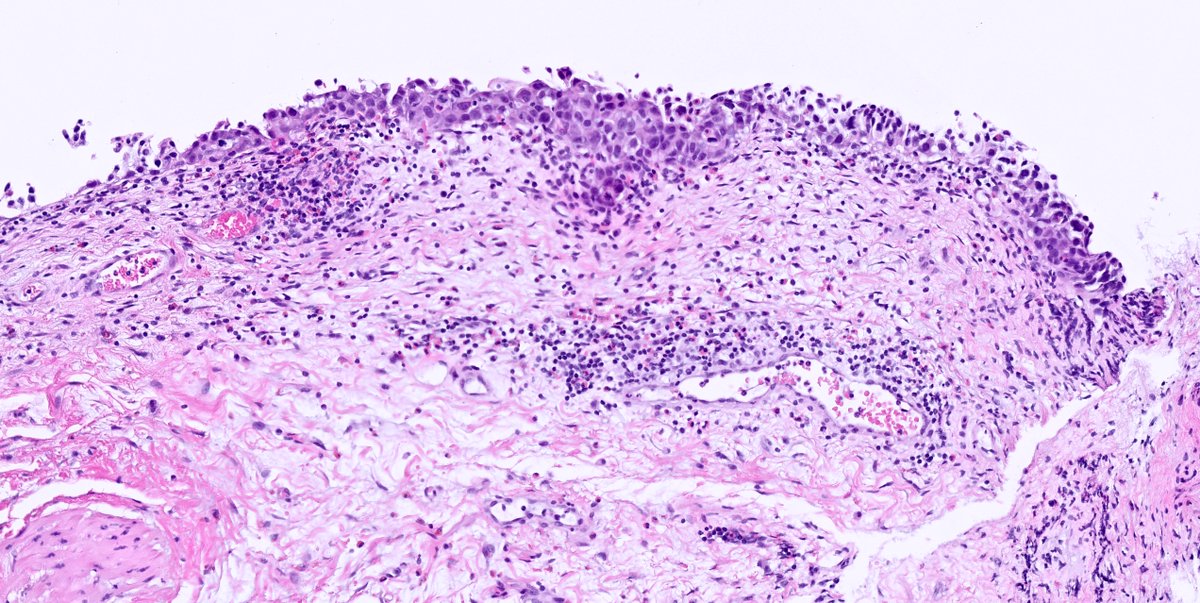
Poster Competition 2024 - p16 immunohistochemistry is used as a surrogate marker for HPV infection in cervical neoplasia. We present a rare case of cervical cytology screen-detected endocervical adenocarcinoma which was negative for p16 immunohistochemistry. #BAGP2024
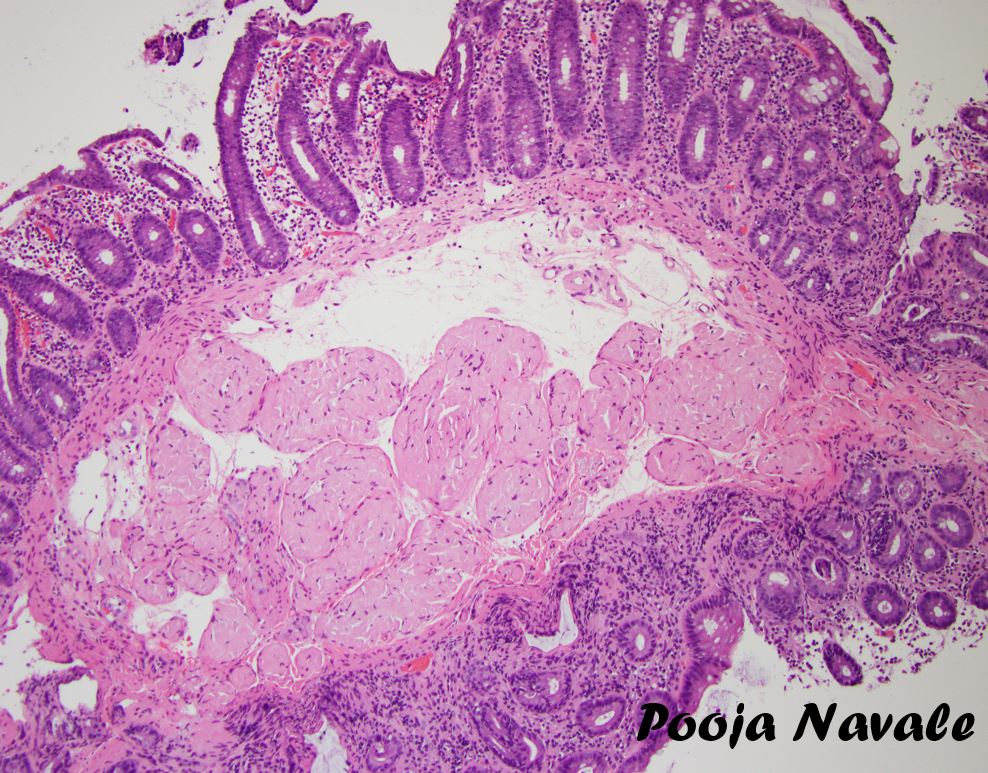
Poster Competition 2024 - Adenolipoleiomyoma is a rare lesion of the uterus composed of Müllerian-type glands, smooth muscle and adipose tissue, with only one previous case reported in the cervix. Herein we describe a case report of adenolipoleiomyoma of the cervix. #BAGP2024
Such an honor to be part of the amazing team @AceMyPath! Thank you @AkankshaGuptaMD for giving me a chance to contribute to the #GynPath section of this innovative, exceptional book "SurgPath Redefined". Looking forward to the awaited #GUPath book soon!
Please join @ISGynP for our monthly gynecologic pathology interesting case presentation! November 22, 07.00 US Eastern Time, Register at https://t.co/QD30bKwX7V #PathTwitter#GynPath#GynaePath
When digital pathology signout from home becomes a reality, will we want to drive for hours to and fro everyday (polluting on the way) just to spend hours at work away from our families? Will we still want to commute to work and sit in an office for 8-10 hours?
Thank you all for your comments. As I expected, the responses were mixed, but ADH was a clear winner in the first case, in part driven by the need and recommendations to be more conservative in our core biopsy diagnoses, and in part because of the presence of two cell populations, the background columnar cell hyperplasia and the overlying (what I like to call) bridging micropapillary atypical proliferation. DCIS was more popular in the second case, because of the presence of contiguous spaces with complete involvement. The size was right at 2 mm though. To be sure, both cases made me pause and carefully consider ADH and DCIS options at length, but I did eventually opt for ADH.
Below, I will detail how I have come to consider ADH in a way that brings a little clarity and understanding to my thought process. It is of course based on the general criteria advanced by David Page in his seminal "Cancer" paper from 1985.
1. Atypical hyperplasia is not really a small DCIS. In his original paper, David Page says that ADH is a lesion that has some but not all the characteristics of DCIS, and because the definition of DCIS he previously put forth stated that the proliferation had to be uniform, completely involve two contiguous spaces, and measure more than 2 mm in diameter, it followed that ADH would be characterized by smaller size, incomplete involvement of spaces, complete involvement of a single space, and a uniform subpopulation of cells. The problem with this definition is that it could imply that atypical ductal hyperplasia is merely an early form of DCIS which, if given time, would evolve into full-fledged DCIS. Although that may be the case in some instances, instances which we cannot in my opinion morphologically discern, it goes against the risk model that was also introduced by David Page which states that the risk of subsequent invasive carcinoma for DCIS is ipsilateral and geographically concordant with the biopsy site, while the risk of subsequent invasive carcinoma following ADH is bilateral and comparable in both breasts. if these two lesions were one and the same but at different stages of development, then the contralateral breast cancer risk should be identical. The fact that it isn't suggests a fundamental difference between ADH and DCIS. I view this fundamental difference's morphological manifestation as follows: While DCIS arises from a single clone that starts in a lobular unit, completely involving it and spreading to adjacent lobular units through intervening ducts (hence the complete involvement of two adjacent spaces over a span of >2 mm), ADH is more akin to mushrooms arising over a widespread mycelium, the mycelium generally representing different varieties of columnar cell change. In other words, while usual ductal hyperplasia is a polyclonal proliferation of cells with a variety of phenotypes, and while DCIS is a single neoplastic clone, ADH is multiple small separate clones on a backdrop of columnar cell change. The one exception that most readily blurs the line between ADH and DCIS would then be micropapillary ADH versus micropapillary DCIS, as micropapillary DCIS can still have columnar cell change in the background and still be extensive with a strong propensity for invasive disease.
2. Aside from this fundamental difference between ADH and DCIS, disease volume plays an important role in the likelihood of clonal proliferations progressing to invasive cancer. Let me take this opportunity to make a disclaimer that is both controversial and potentially aggravating to some. All clonal proliferations in the breast are non-obligate precursors for invasive breast carcinoma. I say this with extreme conviction even in the face of an onslaught of criticism and denial. It is but a game of probabilities. The most basic and innocuous of atypical lesions, namely flat epithelial atypia, will occasionally give rise to tubular carcinoma. ADH not meeting criteria for DCIS will occasionally give rise to low-grade invasive carcinoma. These are rare events because the likelihood of an invasive outcome is proportional to the volume of precursor disease and its mutational burden. In that vein, the reason I was considering low-grade DCIS for the case pictured below is because of the sheer volume of atypia present in the many involved spaces. Computing the risk based on cellular features and volume of disease is of course impossible with our current knowledge and techniques, but knowing that we live in an age of de-escalation of therapy, and that limited examples of DCIS that are excised to widely negative margins are unlikely to cause any future harm to the patient, adopting a conservative stance with borderline lesions such as this one is probably the way to go.
3. Finally, and to conclude this relatively brief
and simplified discussion of a highly complex topic, I suggest being conservative with the diagnosis of DCIS when intermediate to high-grade cells are present in a small area, despite the guideline that high-grade DCIS does not need to fulfill size criteria for diagnosis. If high-grade cells are present in small numbers and not completely filling spaces, I use the somewhat vague and non-committal designation "atypical intraductal proliferation" to prompt excision without subjecting the patient to a permanent diagnosis of DCIS before proving a substantial extent of disease and true potential benefit from adjuvant therapy.
Voila. Hope you all have an Xcellent weekend!
@wusm_pathology @washupathedu #breastpath #PathTwitter #PathX #pathology
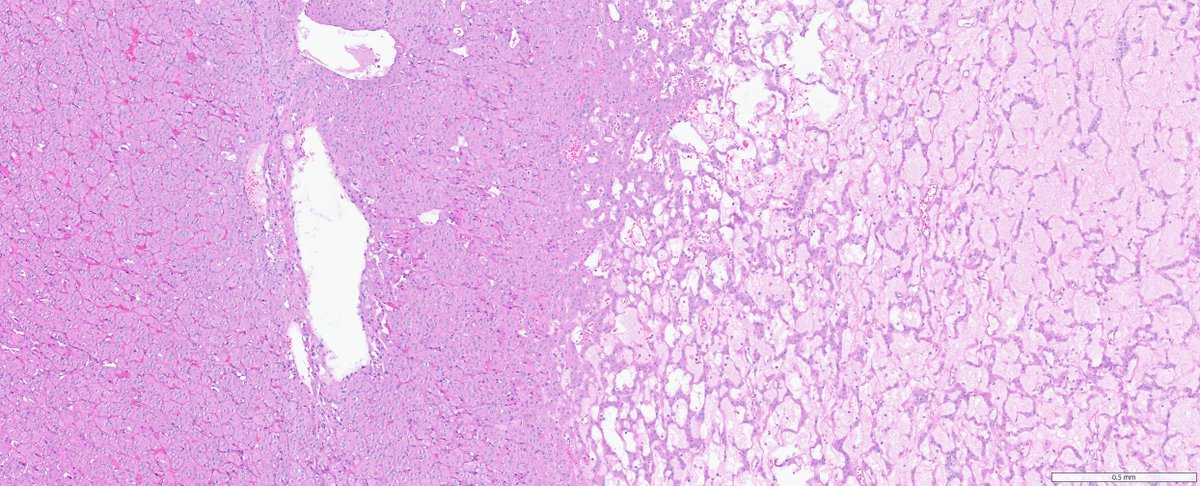
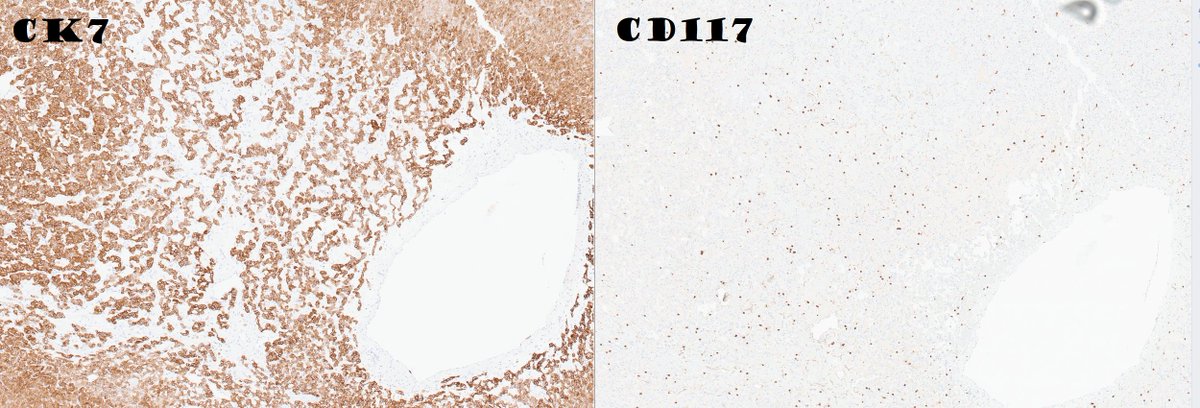
F 60ish. 2 cm polypoid uterine tumour.
Myoinvasion present.
What are your potential differential diagnoses, and which tests would you like to perform?
#pathtwitter#Gynpath#frcpath#bagp