They wanted a 50% NI margin. Ignore the fact that this is wide. They observed DEB 5.3% vs. DES 4.4%. So upper bound of margin = 2.2% increase. Their risk diff=0.91, 95% CI (-0.55, 2.38). 2.38 is >2.2 - the trial missed non-inferiority. This was a NEGATIVE trial.
Guidelines recommend dual antiplatelet therapy after CABG for acute coronary syndrome, but whether it reduces adverse events as compared with aspirin alone is unclear. Research findings from the TACSI trial are summarized in a new Quick Take video. https://t.co/zaEOWkOA5d
Our PRECISE-DAPT Cancer score now validated in a Swedish Cohort (SWEDE-Heart registry) suggesting that the majority of patients with cancer would benefit with short DAPT following ACS / PCI although a few would still benefit from prolonged therapy. We now can better better personalise care in this vulnerable population
Thank you to our swedish collaborators for leading on this @SachariasVK@moman_am@DavidErlinge@MoDafaalla
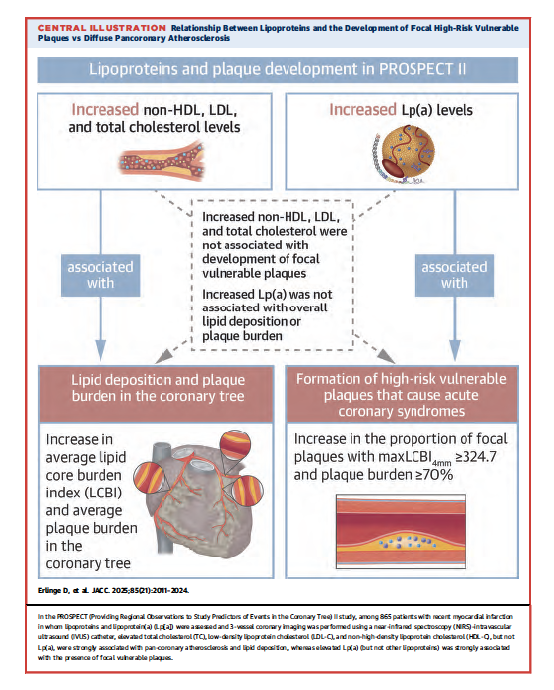
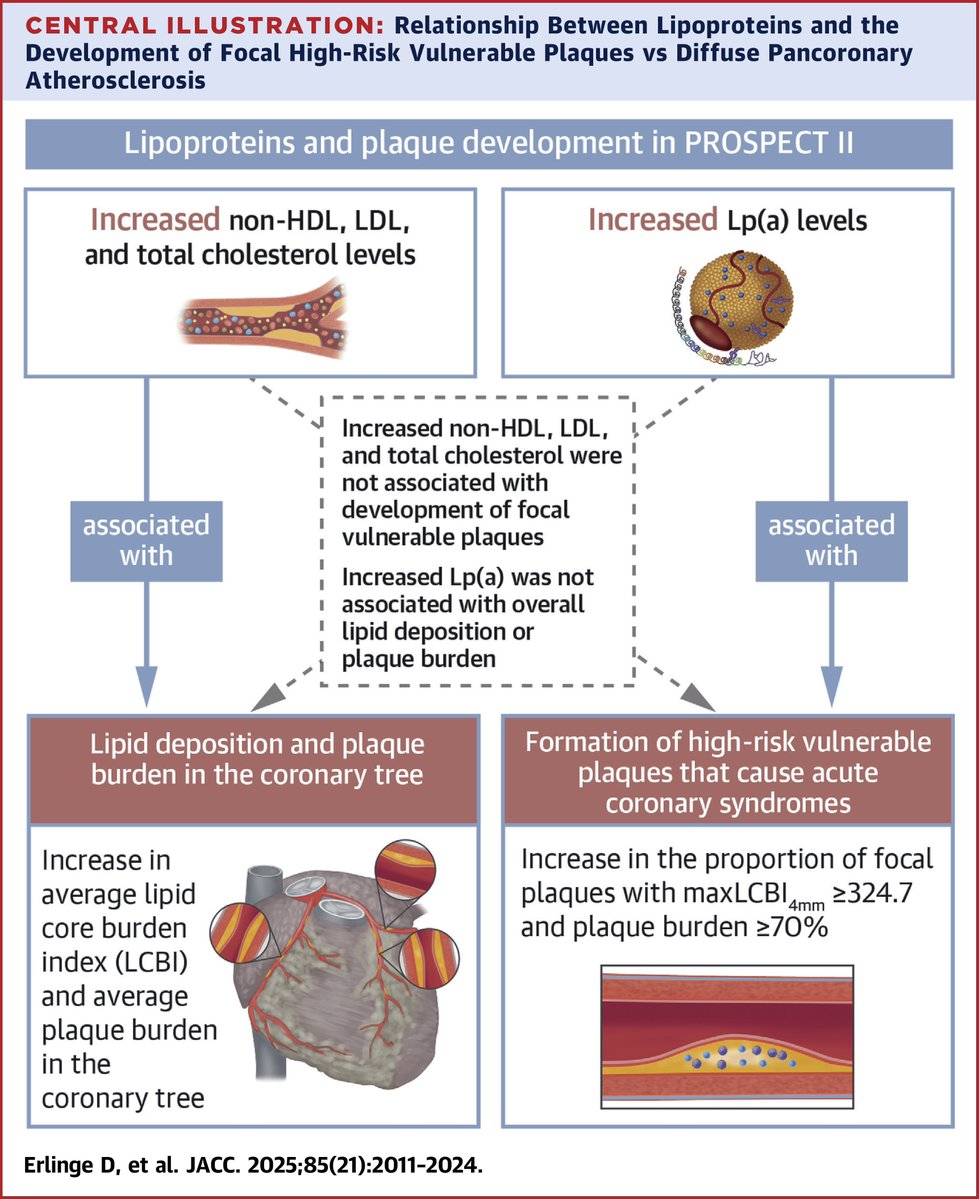
We have a new Lp(a) paper, led by @derlinge from PROSPECT 2 using IVUS/NIRS. It shows high Lp(a) associates most with vulnerable plaque characteristics, whereas LDL-C with plaque burden. Lp(a) was measured by our @UCSDCardiology assay, the only Lp(a) assay I am aware of that is truly isoform-independent (uses monoclonal antibody LPA-KIV9). This study creates a rationale to perform an imaging study with Lp(a) lowering drugs and assess effect of features of high-risk plaques. https://t.co/mPgI1x202T
In PROSPECT II, elevated TC, LDL-C, and non-HDL-C were strongly associated with pancoronary #atherosclerosis & lipid deposition, whereas elevated Lp(a) was strongly associated with the presence of focal vulnerable plaques https://t.co/nBsmNHLIqn
#JACC#ASCVD#cvAMI@GreggWStone