well-executed” rather than questioned
This is not failure of skill—but failure of restraint.
💼 The silent drivers
Industry influence, guideline structures, and training environments normalize interventionist reflexes. Research increasingly validates existing technologies using surrogate endpoints, while negative or null results fade into obscurity.
🤖 AI: help or shortcut?
AI can augment care—but risks outsourcing thinking. When clinicians validate algorithmic outputs instead of interrogating them, clinical reasoning atrophies. Precision without purpose is not progress.
🔮 The real message
This is not anti-innovation. It’s a call to reclaim the “why”:
Teach restraint as a clinical skill
Design guidelines around meaningful patient benefit
Prioritize outcomes that matter to patients, not systems
🧭 Bottom line
When cardiology stops asking why, it doesn’t become more efficient—it becomes less human.
Technology should serve judgement, not replace it.
Keeping up with this topic is really exhausting. Stop everything—here’s a new meta-analysis, this time in patients with myocardial infarction and preserved ejection fraction (≥50%). The first piece of news is that, after I don’t know how many years since the last cardiovascular one, it’s published in @NEJM (and yes, it’s very concise but stylish, of course). The second piece of news is that my post below, which was somewhat of a guess, turned out to be correct. Patients who have had a myocardial infarction and maintain a normal ejection fraction cannot expect any difference in mortality, reinfarction, or heart failure if they take a beta-blocker. If their ejection fraction is below 50%, however, benefits can be expected—and that is what I will do from now on. Until the next trial is published the day after tomorrow, of course. #AHA25
https://t.co/EEy72YqUaJ
Do p-tau217 levels rise without amyloid or tau aggregates? 🐻
In our Acta Neuropathologica paper, we show that 🩸 p-tau217 increases ~300% during bear hibernation, while hibernating hamsters also show ⬆️ p-tau but no changes in MTBR tau.
https://t.co/8QgRj9hfR9
@Lpa_Doc I can add brown bears to the list. Very high LDL-C (but no atherosclerosis). We wrote about it in 2012 and we are still trying to find out how they do it https://t.co/IlWaR7w0XW
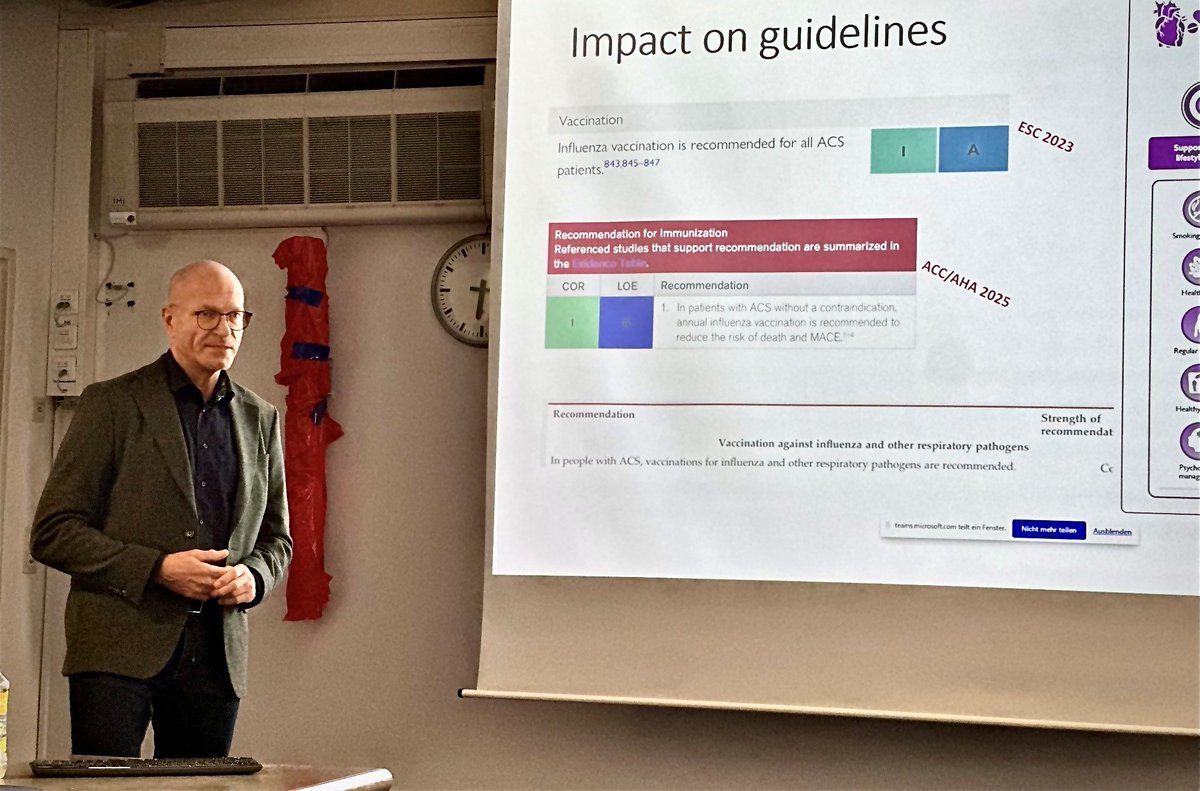
Vaccination as a new form of cardiovascular prevention: a European Society of Cardiology clinical consensus statement just published in EHJ.
https://t.co/q5m1Dqb45w
@ESCardio@ESC_Journals#vaccines
💉 Influenza vaccination as cardiovascular prevention – the evidence is growing.
Co-authored with @FrobertOle, and collegues – our new review in Atherosclerosis highlights the data behind flu shots reducing CV events.
🧠 Simple, low-cost, life-saving.
https://t.co/6J1aiEaIGu
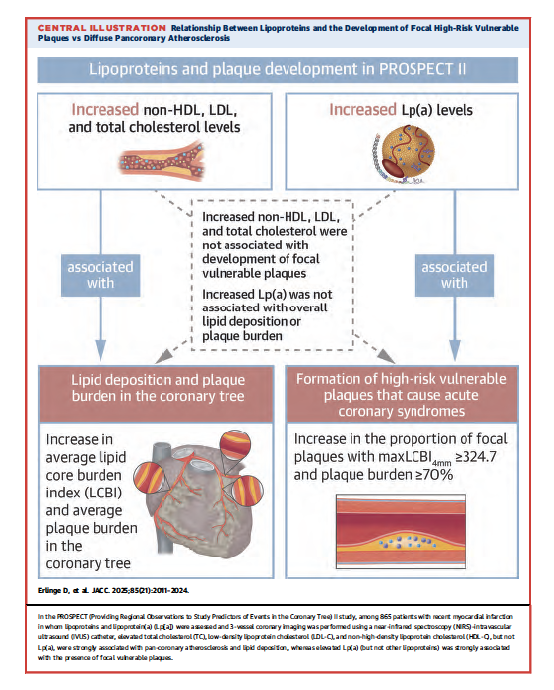
2nd new PROSPECT II publ, this in JACC Int: hs-CRP (inflammation) was independently associated with both diffuse cor plaque and lipid deposition as well as focal vulnerable plaques. Coupled with the JACC article: LDL & CRP → diffuse plaque and lipid whereas Lp[a] & CRP → VP.
We have a new Lp(a) paper, led by @derlinge from PROSPECT 2 using IVUS/NIRS. It shows high Lp(a) associates most with vulnerable plaque characteristics, whereas LDL-C with plaque burden. Lp(a) was measured by our @UCSDCardiology assay, the only Lp(a) assay I am aware of that is truly isoform-independent (uses monoclonal antibody LPA-KIV9). This study creates a rationale to perform an imaging study with Lp(a) lowering drugs and assess effect of features of high-risk plaques. https://t.co/mPgI1x202T






![GreggWStone's tweet photo. 2nd new PROSPECT II publ, this in JACC Int: hs-CRP (inflammation) was independently associated with both diffuse cor plaque and lipid deposition as well as focal vulnerable plaques. Coupled with the JACC article: LDL & CRP → diffuse plaque and lipid whereas Lp[a] & CRP → VP. https://t.co/creOqeYMJz](https://pbs.twimg.com/media/GsCvjYbWgAA41i0.png)
![GreggWStone's tweet photo. 2nd new PROSPECT II publ, this in JACC Int: hs-CRP (inflammation) was independently associated with both diffuse cor plaque and lipid deposition as well as focal vulnerable plaques. Coupled with the JACC article: LDL & CRP → diffuse plaque and lipid whereas Lp[a] & CRP → VP. https://t.co/creOqeYMJz](https://pbs.twimg.com/media/GsCvgftWYAAA9-Z.png)
![GreggWStone's tweet photo. 2nd new PROSPECT II publ, this in JACC Int: hs-CRP (inflammation) was independently associated with both diffuse cor plaque and lipid deposition as well as focal vulnerable plaques. Coupled with the JACC article: LDL & CRP → diffuse plaque and lipid whereas Lp[a] & CRP → VP. https://t.co/creOqeYMJz](https://pbs.twimg.com/media/GsCvb1wWQAAmV11.jpg)










![GreggWStone's tweet photo. 2nd new PROSPECT II publ, this in JACC Int: hs-CRP (inflammation) was independently associated with both diffuse cor plaque and lipid deposition as well as focal vulnerable plaques. Coupled with the JACC article: LDL & CRP → diffuse plaque and lipid whereas Lp[a] & CRP → VP. https://t.co/creOqeYMJz](https://pbs.twimg.com/media/GsCvjYdWsAAoinY.png)